
Abstract
Abstract
Purpose:
To study the microbial spectrum and antibacterial susceptibility of vitreous cultures in a tertiary referral center in Northeast United States.
Methods:
All vitreous samples sent to the microbiology laboratory at a tertiary referral center from January 1988 to December 2008 were included in the study. The distribution and antibiotic susceptibility of all isolates from culture-positive samples were compared across 3 equal time periods 1988–1994, 1995–2001, and 2002–2008.
Results:
One hundred forty-three positive cultures, where 11.9% (n=17) were polymicrobial, yielded a total of 160 isolates that consisted of 80.6% (n=129) gram-positive isolates, 12.5% (n=20) gram-negative isolates, and 6.9% (n=11) fungal isolates. The most prevalent organisms were coagulase-negative Staphylococcus (CoNS) (37.5%, n=60), Viridans Streptococcus (11.3%, n=18), and Streptococcus pneumoniae (6.9%, n=11). Other common gram-positive isolates include Propionibacterium acnes (5.6%, n=9), other Streptococcus species (4.4%, n=7), Staphylococcus aureus (4.4%, n=7), and Enterococcus faecalis (3.8%, n=6). The most common gram-negative isolates were Klebsiella species (3.1%, n=5), Moraxella species (3.1%, n=5), and Haemophilus species (2.5%, n=4). Vancomycin was effective against all CoNS, Sta. aureus, Viridans Streptococcus, and E. faecalis tested, and all Sta. aureus isolates were oxacillin sensitive. Of all CoNS isolates, 83.3% during 1988–1994, 73.1% during 1995–2001, and 100% during 2002–2008 were resistant to at least 1 of the antibiotics tested in the study with the last time period showing an increase in resistance (P=0.021, adjusted standard residual=2.0). CoNS showed a decreasing resistance over time to chloramphenicol and gentamicin (P=0.010, P=0.007, respectively) and an increase in resistance to penicillin and tetracycline during 2002–2008 (P=0.003, P=0.040, respectively). Susceptibility to other antibiotics did not show significant dependence on time.
Conclusion:
Bacteria causing endophthalmitis showed variable resistance to antibiotics over time. The importance of adequately treating endophthalmitis in the setting of these resistance pattern changes stresses the importance of periodic evaluation of causative organisms to ensure appropriate empiric treatment.
Introduction
Suspected endophthalmitis is an ocular emergency that can lead to blindness, and empirical antimicrobials are frequently used before culture results are available. Therefore, it is of utmost importance to know the common causative organisms in endophthalmitis and their antimicrobial susceptibilities. While certain risk factors and clinical presentations can suggest the causative organisms, these clinical associations are not reliable enough to narrow the antimicrobial treatment without culture results. Further, it is well known that the distribution of causative organisms and their sensitivities vary by region and time.
We report data from a tertiary referral center containing all positive vitreous cultures taken from January 1988 to December 2008. This study surveyed the trends of organisms causing endophthalmitis in Connecticut, since no past studies have been done in this region, with the goal of providing the most effective treatment regime to patients.
Methods
This retrospective study was approved by the Yale School of Medicine's institutional review board. Records of all vitreous samples sent to the Yale-New Haven Hospital Microbiology Laboratory from January 1988 to December 2008 were reviewed.
Bacterial and fungal isolates and their susceptibilities to antimicrobials were extracted from all cultures positive for growth. Bacterial susceptibilities were recorded as “resistant,” “intermediate,” and “sensitive”; however, for the purpose of the study, “intermediate” and “sensitive” were both considered sensitive to produce a dichotomous susceptibility variable. Guidelines from the Clinical and Laboratory Standards Institute were used for all susceptibility testing with breakpoints updated annually in January of each year.
To analyze trends over time, microbial isolates were divided into 3 equal time periods—1988–1994, 1995–2001, and 2002–2008—and the distribution of causative organisms and their susceptibilities were compared across the time periods. Exact Kruskal–Wallis tests for independence were run to assess for monotonic trends with time. If no monotonic trends were found, then exact Chi-squared tests of independence were used to evaluate existence of any trends with time, followed by Bonferroni adjustments on the standardized residuals to identify the statistically significant deviations from independence. All data collection and analysis were performed using Microsoft Excel 2008 and IBM SPSS Statistics version 19.
Results
A total of 160 isolates were yielded from 143 positive cultures of which 11.9% (n=17) were polymicrobial. Across all isolates, 80.6% (n=129) were gram-positive isolates, 12.5% (n=20) were gram-negative isolates, and 6.9% (n=11) were fungal isolates. However, the isolate type did vary with the time period (P=0.012) as characterized by an increase in gram-negative organisms (adjusted standard residual=2.5) and a decrease in gram-positive organisms (adjusted standard residual=−2.5) during the middle time period 1995–2001 compared with previous and later time periods (see Fig. 1).

Isolate type by time periods. Isolate type varied by time period (P=0.012) with an increase in gram-negative organisms (adjusted standard residual=2.5) and a decrease in gram-positive organisms (adjusted standard residual=−2.5) during 1995–2001 as compared with other time periods.
The most prevalent organisms were coagulase-negative Staphylococcus (CoNS) (37.5%, n=60), Viridans Streptococcus (11.3%, n=18), and Streptococcus pneumoniae (6.9%, n=11). Other common gram-positive isolates include Propionibacterium acnes (5.6%, n=9), other Streptococcus species (4.4%, n=7), Staphylococcus aureus (4.4%, n=7), and Enterococcus faecalis (3.8%, n=6). The most common gram-negative isolates were the Klebsiella species (3.1%, n=5), Moraxella species (3.1%, n=5), and Haemophilus species (2.5%, n=4). CoNS remained the most common causative organism during all time periods with 38.3% during 1988–1994, 36.6% during 1995–2001, and 38.1% during 2002–2008 (P=0.876). See Table 1 for full list of organisms and their variations over time.
Other gram-positive organisms include Peptostreptococcus species (n=1), Bacillus species (n=2), Clostridium species (n=2), and Corynebacterium species (n=2). Other gram-negative organisms include Capnocytophaga species (n=1), Citrobacter freundii (n=1), Eikenella corrodens (n=1), Proteus mirabilis (n=2), and unspecified gram-negative rods (n=1).
n, total number of isolates found; %, percentage of all isolates in time frame; CoNS, coagulase-negative Staphylococcus.
No bacterial isolates were found to be resistant to all antibiotics tested. Vancomycin was effective against all CoNS, Sta. aureus, Viridans Streptococcus, and E. faecalis tested. Further, no Sta. aureus isolates (n=7) were found to be methicillin-resistant Sta. aureus (MRSA) (oxacillin was used as the surrogate for methicillin similar to other studies3,4).
CoNS isolates were tested against cefazolin, cephalothin, chloramphenicol, clindamycin, erythromycin, gentamicin, oxacillin, penicillin, rifampin, tetracycline, Trimethoprim (TMP)/Sulfamethoxazole (SMX), and vancomycin. Of all CoNS isolates, 83.3% during 1988–1994, 73.1% during 1995–2001, and 100% during 2002–2008 were resistant to at least 1 of these antibiotics with the last time period showing an increase in resistance (P=0.021, adjusted standard residual=2.0) (see Fig. 2).
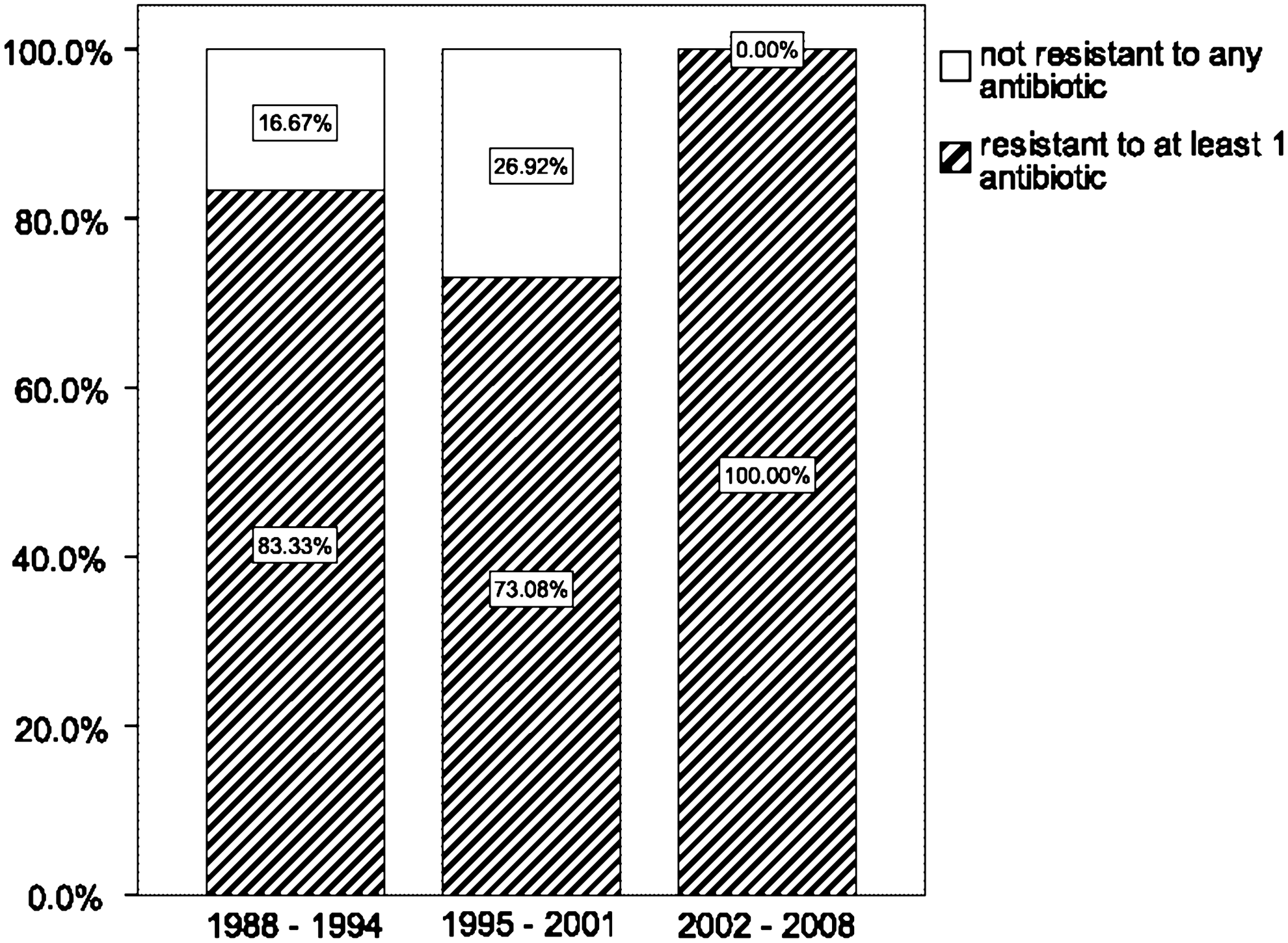
Distribution of coagulase-negative Staphylococcus (CoNS) isolates resistant to at least 1 antibiotic. Antibiotic susceptibility to at least 1 antibiotic varied with time (P=0.021), with the last time period 2002–2008 showing an increase in resistance (adjusted standard residual=2.0).
CoNS showed a decreasing resistance over time to chloramphenicol and gentamicin (P=0.010, P=0.007, respectively). In fact, all CoNS were susceptible to chloramphenicol after 1992 and to gentamicin after 1997. However, CoNS susceptibility to penicillin and tetracycline did not vary monotonically by time as measured by Kruskal–Wallis test (P=0.406, P=0.204), but susceptibility did show dependence on time by the exact Chi-squared test (P=0.003, P=0.040, respectively) that is characterized by an increase in resistance during the last time period 2002–2008 (adjusted standard residual=2.4, adjusted standard residual=2.1, respectively). Susceptibility to other antibiotics did not show significant dependence on time (see Fig. 3).

Antibiotic susceptibilities of CoNS. CoNS isolates were tested against cefazolin, cephalothin, chloramphenicol, clindamycin, erythromycin, gentamicin, oxacillin, penicillin, rifampin, tetracycline, TMP/SMX, and vancomycin. CoNS showed a decreasing resistance over time to chloramphenicol and gentamicin (P=0.010, P=0.007, respectively). However, CoNS susceptibility did not vary monotonically by time for penicillin and tetracycline (P=0.406, P=0.204), but susceptibility did show dependence on time (P=0.003, P=0.040, respectively) that is described by an increase in resistance during 2002–2008 (adjusted standard residual=2.4, adjusted standard residual=2.1, respectively). Susceptibility to other antibiotics did not show significant dependence on time as all P values were >0.05.
Discussion
When comparing the 160 isolates across all time periods, there was an increase in gram-negative organisms (adjusted standard residual=2.5) and a decrease in gram-positive organisms (adjusted standard residual=−2.5) during 1995–2001 as compared with previous and later years (P=0.012). CoNS remained the most common causative organism throughout time ranging from 38.3% during the first time period, 36.6% during the middle time period, and 38.1% during the last time period (P=0.876).
The Endophthalmitis Vitrectomy Study (EVS) data were collected between 1990 and 1994 on bacterial endophthalmitis following cataract extraction and secondary intraocular lens implantation. 5 This landmark study showed that out of 323 microbial isolates meeting criteria for confirmed growth, 94.2% (n=310) were gram-positive isolates, 5.9% (n=19) were gram-negative isolates, and 0% were fungal isolates. Compared to the EVS results, our data showed a statistically lower prevalence of gram-positive organisms (81.2%) with a higher prevalence of gram-negative (12.1%) and fungal organisms (6.7%) across all time periods (see Table 2). Further, in the 1988–1994 time period, which overlaps closest with the study period for EVS, our study showed an overall lower incidence of CoNS in our study (38.3%) compared with EVS (70.0%). There was also a shift toward increased incidence of Streptococcal species in our study (19.2%) compared to EVS (9.0%); however, both Staphylococcal and Streptococcal species remain most prevalent in both studies. Our study contained data on endophthalmitis from all causes whereas EVS only considered endophthalmitis after cataract extraction and secondary lens implantation. This difference may explain our study results reporting a higher incidence of gram-negative and fungal organisms that are more associated with non-postcataract endophthalmitis and a lower incidence of CoNS that is the most common cause of postcataract endophthalmitis.
P value calculated using 2-sided exact Pearson chi-squared between EVS and each time period in our study.
EVS, Endophthalmitis Vitrectomy Study.
The choice of empiric antibiotics is in constant evolution as new information becomes available. Current antibiotic protocols commonly start with intravitreal vancomycin for gram-positive coverage in combination with ceftazidime for gram-negative coverage. For individuals with beta-lactam allergy, amikacin is used with the possible side effect of retinal toxicity. Also important is that bacterial susceptibility varies by region and time. EVS showed 89.5% of gram-negative isolates to be sensitive to amikacin or ceftazidime, but in India, the susceptibility of gram-negative bacteria to amikacin or ceftazidime has only been 68% and 63%, respectively, during 1995–1998. 6 Fourth-generation fluoroquinolones like moxifloxacin and levofloxacin have been increasingly used for endophthalmitis. 7 Gram-positive organisms reportedly have 99% susceptibility to vancomycin 8 but recent reports of vancomycin-resistant strains have been reported9,10 and emerging resistance of gram-positive organisms to vancomycin is concerning. Fortunately, in our study, all tested gram positives, including CoNS, Sta. aureus, and E. faecalis, were sensitive to vancomycin and rifampin, while all tested gram negatives were sensitive to ceftazidime and ceftriaxone. The sensitivity to amikacin and fourth-generation fluoroquinolones was not regularly tested in our microbiology lab.
CoNS appear to be the most prevalent bacteria causing endophthalmitis throughout recent studies, including this one. While the prevalence of CoNS showed no variability throughout the time periods (P=0.876), the number of CoNS isolates resistant to at least 1 antibiotic showed an increase during the last time period with 83.3% during 1988–1994, 73.1% during 1995–2001, and 100% during 2002–2008 (P=0.021, adjusted standard residual=2.0). Further, CoNS showed a decreasing resistance over time to chloramphenicol and gentamicin (P=0.010, P=0.007, respectively) and an increasing resistance to penicillin and tetracycline during the last time period 2002–2008 (P=0.003, adjusted standard residual=2.4; P=0.040, adjusted standard residual=2.1). No other antibiotics, including cefazolin, cephalothin, chloramphenicol, clindamycin, erythromycin, oxacillin, rifampin, TMP/SMX, and vancomycin, showed any trend with time. Antibiotic resistance tends to follow the use of the medication in the general population, which may be the reason for the decreased resistance of CoNS to chloramphenicol, which is rarely used now secondary to side effects of aplastic anemia, and gentamicin, which is generally only used now for gram-negative infections. On the other hand, penicillin and tetracycline, along with other antibiotics in their class, have been continually used to treat common gram-positive organisms.
MRSA ocular infections are growing in absolute numbers and percentage of overall Sta. aureus infections.11,12 Additionally, MRSA also tend to exhibit resistance to fourth-generation fluoroquinolones,4,13 which are often used in endophthalmitis. Interestingly, our samples contained no strains of MRSA among the Sta. aureus isolates, which were also all sensitive to vancomycin.
Data for this study came from computerized reports of culture samples. The current study measures resistance in the in vitro setting of the microbiology lab as opposed to the clinical setting, where patients are likely to get higher intravitreal levels of antimicrobials as compared with the mean inhibitory concentration used in the in vitro studies. Resistance and sensitivity based on in vitro testing may not reflect true clinical resistance and response to an antibiotic because of host factors and drug penetration.
Endophthalmitis, in general, is a rare phenomenon, but its severe effects call for timely and effective treatment to prevent devastating vision loss. 1 The identity of the causative organism and sensitivities vary by region and by time. Symptoms can be variable from little inflammation in the anterior chamber and anterior vitreous to extremely painful panophthalmitis with no fundus view, corneal edema, or complete anterior chamber hypopyon. 14 Therefore, ophthalmologists must have high clinical suspicion for endophthalmitis. Determining the appropriate antimicrobial coverage for infectious endophthalmitis remains a significant clinical challenge. Because of the higher than expected incidence of gram-negative species in our study, we encourage continued careful evaluation of each patient and the use of empiric coverage for gram-positive and gram-negative species. Further research analyzing the trends in the microbiologic spectrum and antibiotic susceptibilities in cases of endophthalmitis stratified by specific etiologies would greatly aid the choice of empiric treatment. Resistance patterns need to be evaluated periodically because it is a dynamic phenomenon varying geographically and chronologically that cannot be extrapolated easily. The increased resistance to commonly used antibiotics found in this study reinforces the need for close follow-up after initial empiric treatment and maintaining low threshold for alternative therapy if there is indication of treatment failure.
Footnotes
Disclosure Statement
No competing financial interests exist for any authors.