
Abstract
Abstract
Purpose:
The purpose of this study was to report a patient with choroidal and optic disc metastases from breast cancer and the response to combination pharmacotherapy with tamoxifen, cyclophosphamide hydrate, letrozole, and bevacizumab.
Methods:
We report a case of a 51-year-old woman with a medical history of breast cancer treated with mastectomy at 16 years earlier followed by 5′-deoxy-5-fluorouridine and tamoxifen for 12 years, who has been followed by annual check-up, with no additional findings. Two weeks prior to her first visit to our hospital, she noted blurred and abnormal color vision and field loss in her right eye. Her right eye showed choroidal metastasis from breast cancer, with retinal detachment involving the macula and inferior periphery.
Results:
Multiple metastases involving bones, lymph nodes in the mediastinum, ovaries, and pelvic nodes were diagnosed after ocular metastases were established. Combination therapy with tamoxifen, cyclophosphamide hydrate, letrozole, and bevacizumab was administered to the patient. The retinal detachment and optic disc metastasis improved dramatically.
Conclusions:
The patient underwent combination pharmacotherapy with tamoxifen, cyclophosphamide hydrate, letrozole, and bevacizumab, which was effective in the treatment of ocular metastases from breast cancer.
Introduction
Case Report
A 51-year-old woman presented to the emergency room complaining of blurred and abnormal color vision and also field loss in her right eye over a period of 2 weeks. She had been diagnosed with infiltrating ductal carcinoma in her right breast T2N1M0 16 years earlier and treated with mastectomy, 5′-deoxy-5-fluorouridine, and tamoxifen for 12 years. Estrogen receptors were positive in the tumor. For the last 4 years, she had annual medical check-ups by medical interview, mammogram, and blood test not including tumor markers; however, no abnormalities had been pointed out by the check-ups.
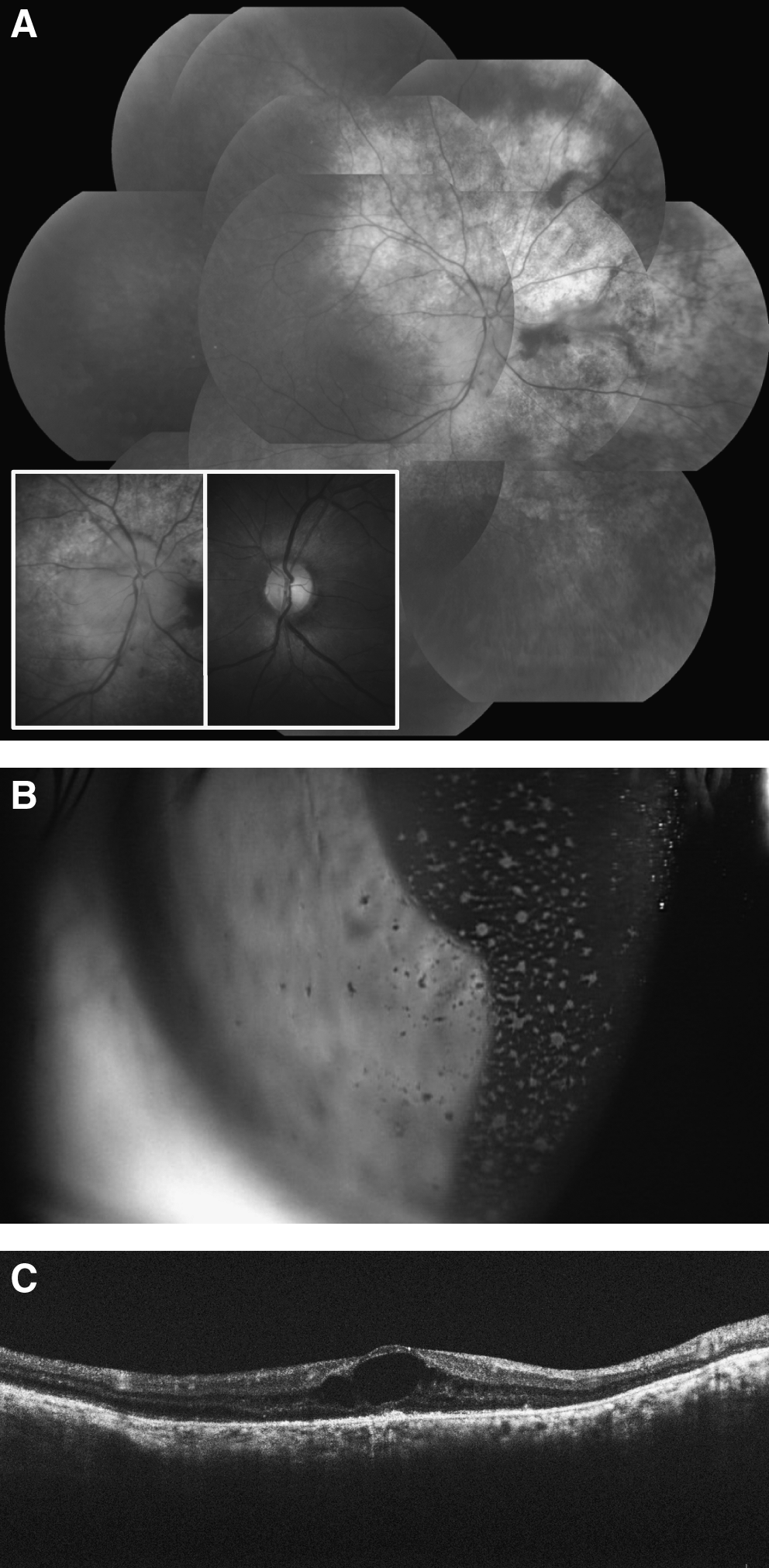
Ocular evaluation revealed a best-corrected visual acuity of 0.5 in the right eye and 1.0 in the left eye. The anterior segment was normal in both eyes. Fundus evaluation revealed a yellow subretinal plaque lesion superonasal to the optic disc of the right eye (Fig. 1A, arrows). Fundus fluorescein angiography revealed a broad blockage of choroidal fluorescein superonasal to the optic disc by the subretinal plaques (Fig. 1B). Optical coherence tomography demonstrated subretinal fluid in the fovea (Fig. 1C). In view of her history of operated breast cancer and of the clinical appearance of the lesion and fluorescein angiography, a diagnosis of right choroidal metastasis from breast cancer was suspected. The patient was referred back to her oncologist to establish her diagnosis and treatment. A detailed systemic examination disclosed multiple metastases from breast cancer involving bones, lymph nodes in the mediastinum, ovaries, and pelvic nodes in accordance with an elevated CA15-3 level.

Fundus evaluations of the patient's right eye on her first visit.
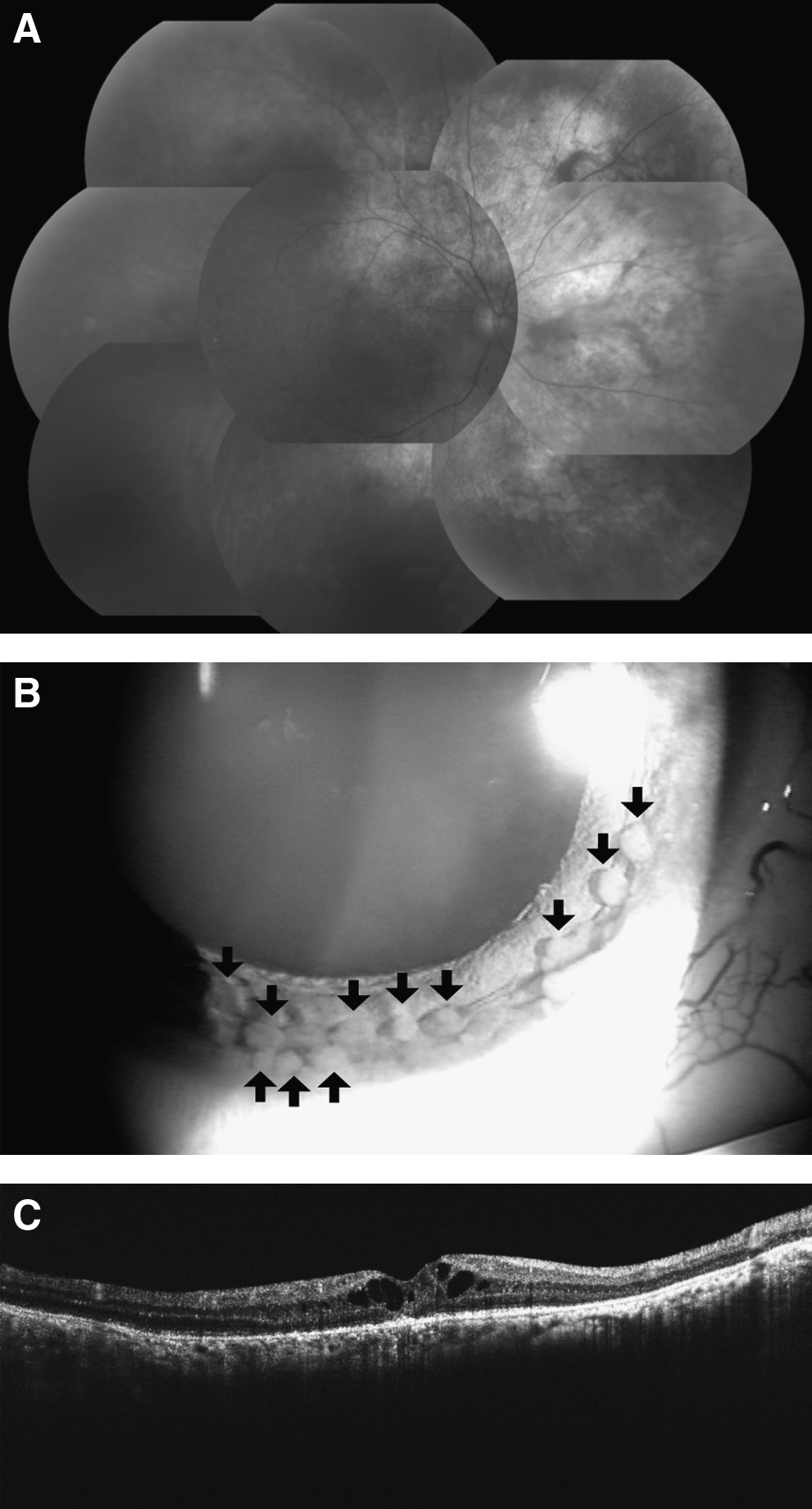
The best-corrected visual acuity in the patient's right eye was 0.3 at 3 weeks after her initial visit; concomitantly, an exudative retinal detachment of the right eye was noted (Fig. 2A, arrows). The patient subsequently underwent combination therapy with tamoxifen and cyclophosphamide hydrate. Nine months after introduction of therapy, regression of retinal detachment involving the inferior periphery was achieved and the CA15-3 level was normalized. However, an optic disc metastasis was found (Fig. 2B, arrows) and the subretinal fluid in the fovea showed no improvement. We applied bevacizumab by intravitreal injection in an attempt to relieve the lasting subretinal fluid in the fovea. Three weeks after bevacizumab application, the subretinal fluid in the fovea improved significantly (Fig. 2C).

Retinas before and after combination tamoxifen, cyclophosphamide hydrate, and bevacizumab therapy.
Eight months after the subretinal fluid in the fovea improved, the metastasis at the optic disc became more evident (Fig. 3A, in the box), although the patient was not conscious of any symptoms. The best-corrected visual acuity in the right eye was 0.05. Further, mild anterior chamber inflammation with pigment keratic precipitates appeared (Fig. 3B), and betamethasone sodium phosphate was applied as eye drops twice a day for 2 months. Cystoid macular edema appeared 2 years after the initiation of tamoxifen and cyclophosphamide hydrate combination therapy (Fig. 3C).
The right eye at 17–24 months after the initiation of a combination therapy.
Because the patient was postmenopausal, tamoxifen plus cyclophosphamide hydrate combination therapy was terminated, but was followed by a daily dose of letrozole (2.5 mg). Five months after the initiation of letrozole therapy, the optic disc lesion resolved (Fig. 4A). Finally, the loosely cohesive cells in the anterior chamber settled on the nasal to inferior iris and appeared as giant iris nodules (Fig. 4B, arrows). Cystoid macular edema was moderately reduced at 6 months after the termination of tamoxifen therapy (Fig. 4C).
The right eye after letrozole treatment.
Discussion
Exudative retinal detachment was demonstrated in this patient and was successfully improved by a combination of tamoxifen as an endocrine treatment and cyclophosphamide hydrate as a cytotoxic chemotherapy. Previous reports have indicated that exudative retinal detachment may be associated with breast cancer metastasis3,4; in these cases, no ocular surgical treatment was required. Letson et al. reported favorable chemotherapy results when treating choroidal metastases from breast carcinoma, 5 and recently, Demirici demonstrated an 81% uveal metastasis control rate after systemic chemotherapy. 1 Owing to detailed investigation by the oncologist, a correct diagnosis was immediately established in the present case, and appropriate therapy was applied to the patient in a timely manner. Regarding the differential diagnosis, serous retinal detachment accompanied by posterior uveitis (such as Harada disease or uveal effusion syndrome) should be excluded, although the subretinal plaque observed in this case is unusual in such disorders.
Optic nerve involvement may be the result of either metastatic emboli deposited in the microcirculation of the papilla or the direct extension of an adjacent choroidal tumor. 4 We believe the latter mechanism is more likely in this patient. Interestingly, the initial choroidal plaque, superonasal to the optic disc, was significantly reduced, but the optic disc lesion gradually enlarged under the combination of tamoxifen and cyclophosphamide hydrate. It is unclear why these two metastatic lesions had opposite responses to the same therapy. We speculate that inflammatory reactions modified these metastases, and thus the anti-inflammatory effect by the therapy may be different. Further, different drug circulation depending on anatomical location may be involved in the antithetic processes. However, we concluded that the optic nerve lesion is a metastatic breast cancer lesion without histological evidence, as it disappeared after the initiation of letrozole therapy.
Tamoxifen, a selective estrogen receptor modulator, is generally well tolerated and has a favorable therapeutic index. However, tamoxifen also has ocular toxicity. Tamoxifen-induced optic neuritis 6 was suspected at the initial appearance of this patient's optic disc metastasis, because the patient had already undergone tamoxifen therapy for 9 months. Further, it is likely that the cystoid macular edema observed in this patient may be involved in tamoxifen retinopathy, 7 as the lesion was improved by the termination of tamoxifen despite the anterior uveitis accompanied by giant nodules on the iris. However, the cystoid macular edema might be associated with uveitis induced by breast cancer metastases.
A few reports have described the efficacy of letrozole in patients with choroidal breast cancer metastasis.8,9 In the present study, letrozole drastically reduced the metastasis at the optic disc; and as far as we know, this is the first such case reported in the literature.
The decrease of subretinal fluid in the fovea after the injection of bevacizumab into the vitreous cavity may indicate that vascular endothelial growth factor was involved with the condition in this case. Many reports have demonstrated that systemic bevacizumab is an effective treatment for systemic breast cancer metastases. Amselem et al. recently described the beneficial effect of a single intravitreal injection of bevacizumab in a patient with choroidal metastasis secondary to breast cancer. 10 In the present case, intravitreal injection of bevacizumab may have contributed to improvement in choroidal metastasis as well as in the subretinal fluid in the fovea.
Metastases to the ciliary body or iris are often involved in secondary glaucoma by invading the iris root and trabecular meshwork, which may not respond to medical treatment.4,11 In the present case we observed iris nodules (Fig. 4), which are not a typical aspect of ocular breast cancer metastasis. The present ocular condition in this case has been stable; however, we will consider additional therapy in case of enlargement of the ocular metastases or progression to glaucoma (such as external beam radiotherapy or additional intravitreal injection of bevacizumab, depending on the patient's preference).
Footnotes
Author Disclosure Statement
No competing financial interests exist.