
Abstract
Abstract
Purpose:
This study evaluated the ocular pharmacokinetics of indomethacin following topical administration of two different formulations present in the market.
Methods:
Rabbits received a multiple topical instillation (30 μL) of indomethacin ophthalmic suspension containing hydroxypropylmethylcellulose (IND-HPMC; Indom™ Alfa-Intes) or indomethacin ophthalmic solution with hydroxypropyl-β-cyclodextrin (IND-CD; Indocollirio™ Bausch & Lomb). Aqueous humor, vitreous humor, and retina were collected from animals at fixed time intervals after dosing. Indomethacin ocular levels were measured by liquid chromatography mass spectrometry (LC-MS/MS), and the pharmacokinetic parameters—peak drug concentration (Cmax), time to peak value (Tmax), and area under the concentration–time curve between 0 and 240 min (AUC0–240)—were determined. All of the animals were treated according to the Association for Research in Vision and Ophthalmology (ARVO) Statement for the Use of Animals in Ophthalmic and Vision Research.
Results:
Peak concentrations of indomethacin in aqueous and vitreous were achieved within 30 min and 60 min after a single instillation of IND-HPMC and IND-CD, respectively. Retinal Tmax was 30 min and 120 min in the IND-HPMC-treated group and the IND-CD-treated group, respectively. Higher levels of indomethacin were found in retina after IND-HPMC administration compared to IND-CD (AUC0–240 272.9 ng/g per min vs. AUC0–240 73.5 ng/g/min, respectively; P<0.01). Also in the aqueous and vitreous, the drug levels were statistically higher (P<0.01) in the IND-HPMC group in comparison with the IND-CD group (AUC0–240 2039 ng/mL per min vs. AUC0–240 427.3 ng/mL per min, AUC0–240 53.8 ng/mL per min vs. AUC0–240 12.5 ng/mL per min, respectively). The highest drug levels in the ocular tissues were found following IND-HPMC administration compared with IND-CD (retina: Cmax 73.7±6.4 ng/g vs. 25.5±1.73 ng/g; aqueous: Cmax 952±6.8 ng/mL vs. 163±4.1 ng/mL; vitreous Cmax 31±3.5 ng/mL vs. 6.37±3.6 ng/mL).
Conclusions:
IND-HPMC treatment demonstrates a nonclinical ocular pharmacokinetic profile of indomethacin characterized by higher concentrations of drug in ocular tissues (4.7-, 4.3- and 3.7-fold higher in aqueous, vitreous, and retina, respectively) compared to the ND-CD-treated group. Taken together, these data seem to indicate that IND-HPMC formulation has good ocular distribution reaching relevant indomethacin levels in the back of the eye, and suggest that this formulation may be very useful for clinicians to manage retinal conditions.
Introduction
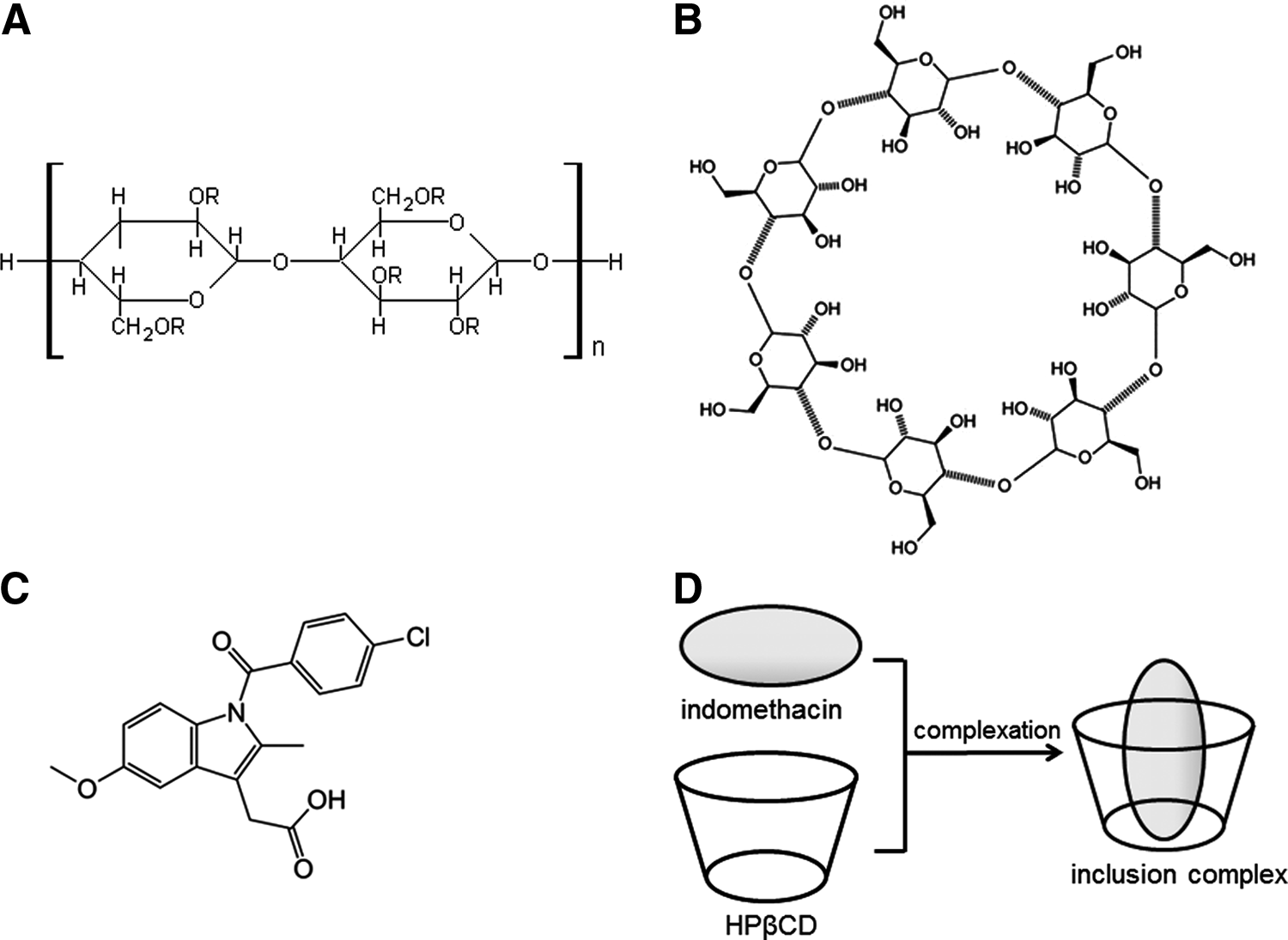
Structures of hydroxypropylmethylcellulose (
Several ocular diseases, such as diabetic retinopathy or age-related macular degeneration (AMD), have an underlying inflammatory component that results in macular edema. NSAIDs are potent inhibitors of cyclooxygenase (COX) enzymes, and thereby the synthesis of prostaglandins (PGs). In the eye, PGs cause vasodilatation, disruption of the blood–ocular barrier, and leukocyte migration; consequently, their inhibition by COX inhibitors may have therapeutic effects. In fact, numerous studies have demonstrated that NSAIDs are beneficial in diabetic retinopathy1–5 and age-related macular degeneration.6–9 Accumulating evidence suggests that COX-2 has important therapeutic implications in retinal diseases. 10 Indomethacin is a nonselective COX-2 inhibitor, even though this molecule can act via a COX-2-independent pathway. An important work by Zhang et al. 11 demonstrated that this molecule reduced mammalian target of rapamycin (mTOR) signaling activity. This observation is particularly relevant because mTOR signaling is implicated in the neoangiogenesis that occurs in many intraocular inflammatory diseases such as uveitis, AMD, and diabetic retinopathy.
The aim of the present study was to evaluate the ocular pharmacokinetics of indomethacin following multiple topical administration on the rabbit eye of two different formulations present in the European market to better understand which formulation is able to achieve consistent levels of drug in the back of the eye. To evaluate the distribution of indomethacin through the ocular tissues, the drug was determined by liquid chromatography mass spectrometry (LC-MS/MS).
Materials and Methods
Animals
White New Zealand rabbits weighing approximately 2–2.2 kg were obtained from Charles River (Calco, Italy). All the animals were treated according to the Association for Research in Vision and Ophthalmology (ARVO) Statement for the Use of Animals in Ophthalmic and Vision Research, and according to the European Guidelines for the Care and Use of Laboratory Animals (2010/63/EU). The animals were fed on standard laboratory food and were allowed free access to water in an air-conditioned room with a 12-h light/12-h dark cycle.
Experimental procedure and sample collection
Rabbits were randomly divided in two groups. A multiple treatment (30 μL/eye; four times in 8 h) was performed with Indom™ (Alfa-Intes; ophthalmic suspension containing 0.5% indomethacin+hydroxypropylmethylcellulose; IND-HPMC) or Indocollirio™ (Bausch & Lomb; ophthalmic solution containing 0.1% indomethacin+hydroxypropyl-β-cyclodextrin; IND-CD) eye drops. After the last instillation, aqueous humor, vitreous, and retina were collected from animals at fixed time intervals (30, 60, 120, and 240 min). Animals were killed by Tanax® (0.3 mL/kg intravenously [i.v.]; Intervet Italia, Milano), and ocular tissues collected. Samples were stored at −20°C and then processed for analysis.
LC-MS/MS analysis
Aliquots of vitreous humor, aqueous humor, and retina were spiked with diclofenac as internal standard (IS) in water/acetonitrile (50:50, vol/vol). Vitreous and aqueous samples were extracted with ethyl acetate. Retinal samples were added to 500 μL of ammonium acetate buffer (20 mM, pH 7.2), homogenized, and then extracted with ethyl acetate. After vortex mixing for 10 min and centrifugation at 4100 rpm at+4°C for 15 min, aliquots of 2.5 mL of the organic phase were transferred into a single glass tube and dried under vacuum at 50°C using a Büchi vacuum system. The residues were reconstituted with water/acetonitrile. The tubes were then vortex mixed and centrifugated.
The final extracts were transferred into an autosampler vial, and 5 μL were injected into the LC-MS/MS system. A Phenomenex Gemini-NX column (2.0×50 mm, 3 μm, C18) was used to perform the chromatographic analysis under gradient conditions at a flow rate of 0.2 mL/min. Retention times of indomethacin and IS were about 2.36 and 2.44 min, respectively. Total cycle time was 5 min. MS detection used an Agilent Technologies 6410 Triple Quadrupole LC/MS with atmospheric pressure ionization/electrospray ionziation (API/ESI) source and multiple reaction monitoring (MRM) (358→139 mass-to charge [m/z] for indomethacin, 296→215 m/z for IS) operated in the positive ion mode. Calibration curves were constructed by plotting the ratio of the area of the compound and the IS (y) against the analyte concentration (x). A weighted linear regression function (1/x2) was used to fit calibration lines and consequently to calculate indomethacin concentrations. The lower and upper limits of quantification for indomethacin were 1 ng/mL and 200 ng/mL for aqueous and vitreous humor samples and 1 and 200 ng/g for retinal samples.
Pharmacokinetic analysis
Indomethacin concentrations in the aqueous, vitreous, and retina were plotted versus time after topical administration. Peak drug concentration (Cmax), time to peak value (Tmax), area under the concentration–time curve between 0 and 240 min (AUC0–240) were obtained. Values represent the mean±standard deviation (SD) of four to six samples. Graphs and data were processed by GraphPad Prism 5 software (GraphPad Software, San Diego, CA). AUC0–240 values were calculated using the trapezoidal rule. Statistical comparisons were made by the Student t-test for interval variables. Statistical significance was accepted at a level of P<0.05.
Results
The mean indomethacin concentrations in the aqueous, vitreous, and retina at different time intervals after instillation are shown in Fig. 2. The key parameters of such concentration–time curves (Cmax, Tmax, and AUC0–240) are shown in Table 1. Peak indomethacin concentration was achieved within 30 min and 60 min in the IND-HPMC-treated group and IND-CD-treated group, respectively, for all tissues except for the retinas obtained from IND-CD-treated group, where the peak was achieved within 120 min. Highest levels concentration of drug were found in the aqueous with Cmax of 952 and 163 ng/mL, and AUC0–240 of 2039 and 427 ng/mL per min for IND-HPMC and IND-CD, respectively. Significant (P<0.01) levels of indomethacin were found in retina in the IND-HPMC-treated group (Cmax 73 mg/g; AUC0–240 272.9 mg/g per min) compared with the IND-CD-treated group. Also in the vitreous, the levels of indomethacin were significantly higher in the IND-HPMC-treated group in comparison with the IND-CD-treated group (AUC0–240 53.8 mg/g per min and AUC0–240 12.5 mg/g per min, respectively). In the group treated with IND-HPMC, aqueous and retinal levels of indomethacin were significantly higher (P<0.05; P<0.01) at each time intervals compared with the group treated with IND-CD. Furthermore, it is noteworthy that in the group treated with IND-HPMC the retinal distribution of indomethacin was sustained (Fig. 2C). Representative chromatograms of indomethacin in each sample tissue are shown in Fig. 3.
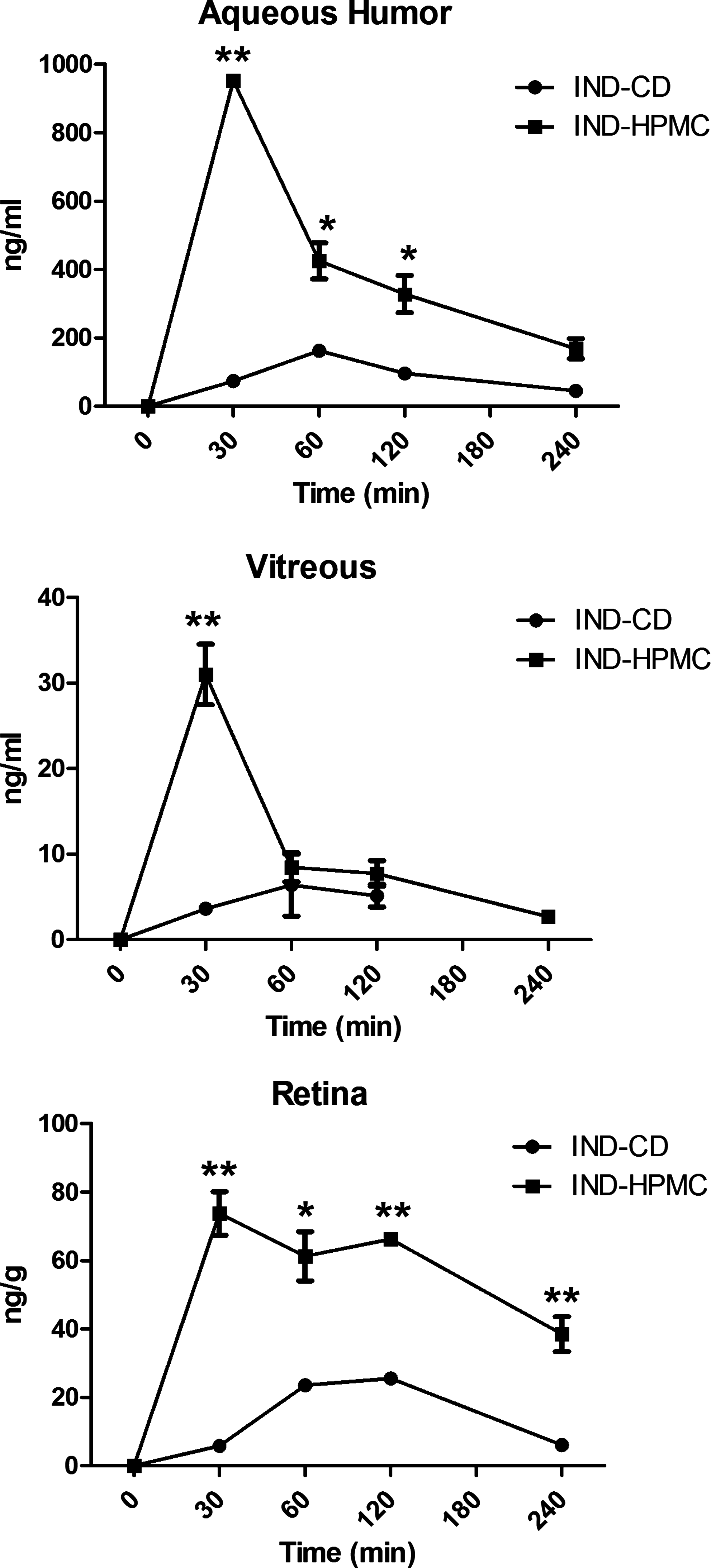
Ocular distribution of indomethacin in rabbit eye after multiple treatment with indomethacin+hydroxypropylmethylcellulose (IND-HPMC) or indomethacin+hydroxypropyl-β-cyclodextrin (IND-CD). Each point represents the mean±standard deviation (SD) of four to six samples. (*) P<0.05; (**) P<0.01 vs. IND-CD.
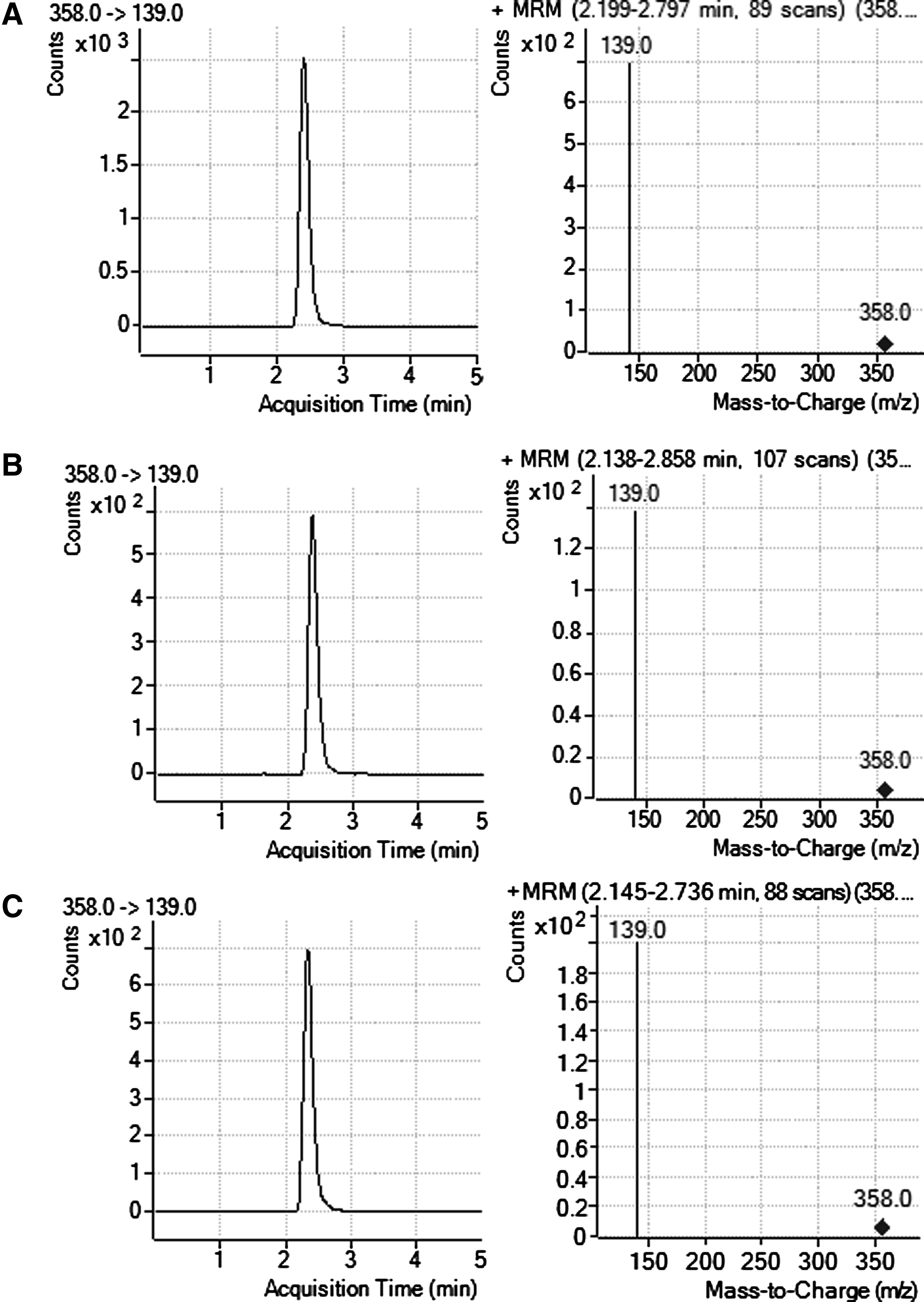
Representative chromatograms in aqueous humor (
P<0.05.
P<0.01 vs. IND-CD.
Tmax, time to peak value; Cmax, peak drug concentration; AUC0–240, area under the concentration–time curve between 0 and 240 min; IND-HPMC, indomethacin ophthalmic suspension containing hydroxypropylmethylcellulose; IND-CD, indomethacin ophthalmic solution with hydroxypropyl-β-cyclodextrin.
Discussion
Topical NSAIDs have proven effective in treating many inflammatory ocular disorders, and newer topical formulations available, some of which are already in the market, with different pharmacokinetics may allow important therapeutic advances for the back of the eye. NSAIDs are one of the most commonly prescribed classes of medications worldwide, and they have used to maintain mydriasis during eye surgery, reduce postoperative inflammation, and treat ocular inflammatory conditions. With our growing understanding of pathogenesis, the clinical indications for topical NSAIDs may continue to expand. For instance, scientists and ophthalmologists have long agreed that inflammation appears to be at least part of the pathogenesis of cystoid macular edema (CME) after cataract surgery; therefore, it was reasonable to attempt to prevent and minimize the inflammatory response with NSAIDs, particularly with indomethacin.
Another good example of inflammation involvement is represented by diabetic macular edema (DME). The pathogenesis of DME is complex and multifactorial, but ultimately is the result of disruption of the blood–retinal barrier due to a variety of inflammatory mediators such as, among of others, cytokines, adhesion molecules, integrins, growth factors, lipid-derived mediators, and enzymes. It is noteworthy that much evidence indicates a key role of COX-2 in the pathogenesis of DME; in fact, this enzyme is a promoter of angiogenesis and can be detected in human choroidal neovascular membranes.2,9,12–14 Furthermore, inhibition of COX-2 by NSAIDs reduces VEGF production and neovascularization in trauma-, ischemic-, and diabetic-induced animal models.2,8,9,15,16 Another potential use of NSAIDs has been suggested in AMD. AMD is a leading cause of blindness for individuals aged 55 and over. 17 The pathogenesis of AMD is complex and poorly understood; however, there is considerable evidence from human and animal studies that inflammation plays a central role.
New topical formulations of indomethacin with potentially greater retinal penetration, some of which are already available in the market, stimulated us to investigate the pharmacokinetic profile of this drug after topical administration of eye drops. The present study demonstrated that, among the formulations available in the European market, IND-HPMC has better ocular distribution compared with IND-CD, and this is likely due to the major reason of different concentrations and diverse vehicles. Cyclodextrins are a family of cyclic oligosaccharides with a hydrophilic outer surface and a lipophilic central cavity (Fig. 1B, D), and they have mainly been used as complexing agents to increase the aqueous solubility of poorly soluble drugs and to increase their stability. In addition, their effects on ocular bioavailability are quite controversial. Studies have reported both a decrease18,19 and an increase20,21 in ocular bioavailability when compared to suspension having the same drug concentration. The reasons for these conflicting findings are not completely clear; however, a clue could come from the differences in terms of physicochemical characteristics of the molecules, the different concentrations of cyclodextrins, and the presence of other vehicles.
It is noteworthy that when using cyclodextrins in the reformulation of ophthalmic suspensions as solutions, attention must be paid to the concentration of cyclodextrin used; in fact, very often the final result is a decrease in ocular bioavailability because whole molecules of the active ingredient are tightly complexed and hardly available (Fig. 1D). Besides that, it is well known that cyclodextrins do not have mucoadhesive properties; on the contrary, polymers such as sodium hyaluronate, carbopol, and hydroxypropylmethylcellulose are bioadhesive to the ocular surface and they are able to improve the ocular bioavailability of drugs. This latter fact has been well demonstrated in numerous studies22,23 where ocular formulations with cyclodextrins were compared with or without the presence of bioadhesive polymers. These considerations fit with the data of the present study, where IND-HPMC and IND-CD formulations contain hydroxypropylmethylcellulose and hydroxypropyl-β-cyclodextrin, respectively. Taken together, these findings seem to indicate that the IND-HPMC formulation has good ocular distribution, reaching relevant retinal indomethacin levels, and suggest that this formulation may be very useful for clinicians to treat various disorders in the back of the eye.
Footnotes
Disclosure Statement
Claudio Bucolo, Filippo Drago, Barbara Melilli, and Cateno Piazza have no proprietary interest in the products and no competing financial interests. Monia Zurria is employee of Alfa-Intes.