
Abstract
Abstract
Purpose:
After keratoplasty, antibiotic eye drops are used to prevent ocular infection until the recipient corneal epithelium has healed. We compared the effects of azithromycin, a new macrolide, with the effect of the standard antibiotics, tobramycin, on the (i) prevention of infection, (ii) epithelial healing, and (iii) ocular tolerance after penetrating keratoplasty.
Methods:
In this prospective, single-center, randomized study, patients undergoing penetrating keratoplasty received postoperative topical dexamethasone and either azithromycin (n=23; Azyter®; one drop twice daily for 3 days) or tobramycin (n=23; Tobrex®; 1 drop 4 times daily until complete re-epithelialization). Daily slit-lamp examination with fluorescein was performed, and photographs were taken to digitally assess the re-epithelialized surface area. Daily questionnaires assessed ocular comfort and pain.
Results:
There were no cases of infection in either group. The re-epithelialized area of the corneal graft increased at a similar rate in each group, with no difference between the groups on any day. The mean±SD days until complete re-epithelialization did not differ between tobramycin (4.14±1.17) and azithromycin (4.13±1.82) (P=0.89). Superficial punctate keratitis scores were similar for tobramycin (1.39) and azithromycin (1.34). Pain and discomfort scores improved each day after surgery with no differences between the groups on any day.
Conclusion:
Postkeratoplasty epithelial healing and ocular tolerance were not significantly different between the azithromycin- and tobramycin-treatment groups. Our results support the use of azithromycin as an alternative to tobramycin after corneal surgery such as keratoplasty.
Introduction
Tobramycin (Tobrex® 0.3%; Alcon Laboratories), one of the standard postkeratoplasty antibiotics, is effective but requires an intensive dosage regimen of 4 drops per day until the cornea has re-epithelialized. Another disadvantage of tobramycin is the inclusion of the preservative benzalkonium chloride 0.01% (BAK), which is thought to cause eye irritation, to impair the stability of the corneal epithelium, 7 and to delay epithelial healing.8,9
Azithromycin (Azyter® 1.5%; Théa Laboratories), a second-generation macrolide, has a broad spectrum activity against gram-positive and gram-negative bacteria, is relevant for keratitis, and has been shown to be safe and effective in the treatment of purulent bacterial conjunctivitis.10–14 Azithromycin 1.5% eye drops undergo rapid tissue distribution with constantly raised concentrations in corneal and conjunctival tissues; therefore, efficacy can be maintained at a lower dose. 15 An added advantage of the Azyter formulation of azithromycin is the preservative-free single dose unit (SDU) packaging.
The aim of this study was to compare postkeratoplasty prevention of infection, corneal epithelial healing, and ocular comfort in patients treated with either azithromycin (Azyter 1.5%) or tobramycin (Tobrex 0.3%).
Methods
Study design and patients
A prospective, single-center, randomized study was performed in 46 patients who underwent penetrating keratoplasty in one eye between June 2009 and May 2010 at the Strasbourg University Hospital. The study was performed in accordance with Good Clinical Practice guidelines. Independent ethics approval was obtained, and each patient gave informed written consent. Keratoplasties arising from the following conditions were included: bullous keratopathies (pseudophakic bullous dystrophy, Fuchs dystrophy), keratoconus, transplant changes (chronic rejection or endothelial decompensation), and postinfectious corneal scars (including those of herpetic origin). Patients were not included in the study if they (i) had emergency keratoplasty for active corneal infection, (ii) were prescribed cyclosporin eye drops to prevent the rejection of transplant tissue, (iii) had a significant deficit in limbal stem cells, (iv) had severe dry eye syndrome, (v) had eyelid abnormalities such as palpebral trauma or malposition with corneal involvement, or (vi) had complete corneal anesthesia.
Transplant tissue
Corneal transplant tissue was obtained from the Franche Comté cornea bank. After postmortem harvest from the donor, the tissue was stored in culture for 14 to 24 days. The corneal storage media contain 2 antibiotics (penicilline G 100 U/mL, Streptomycine 100 μg/mL) and amphotericine B (0.25 μg/mL). On day 13 of storage, an endothelial count, morphological evaluation of the transplant, and serological and microbiological safety checks were performed on the transplant tissue.
Surgical technique
All surgeries were performed under general anesthesia by the same surgeon. A Hanna trephine was used to trephine the recipient cornea at 100% depth. The trephine diameter was 8.25, 8, or 7.75 mm depending on the size of the recipient cornea. The corneal transplant was trephined and over-sized by 0.25 mm compared with the recipient. It was then sutured to the recipient cornea by 16 separate stitches or 4 separate stitches combined to a radial circumferential continuous stitch of 10/0 nylon monofilament, depending on the age and initial pathology of the patient. The epithelium of the transplanted cornea was then removed using a sterile triangular eye sponge. A subconjunctival injection of dexamethasone (Célestène®; Schering-Plough Laboratories) was administered, followed by instillation of a drop of Tobradex® (tobramycin combined with dexamethasone; Alcon Laboratories) and application of one drop of a viscoelastic product (Viscoat®; Alcon Laboratories). After the surgery, the eye was covered with an occlusive pad-type bandage with a protective shell. The day of surgery was designated day 0 of the study.
Antibiotic treatment
Patients were randomized before surgery in a 1:1 fashion to receive either tobramycin or azithromycin. Four hours after the surgery, the bandage was removed, and the transplanted eye was treated with one drop of either tobramycin or azithromycin. Patients in the tobramycin 0.3% group then received one drop of tobramycin 4 times daily until the cornea had completely re-epithelialized. Patients in the azithromycin 1.5% group received one drop of azithromycin twice daily for a fixed period of 3 further days. In addition, each patient was treated with dexamethasone (Dexafree®; Théa laboratories) and carmellose sodium (Celluvisc®; Allergan laboratories), both at a dose of 1 drop 4 times per day until the cornea had completely re-epithelialized.
Postoperative examinations
Re-epithelialization of the transplant was assessed daily by slit-lamp examination after instillation of fluorescein. A blue-light digitized 10× photograph was taken, and the re-epithelialized surface area (ratio of 2 areas) was calculated using Mesurim Pro software® (Académie Amiens). The occurrence of infection was also recorded. At the day 10 postoperative examination, fluorescein and slit-lamp examination were used to quantify superficial punctate keratitis (SPK) on the Oxford score. Patients filled in 2 questionnaires daily: the visual analog scale (VAS) was used to quantify pain, and the ocular surface disease index (OSDI) was used to quantify ocular discomfort. 16
Statistical analysis
For each patient, the following quantitative variables were measured: the age of the patient, the age of the donor, the delay from donor death to tissue harvest, the duration of tissue conservation, the density of the tissue on day 13 of storage, the delay to complete re-epithelialization, the SPK score, and the comfort score. The following qualitative variables were also measured: indication for transplant and postoperative treatment (azithromycin or tobramycin). The threshold of 0.05 was chosen as the limit of significance. Treatment groups were compared using the Mann–Whitney test for quantitative variables or the Fischer exact test for qualitative variables. The regression analysis was carried out. Statistical tests were performed using GraphPad Prism 5 (GraphPad, Inc.).
Results
Patient demographics
This study included 46 patients (19 men and 27 women), with a mean±SD age of 67±15 years (range 16 to 89), each of whom underwent corneal transplant in one eye (Table 1). There was no statistically significant difference in donor age, time to tissue harvest postmortem, endothelial cell density, or mean storage density between the 2 groups (Table 2). The size of the transplant was similar between the groups (Table 3).
NA, not applicable.
Corneal healing
The re-epithelialized surface area increased rapidly between days 1 and 3 and then increased at a slower rate until complete re-epithelialization had occurred by day 9 (Fig. 1). The area of the re-epithelialized cornea did not significantly differ between the groups on any day. All patients in the tobramycin group had been fully healed by day 7 postsurgery. In the azithromycin group, 1 patient had not been fully healed by day 7 (61% re-epithelialization), but all the transplants in each group had re-epithelialized by day 9. The mean±SD number of days taken for complete re-epithelialization of the cornea was similar between the tobramycin group (4.14±1.17 days) and the azithromycin group (4.13±1.82 days) (P=0.89). The time for re-epithelialization varied depending on the initial reason for transplant, but there were no significant differences between the treatment groups (Table 4).
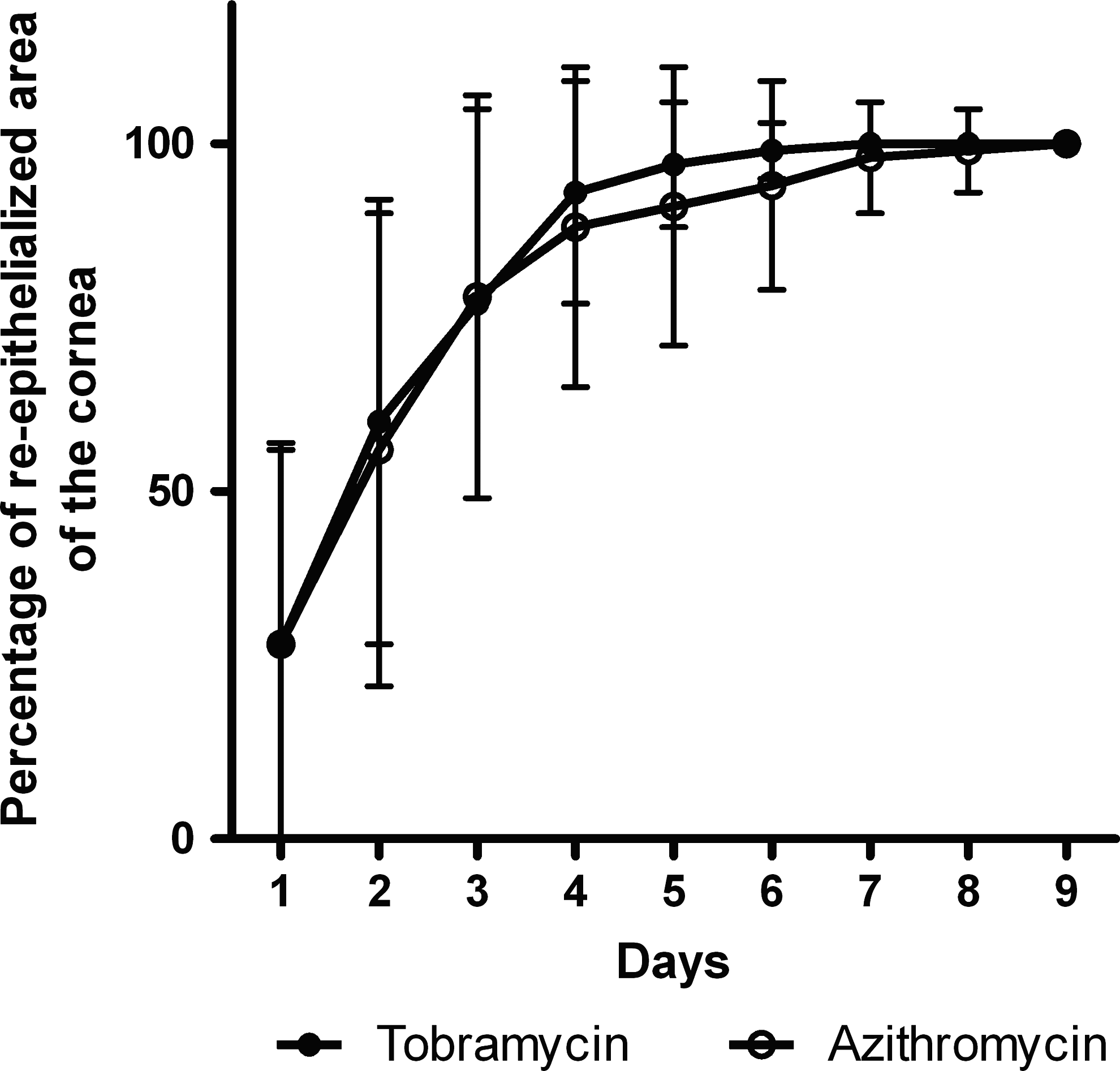
Re-epithelialized area of the cornea in patients undergoing penetrating keratoplasty. Mann–Whitney test P>0.05.
Oxford, VAS, and OSDI scores
The SPK scores on day 10 were similar between the tobramycin group (1.39) and the azithromycin group (1.34) (Mann–Whitney test; P=0.80). The VAS and OSDI scores in both groups improved steadily each day after the surgery. There were no significant differences in either the VAS score (Fig. 2) or OSDI score (Fig. 3) between the 2 groups on any day after the transplant.

Visual analog scale that quantifies pain in patients undergoing penetrating keratoplasty. Mann–Whitney test P>0.05.
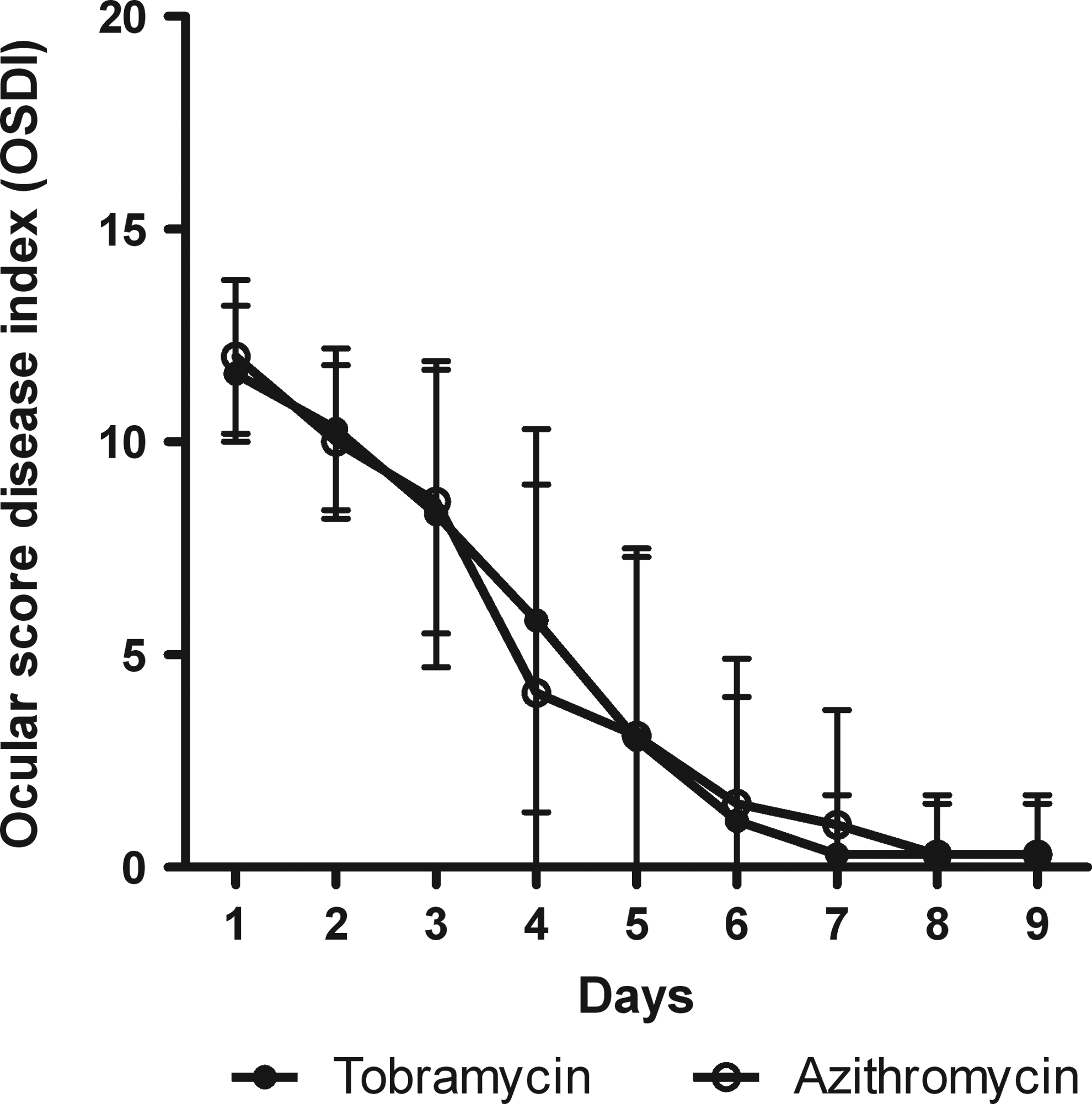
Ocular surface disease Index in patients undergoing penetrating keratoplasty. Mann–Whitney test P>0.05.
Infection
No cases of infection were reported in either group over the course of the study.
Discussion
After penetrating keratoplasty, antibiotic eye drops are administered as routine prophylactic treatment to prevent bacterial infection, which is one of the many reasons for the failure of corneal transplant. We compared one of the standard treatments, tobramycin (Tobrex), with azithromycin (Azyter), which has the advantage of a shorter, less intensive dosage schedule and a nonpreserved SDU formulation.
Treatment groups were comparable with regard to surgical technique, recipient ocular health, and nonantibiotic pharmacological interventions. The ocular health of the recipient eye before the transplant is thought to be more important than the ocular health of the donor eye;1,4 therefore, patients were excluded if they presented severe limbal deficiency or abnormalities of the eyelid and lacrymal film. After surgery, transplanted eyes in each treatment group were treated with sodium hyaluronate, which accelerates corneal transplant healing1,7 and dexamethasone to reduce inflammation and the risk of rejection. Dexamethasone, however, reduces the proliferation of corneal epithelial cells and extends healing time.1,3,17 Both azithromycin and tobramycin prevented microbial contamination, with no infections reported in either group. This supports previous reports that azithromycin is as effective as tobramycin in the treatment of eye infections.10–14
The mean time taken for complete re-epithelialization of the cornea after transplant was similar in the tobramycin (4.14 days) and azithromycin groups (4.13 days), which is in line with previously published data reporting a healing time of 2.5 to 4.6 days. 1 BAK, the preservative used in the tobramycin formulation, has been reported as either prolonging8,9 or having no effect 18 on epithelial healing. Our data suggest that BAK had no effect, but further investigation with appropriate controls is required to further elucidate the effect of BAK on epithelial healing. In our study, all patients in both groups had complete re-epithelialization by day 9. Other studies have found that complete re-epithelialization varies from 28.5% to 64.5% on day 11,2 and from 89% to 93.5% on day 71,19 The absence of re-epithelialization on day 1 in our study can be explained by the total ablation of the transplant epithelium at the end of the surgery to reduce the risk of transplant rejection. Previous studies reported that tobramycin had no effect on,20,21 or prolonged,22,19 epithelial healing time. To our knowledge, this is the first study in humans that investigates the effect of azithromycin on corneal epithelial healing. In an animal model of corneal refractive surgery, azithromycin was well tolerated and effectively prevented bacterial infection. 23
We found that the ocular tolerance of azithromycin was similar to that of tobramycin, in accordance with several previous reports comparing the 2 antibiotics in the treatment of bacterial conjunctivitis.10–14 The VAS score for pain was similar in each treatment group, as was the OSDI score for ocular comfort. It should be remembered that changes in corneal innervation will have occurred during the transplantation, which may influence or overshadow the effects due to antibiotic use. In addition, postoperative swelling could impair the clarity of vision, which could impact the ODSI score.
Azithromycin, a second-generation macrolide, differs from erythromycin by the addition of one nitrogen atom, which confers improved tissue penetration and digestive tolerance. 24 An important advantage of azithromycin eye drops is the persistence of the antibiotic effect for up to 1 week in the cornea after treatment has been stopped 25 ; therefore, it can be administered for fewer days without compromising efficacy. The twice daily regimen for 3 days for azithromycin is more convenient for the patient than the longer, more intensive treatment schedule for tobramycin. This may improve patient compliance and completion of antibiotic courses, which will, in turn, reduce the emergence of antibiotic-resistant strains. The preservative-free SDU formulation of azithromycin also avoids the potential deleterious effects of the preservative BAK such as eye irritation and prolongation of epithelial healing time.
In conclusion, we found that postkeratoplasty epithelial healing and ocular tolerance were not significantly different between the azithromycin and tobramycin treatment groups. The advantages of azithromycin just mentioned may also be applied to other surgical procedures involving re-epithelialization such as refractive surgery and, more specifically, refractive photokeratectomy. Our results add to the growing body of evidence supporting the use of azithromycin as a first-line antibiotic in an ocular context.
Footnotes
Author Disclosure Statement
No competing financial interests exist.