
Abstract
Abstract
Purpose:
To evaluate the retinal and optic nerve functions of bevacizumab when injected intravitreal in human eyes using electrophysiological tests; electroretinogram (ERG) and visual evoked potentials (VEP).
Methods:
Fifty-five eyes of 55 patients with choroidal neovascular membrane (CNV) who were prepared for intravitreal injections of 1.25 mg bevacizumab underwent baseline ERG and VEP in both eyes before, and at 1 and 6 weeks after the intravitreal injections.
Results:
Mean age was 50 years ranging from 24 to 62 years, with 32 age-related macular degenerations and 23 myopic patients. Mean baseline best corrected visual acuity (BCVA) was 4/60, and mean final BCVA at 6 weeks was 6/60. There was no statistically significant reduction of the postinjection (1 and 6 weeks) ERG A and B-waves or the VEP waves' amplitudes and latency, or in the contralateral noninjected eyes. On the contrary, there were statistically significant improvement at 1 and 6 weeks in the photopic B-wave of the injected and fellow eyes (P values=0.046, and <0.001).
Conclusions:
Intravitreal bevacizumab did not appear to be toxic to the retina or the optic nerve at a concentration of 1.25 mg.
Introduction
Philip Rosenfeld and colleagues publications for the efficacy of systemic 7 then intravitreal injections 8 of bevacizumab for patients with choroidal neovascular membranes (CNV) secondary to age-related macular degenerations (AMD), have initiated a worldwide interest in the use of this drug for many ocular pathologies.9–13 During the past 5 years, many researchers have assessed the safety of intravitreal bevacizumab on retinal functions by histopathology and electrophysiology mainly electroretinograms (ERG).14–18 However, only few studies have investigated the effect of bevacizumab on optic nerve functions in human eyes, 18 which could be affected either by direct toxicity or indirectly by reducing blood circulation in the optic nerve head. In this study we investigated the effect of intravitreal bevacizumab on optic nerve and retinal functions by electrophysiological test; visual evoked potentials (VEP) and ERG.
Methods
Approval for the study was obtained from the hospital's ethical committee, and the tenets of the Declaration of Helsinki were followed. All patients received a thorough explanation of the study design and aims, and were provided with written informed consent.
This is a prospective nonrandomized uncontrolled interventional study, where patients who were scheduled for intravitreal injections of bevacizumab were included. Inclusion criteria: patients with CNV secondary to AMD or myopia. Exclusion criteria were eyes with (1) previous vitrectomy and/or intraocular surgeries, (2) recent intravitreal injections with anti-VEGFs and/or triamcinolone, (3) previous trauma, and (4) no other ocular pathologies.
Preoperatively all patients were evaluated before injection for best corrected visual acuity (BCVA), slit-lamp examination, intraocular pressure (IOP), dilated fundus examination, fundus fluorescein angiography, and optical coherence topography when necessary for the diagnosis and follow-ups after injections. Baseline ERG and VEP in both eyes were done before injections. Intravitreal injections of bevacizumab (1.25 mg/0.05 mL) were received. All patients were examined on the first day after injections to check for complications resulting from the intravitreal procedure. All patients were then re-examined 1 week after the injection for BCVA, slit lamp, and IOP. ERG and VEP were repeated 1 and 6 weeks after the intravitreal injections. Each of the ERG and VEP recordings done at baseline, 1 and 6 weeks following bevacizumab injections were done twice, 24 h apart, and the average of both recordings was taken.
Flash ERG recordings
The pupils were maximally dilated to ∼8 mm in diameter following topical application of a mixture of 0.5% tropicamide and 0.5% phenylephrine HCL. Ganzfield full- field electroretinogram (ffERGs) were recorded from both eyes on the Espion E 2 ERG instrument using Dawson-Trick-Litzkow–Plus electrodes (both by Diagnosys LLC). ERGs were done according to the International Society for Clinical Electrophysiology of Vision (ISCEV) standards in both scotopic and photopic states to assess retinal function. 19 The minimum protocol incorporates the rod-specific and standard bright flash ERGs, both recorded after a minimum of 20 min dark adaptation. After 10 min of light adaptation, the photopic 30 Hz flicker cone and transient photopic cone ERGs were recorded. In brief, the parameters measured were: a 30 Hz flicker (in a light-adapted patient, cone responses are evoked by a stimulus flickering at 30 Hz); a photopic single flash; scotopic oscillatory potentials; and scotopic single flash (in the dark-adapted eye is maximal response, a bright single white flash stimulus and in a dark-adapted eye, a rod-isolated response is obtained that occurs after a dark-adapted patient receives dim white and/or a blue flash that is below the cone threshold, and doing so, the resulting waveform is almost exclusively a B-wave).
Flash VEP recordings
VEPs were done according to the ISCEV standards. 19 Flash VEPs were recorded using 5 electrodes positioned 3–5 cm apart (depending on the subject's head size) across the occiput in a row 2 cm above the inion. These were referred to a mid-frontal reference electrode at Fz. Their positions were aligned according to the international 10–20 system. 20 Electrode impedance was <5 kohms. Low and high bandpass filter settings were 1 and 100 Hz with an analysis time of 250 ms. Patients wore their full spectacle correction throughout. Flash VEPs were recorded to a 2 Hz stimulus of intensity 17 cd/s/m2 using a Grass photic stimulator positioned ∼25 cm from the subject's eyes (<25 cm if younger subjects showed limited compliance).
Data were statistically described in terms of range, mean±standard deviation (±SD), frequencies (number of cases), and percentages when appropriate. Comparison of numerical variables between the study groups was done using 1-way analysis of variance (ANOVA) test with post hoc multiple 2-group comparisons. P values less than 0.05 was considered statistically significant. All statistical calculations were done using computer programs Microsoft Excel 2007 (Microsoft Corporation) and SPSS (Statistical Package for the Social Science; SPSS, Inc.) version 19 for Microsoft Windows.
Results
Fifty-five eyes of 55 patients were included in our study with a mean age of 50 years (ranging from 24 to 62 years). Male to female ratio was 4:5. Patients' diagnoses were as follows: 33 patients with CNV due to AMD and 22 patients with myopic CNV. IOPs did not change in any of our patients during the study period. Mean baseline BCVA was 4/60, and mean final BCVA at 6 weeks was 6/60. All our patients had a relatively small to moderate size CNV (1–2 Disc Area) with no exudation.
Tables 1–3 shows the mean with the SDs of the photopic and scotopic ERG A and B-waves (Tables 1 and 2); and VEP P100 amplitude and latency (Table 3) for the injected eyes and fellow eyes; before, 1 week, and 6 weeks after injections. There were no statistically significant reduction of the ERG A and B-waves amplitudes in the injected and fellow eyes under scotopic and photopic conditions at 1 and 6 weeks postinjection (P values >0.05). Also there were no statistically significant reduction of the VEP P100 amplitude and latency at 1 and 6 weeks when compared with baseline records (P values >0.05).
Included are the P values for the statistical analysis between different study points.
ERG, electroretinogram; μv, microvolt; msec, millisecond; SD, standard deviation.
Significant.
Included are the P values for the statistical analysis between different study points.
Significant.
Included are the P values for the statistical analysis between different study points.
VEP, visual evoked potential.
On the contrary, there was improvement in the following: (1) Photopic B-wave in the injected eyes showed significant improvement after the injections at 1 and 6 weeks (P value=0.046). (2) Photopic B-wave in the fellow eyes showed a highly significant improvement after the injections at 1 and 6 weeks (P value <0.001). (3) Nonsignificant improvement was also noted in the photopic A-wave amplitudes of the injected eyes at 1 and 6 weeks postinjections. (4) Although the VEP data analysis showed no significant difference between the baseline amplitude and latency, yet there were a notable improvement of all parameters in the injected eyes at 1 and 6 weeks (Table 3). Multiple group analysis was done to confirm the above result (Table 4).
Multiple group analysis at the different study points; baseline, 1 and 6 weeks.
Significant.
Electroretinograms
Figures 1 and 2 show the mean of the photopic and scotopic A and B-wave amplitudes at baseline, 1 and 6 weeks after injections in the injected and fellow eyes, respectively.
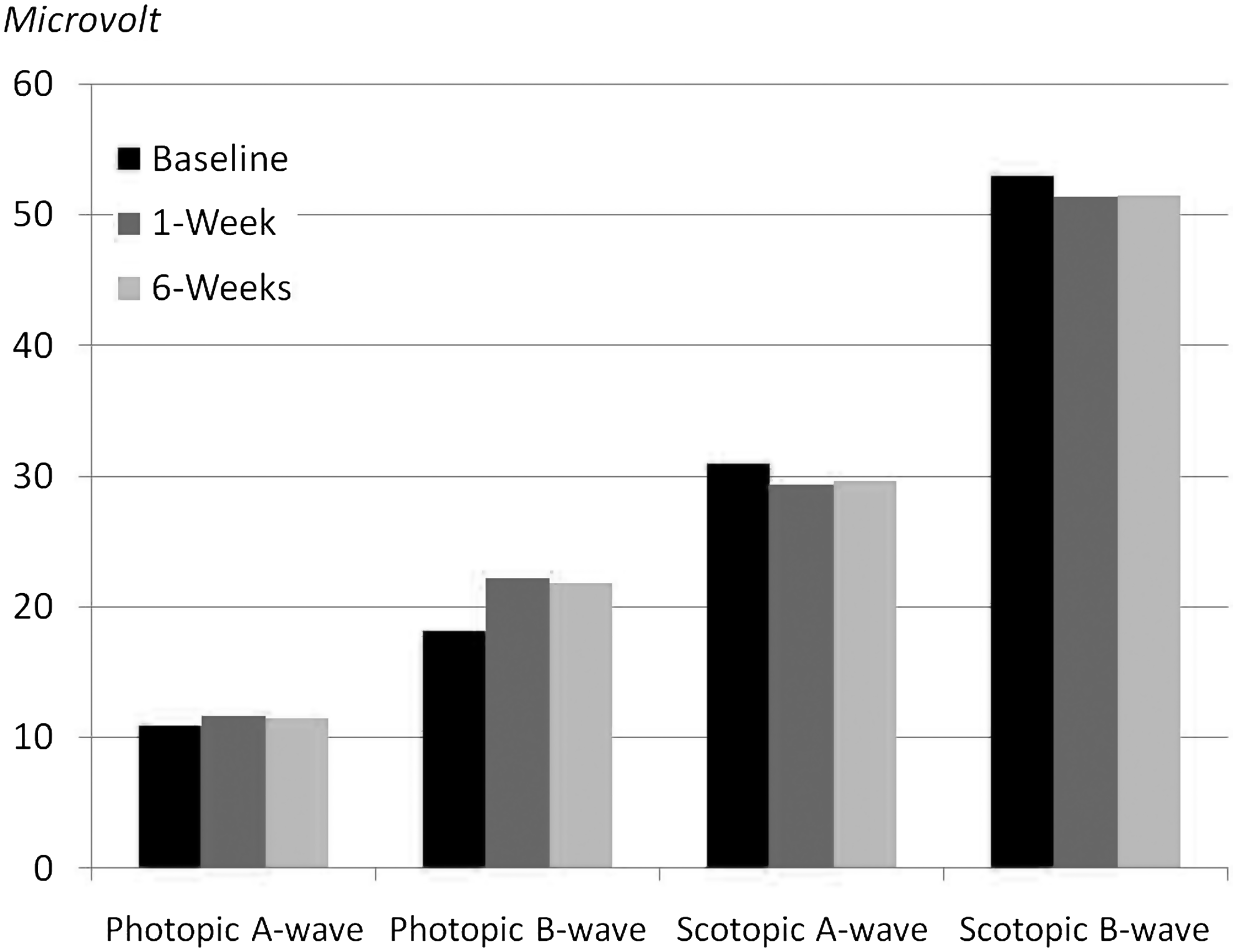
The injected eyes' mean±standard deviation (SD) electroretinogram (ERG) waves' amplitudes: Photopic: A-wave: 10.85±10.1, 11.62±1.69, 11.5±1.78, B-wave: 18.1±5.46, 22.21±5.15, 21.82±5.37; Scotopic: A-wave: 30.93±4.29, 29.37±4.76, 29.6±4.82, B-wave: 52.96±12.27, 51.33±7.05, 51.44±7.07, at baseline, 1 and 6 weeks postinjections, respectively.
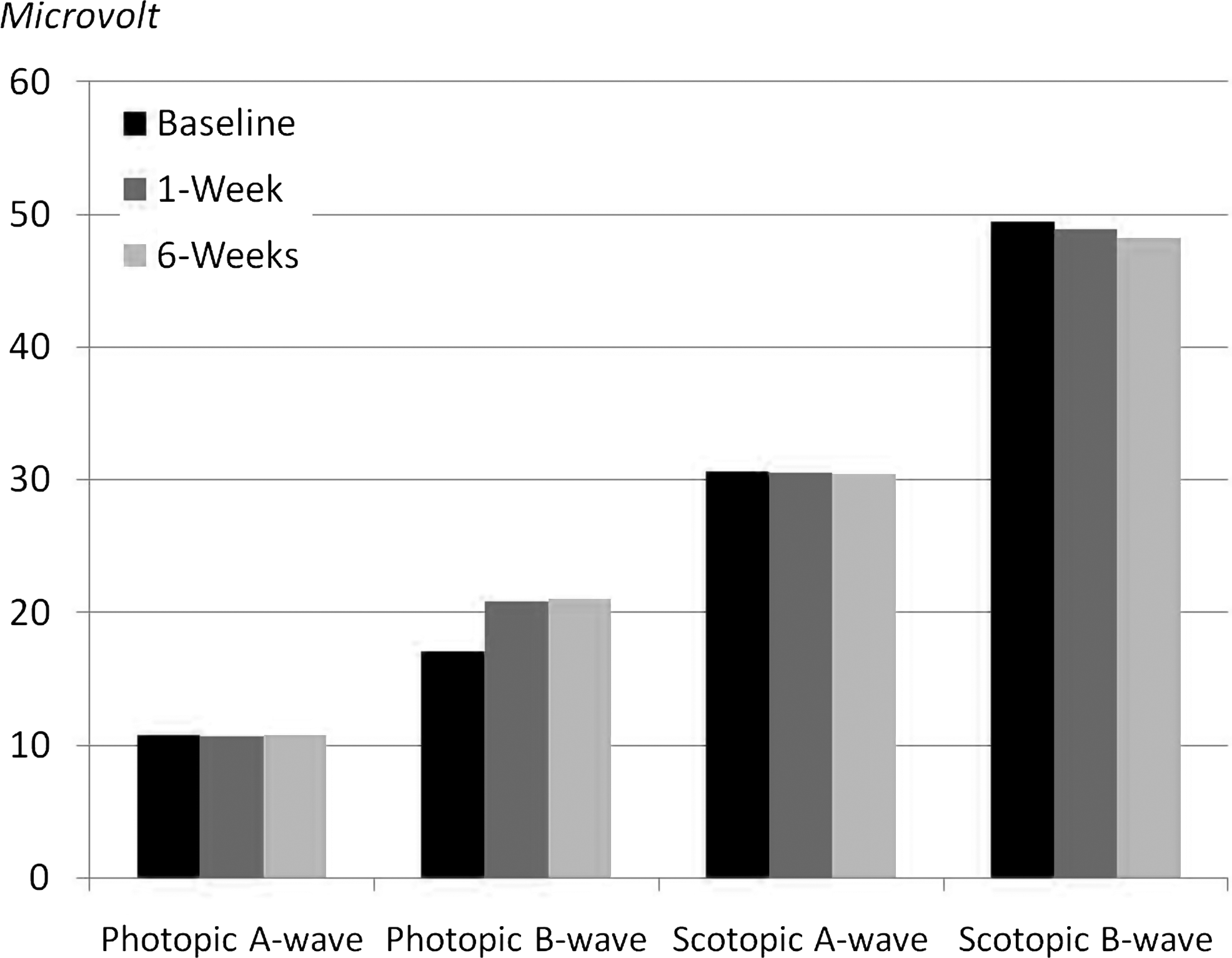
The fellow eyes' mean±SD ERG waves' amplitudes: Photopic: A-wave: 10.79±2.36, 10.66±1.05, 10.76±1.39, B-wave: 17.01±2.97, 20.83±3.65, 20.97±3.53; Scotopic: A-wave: 30.63±7.06, 30.49±4.1, 30.41±4.05, B-wave: 49.42±6.57, 48.87±9.25, 48.23±9.21, at baseline, 1 and 6 weeks postinjections, respectively.
Photopic conditions
The injected and fellow eyes showed slight improved amplitudes which were significant for the B-wave at 1 and 6 weeks postinjection in both eyes.
Scotopic conditions
No significant changes were observed in both eyes at 1 and 6 weeks after the injections, but there was a slight nonsignificant depression of A and B-waves.
Visual evoked potentials
There were no observed deterioration in the P100 amplitudes and latency in the injected and fellow eyes at 1 and 6 weeks after injections as seen in Figs. 3 and 4. However, improved P100 amplitudes (Fig. 3) and latency (Fig. 4) in the injected eyes is noted at 1 and 6 weeks after injections.

The mean±SD of the visual evoked potential (VEP) P100 amplitudes (N75-P100) for the injected (6.53±2.35, 7.23±4.49, 7.32±4.48) and fellow eyes (8.83±2.38, 7.68±4.06, 7.66±4.07), at baseline, 1 and 6 weeks postinjections, respectively.
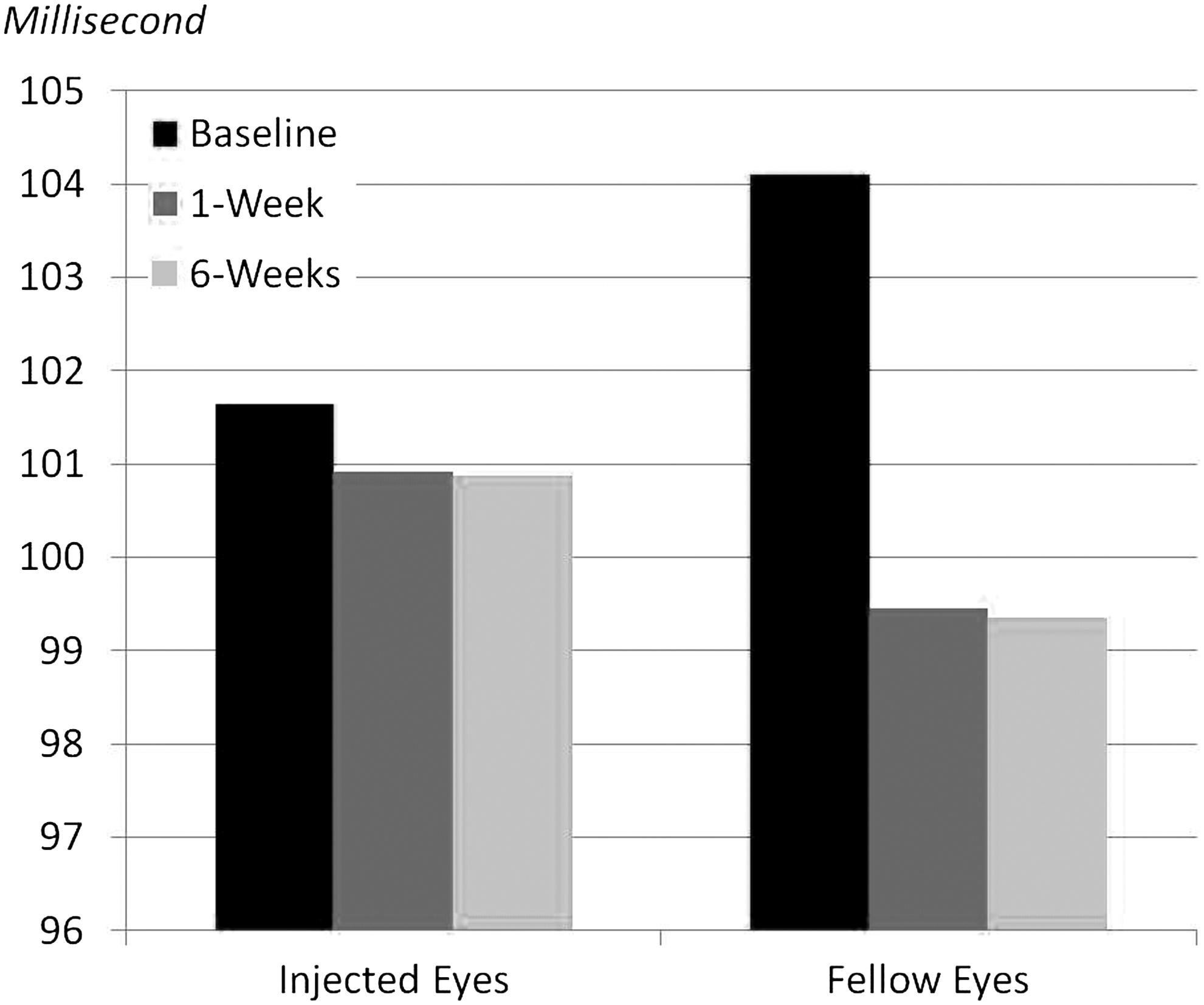
The mean±SD of the VEP P100 latency for the injected (101.64±17.05, 100.91±13.78, 100.86±13.64) and fellow eyes (104.103±18.05, 99.45±13.14, 99.35±13.2) at baseline, 1 and 6 weeks postinjections, respectively.
Discussion
Although the retinal toxicity of intravitreal bevacizumab has been tested in numerous humans and animals study and appeared to be safe,14–18 its effect on optic nerve head functions was not properly investigated. Bevacizumab has been found to occasionally produce retinal ischemia due to the reduction of VEGFs which appeared to play an important role in normal retinal vascularity and circulation.
To provide additional insight into the safety of intravitreal bevacizumab, we performed electrophysiological tests to study optic nerve and retinal toxicity. We report a series of patients who received a single intravitreal injection of bevacizumab 1.25 mg in 0.05 mL for CNV (AMD and myopia) that had a baseline VEP and ERG (photopic and scotopic), at 1 and 6 weeks postinjections.
Previous animal studies using flash VEP 16 showed that responses of the experimental eyes were of normal pattern and amplitude and did not differ from those recorded by stimulation of the control eye alone. In human eyes, Pai et al. 18 used pattern VEP in addition to multifocal electroretinogram (mfERG) and ffERG. Testing for retinal and optic nerve functions by ffERG, mfERG, and pattern VEP studies showed no short-term safety concerns of intravitreal bevacizumab.
Our present study confirms the previous reports on the safety of intravitreal injection of bevacizumab. Our nonrandomized, uncontrolled, prospective, interventional study did not find any statistically significant reduction of ERG waves' amplitudes and implicit times or in VEP P100 amplitudes or latency times at 1 and 6 weeks after intravitreal injections of bevacizumab; compared to baseline in both eyes. On the contrary, we found significant improvements in some ERG in both the injected and the fellow eyes and non significant VEP waves improvements in the injected eyes as mentioned earlier. However, we do not have any scientific explanation for these changes at the moment.
In conclusion, intravitreal bevacizumab appeared to be safe and tolerable with no detectable significant reduction in optic nerve or retinal functions in the injected or the fellow eyes. However, this study is limited by its short duration; a study with a longer follow-up duration, perhaps 6 months, is needed. In addition, further research with a larger sample size for each disease entity is warranted to confirm the results in this study.
Footnotes
Author Disclosure Statement
The authors report no declarations of interest. The authors have no disclosure(s) to declare. The authors have no financial or proprietary interest in any product mentioned in this article. There is no funding/support for this study.