
Abstract
Abstract
Purpose:
To evaluate the pharmacokinetics (PK) and tolerability of a proprietary sirolimus depot-forming ocular formulation in rabbits and humans after a single intravitreal (IVT) injection.
Methods:
New Zealand White (NZW) rabbits were intravitreally injected in both eyes with an injectable formulation in 5 (3 PK and 2 tolerability) studies. The rabbits received up to approximately 220 μg sirolimus per eye. At the desired timing post-injection, the animals were euthanized; both eyes were enucleated, frozen, and dissected to separate sclera, retina/choroid, and vitreous humor (VH). Whole blood (WB) samples were obtained at each time point before euthanasia. In clinical trials, patients received an IVT injection of approximately 352 μg sirolimus. Sirolimus concentrations in ocular tissues and WB samples were measured using liquid chromatography/tandem mass spectrometry (LC/MS/MS). In both single- and repeat-dose tolerability studies, systemic and ocular adverse effects were evaluated.
Results:
After IVT administration, sirolimus formed a depot in the VH. During dissolution, concentrations in VH were dose related and exhibited continuous release from the depot. This was characterized by a gradient of sirolimus concentration in the order of VH > retina/choroid > sclera > WB, and the concentrations were maintained for approximately 2 months after the IVT injection. After repeat dosing (132 μg), no drug accumulation was seen in the ocular tissue or systemically. In clinical studies, the highest blood levels were <2 ng/mL at day 2, and half-time (t1/2) was 8–9 days. There was no accumulation at day 30 after the IVT injection (up to 352 μg). Safety studies conducted on rabbits indicated good local tolerability. Sirolimus-related effects were limited to minor incipient cataract findings and mild lenticular changes. In the clinical studies where sirolimus was intravitreally administered up to 352 μg, injections were well tolerated.
Conclusions:
Sustained IVT delivery was achieved in a dose-dependent fashion after the IVT injection of a proprietary sirolimus depot-forming ocular formulation. Across the tolerability and safety studies, no significant findings were observed for systemic and ocular tolerability. The human WB levels were well below the daily trough systemic blood level range required for systemic immunosuppression. An IVT injection of sirolimus has a PK and safety profile that is favorable for treating inflammatory conditions of the eye, such as non-infectious uveitis, and warrants further investigation in humans.
Introduction
Sirolimus, also known as rapamycin, is a macrolide antibiotic that was isolated in the 1970s from Streptomyces hygroscopicus in soil samples from Easter Island. 5 Sirolimus arrests cell-cycle progression by direct interaction with 2 intracellular proteins, specifically the immunophilin FK binding protein 12 (FKBP-12) and the mammalian target of rapamycin (mTOR), a multifunctional serine–threonine kinase. 5 In cells, sirolimus binds to FKBP-12, and the resulting sirolimus: FKBP-12 complex then binds to and inhibits mTOR. The inhibition of mTOR blocks interleukin (IL)-2 mediated signal transduction pathways that prevent cell-cycle progression from G1 to S phase in T cells, endothelial cells, osteosarcoma cells, myogenic cell lines, and smooth muscle cells.6,7 In addition, sirolimus inhibits the production of antibodies.6,8 Sirolimus is approved for use as an immunosuppressive agent in renal transplants 9 and as a sirolimus/polymer-coated stent for improving coronary luminal diameter in patients with symptomatic ischemic disease. 10
In chronic uveitis, T-cell infiltration is responsible for recurrent episodes of inflammation that result in cumulative structural damage and a loss of vision. 11 Sirolimus blocks T-cell activation and inhibits the production of inflammatory cytokines (IL-2, IL-4, and IL-15).6,8 Sirolimus has been shown to reduce inflammation in animal models of experimental autoimmune uveitis and is being evaluated for its potential therapeutic use in humans.12–14 The purpose of this article is to characterize the ocular and systemic pharmacokinetics (PK) and tolerability of the IVT injection of sirolimus in rabbits and humans.
Methods
Injectable formulations
Initially, 3 different proprietary injectable formulations containing 0.2%, 0.6%, and 2% sirolimus were evaluated. The third formulation containing 2% sirolimus, referred to as 2% DE-109, was used in all subsequent studies and is a proprietary formulation owned by Santen (Osaka, Japan). It should be noted that sirolimus content is reported as weight/weight.
Injections
IVT injections were administered by a standard technique, and antibiotic ointment was applied post-injection. IVT injections of less than 10 μL were administered using a sterile 10 μL Hamilton syringe with a 30 gauge×½ inch needle. IVT injections of 10 μL were administered using a sterile 0.3 cc Becton Dickinson insulin syringe with a 29 gauge×½ inch needle. Proprietary sirolimus formulation was supplied as a sterile injectable solution, filled in a United States Pharmacopeia (USP) type 1 glass vial with a rubber stopper. Since the product was stored at −20°C, it was thawed at room temperature for 1 h before use. The IVT injections were administered using a needle introduced through the ventral-nasal quadrant (inferior) of the eye (i.e., 5 o'clock for the right eye and 7 o'clock for the left eye), approximately 2–3 mm posterior to the limbus.
Studies
Five (3 PK and 2 tolerability) studies characterize the IVT administration of sirolimus in New Zealand White (NZW) rabbits (Table 1). In-life portions for PK studies were conducted at the Biological Test Center (Irvine, CA), in-life portions for 2 tolerability studies were conducted at Charles River Laboratories (Redfield, AR), and the third study was conducted at NASA Ames Research Center (Moffett Field, CA). All studies treated research animals according to the guidelines of the Association for Research in Vision and Ophthalmology and in accordance with an appropriate Animal Care and Use Committee at the site where the work was conducted.
Three clinical studies were conducted (Table 2). These studies were conducted in accordance with Good Clinical Practice requirements described in the current revision of International Conference on Harmonization of Technical Requirements of Pharmaceuticals for Human Use Guidelines. Compliance with these regulations and guidelines also constitutes compliance with the ethical principles described in the current revision of the Declaration of Helsinki. These studies were also carried out in accordance with local institutional requirements.
PK studies in NZW rabbits
For PK studies, WB was collected at specified intervals in either rabbits or humans after IVT injections. Animals were euthanized at various times after injections, and both eyes were immediately enucleated for dissection. Since sirolimus forms a depot after the IVT injection, the vitreous humor (VH) was separated into 2 sections (with and without depot). Sirolimus levels from VH, retina/choroid, sclera, and WB were analyzed by liquid chromatography/tandem mass spectrometry (LC/MS/MS). The lower limits of quantitation were ≤0.6 ng/mL, 1.0 ng/g, 0.3 ng/g, and 0.05 ng/mL for VH, retina/choroid, sclera, and WB, respectively.
Tolerability studies in NZW rabbits
In both single- and repeat-dose tolerability studies, clinical observations, body weights, feed consumption, ophthalmology (examinations by a board-certified veterinary ophthalmologist), electroretinography (ERG), intraocular pressure (IOP), clinical pathology (hematology, coagulation, and clinical chemistry), organ weights, and gross and microscopic pathology were evaluated.
PK and safety studies in humans
The phase 1/2 study evaluated the safety and tolerability of sirolimus intravitreally administered in patients with macular edema associated with diabetic retinopathy (Study-6; NCT00401115) and those with age-related macular degeneration (Study-7, NCT00712491). The PK study was a single-masked safety and efficacy study. Sirolimus was administered via an IVT injection to 10 patients at a dose level of 352 μg/dose sirolimus (1056 μg as total of 3 doses), and WB samples were assayed by LC/MS/MS. The patients were carefully monitored for each study's desired terms (Table 2).
Results
Sub-acute PK in VH with or without depot after single dosing in NZW rabbits for 72 h
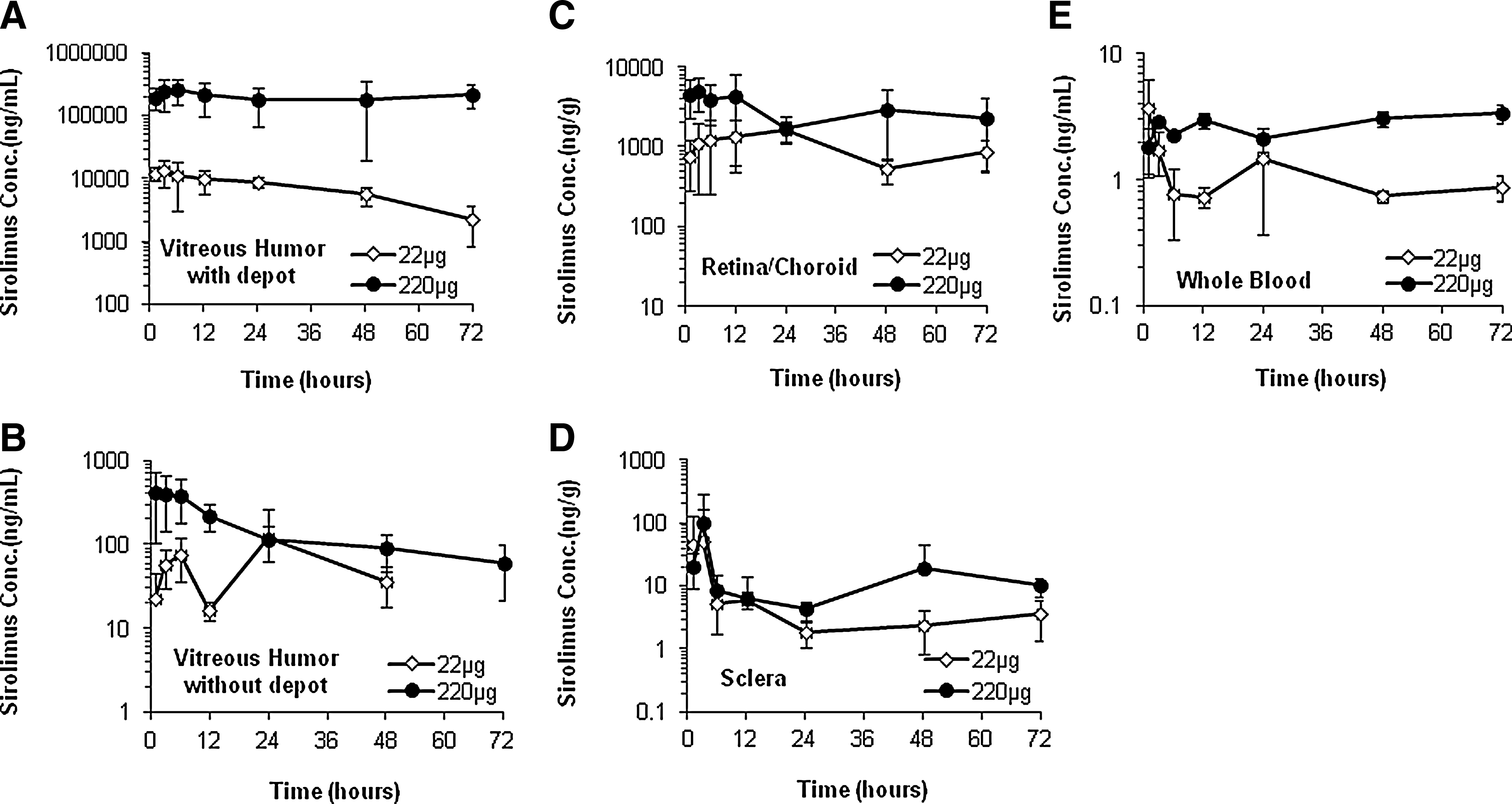
To explore the formation and dissolution of the depot, sirolimus levels in the VH were investigated in a sub-acute study (Study-1). The rabbits were administered 22 or 220 μg of sirolimus by an IVT injection in both eyes. Figure 1 shows the sirolimus level in VH with or without depot and sclera for 72 h after the IVT injection.
VH with
Before euthanasia, a depot was visually detected by an ophthalmoscopic examination. After euthanasia, it was also possible to visually identify the depot in some eyes during dissection of the VH. For those eyes that contained a depot, the part of the VH with the depot was separated from the rest of the VH at some of the time points and dose groups. When the depot was not visible during dissection, the entire VH was collected.
As expected, the sirolimus concentration in the depot portion of the VH was markedly higher than in the non-depot portion (over 2 orders of magnitude) (Fig. 1A, B). For the depot portion, sirolimus concentrations were dose related and disproportionately higher for the larger 220 μg dose, that is, approximately 16–24 times higher than the 22 μg dose. Sirolimus concentrations in the VH depot were maximal at 3–6 h post-injection (13188.3 and 263166.7 ng/mL for eyes injected with 22 and 220 μg, respectively). On the other hand, sirolimus concentrations in the non-depot portion of vitreous were relatively low, although they were also dose-related and disproportionately higher for the larger 220 μg dose. The maximum concentrations were 117.5 and 420.4 ng/mL for the eyes injected with 22 and 220 μg, respectively. The levels of sirolimus in the non-depot portion of vitreous reflect dispersion from the depot into the surrounding vitreous. These levels tend to fluctuate over time but still show a continuous release of the depot material. The appreciable concentration in the target tissues (retina/choroid) was achieved by an IVT injection (Fig. 1C). The tissue concentrations were generally less than dose-proportional, and exposure was maintained over a 72 h period after the injection, as would be expected with the slow diffusion of sirolimus from the depot. On the other hand, the sclera (layer) is relatively remote from the site of the IVT injection. For the first few hours post-injection, the sclera levels were in a range that was below the concentrations measured in the non-depot portion of VH, and they diminished substantially thereafter (Fig. 1D). This continuous exposure of target ocular tissue was achieved with minimal systemic exposure to sirolimus (Fig. 1E).
Long-term PK in VH with depot, retina/choroid, sclera, and WB levels after single dosing in NZW rabbits
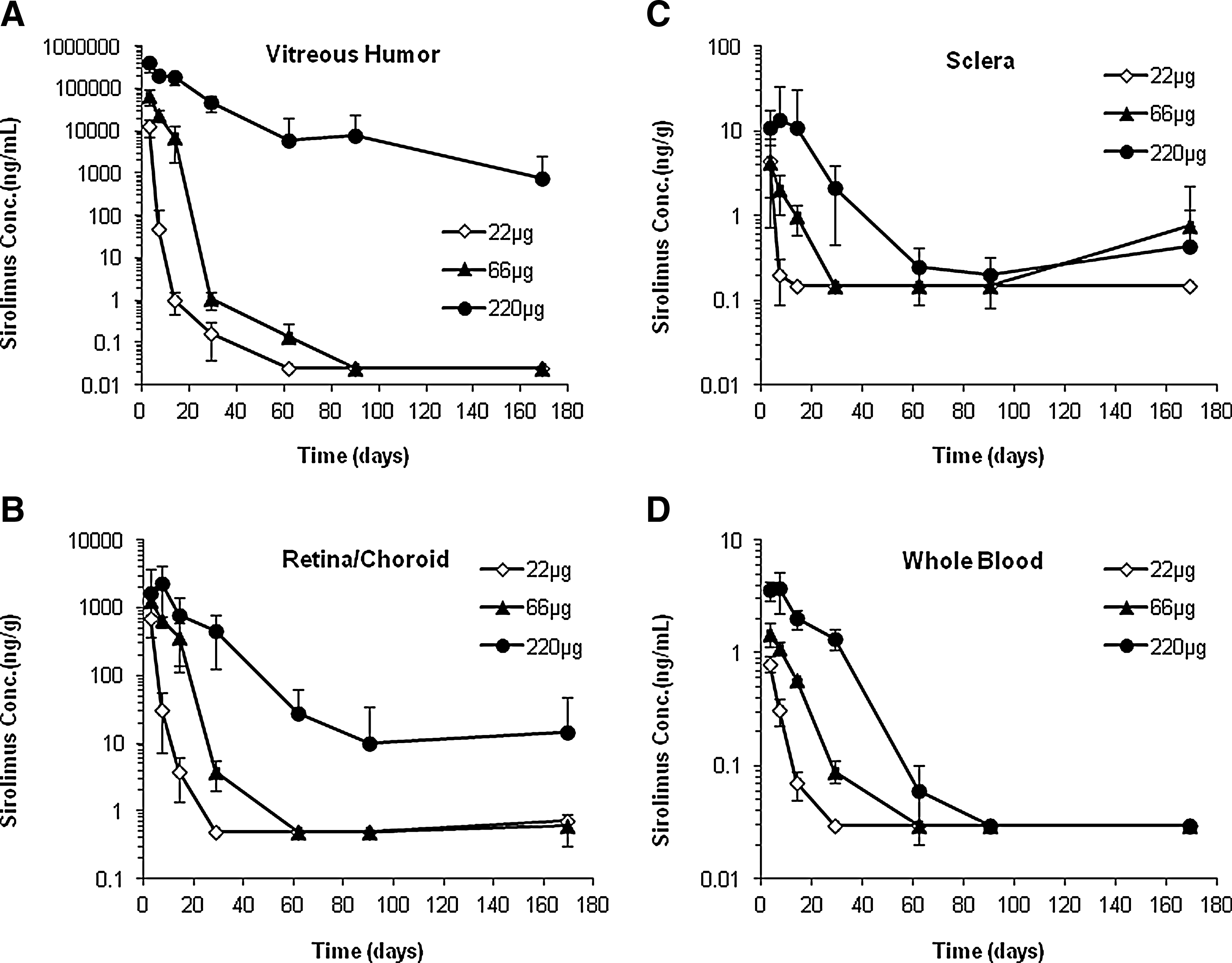
In a single-dose PK study (Study-2), the rabbits were administered 22, 66, or 220 μg of sirolimus by an IVT injection in both eyes.
VH levels
As observed in the sub-acute study just described, the depot could be visually detected, and it was possible to separate the part of the VH that contained the depot. Sirolimus concentrations in the depot portion were dose related (Fig. 2A). These levels diminished quite rapidly for the 22 μg dose, but appreciable concentrations persisted through day 14 for the 66 μg group and day 90 for the 220 μg group.
VH with depot
Retina/choroid levels
The retina/choroid levels of sirolimus across dose levels were dose proportional (Fig. 2B). The rate of decline was greater for the 22 μg dose and much slower for 66 and 220 μg dose levels. A sharp decline in tissue concentration occurred in the 66 μg group between days 14 and 29, while appreciable levels were present in the retina/choroid through day 29 for the 220 μg.
Sclera levels
The sclera levels of sirolimus across dose levels showed a dose response with the highest mean concentration observed on day 3 of 4.37 and 4.17 ng/g for the 22 μg and 66 μg doses, respectively (Fig. 2C). The highest sirolimus concentration for the 220 μg dose was observed on day 7 (13.52 ng/g).
WB/systemic levels
Sirolimus was detected in WB through day 14 for the 22 μg dose, day 29 for the 66 μg dose, and day 62 for the 220 μg dose (Fig. 2D). The highest concentrations were seen at the first sampling time point (day 3). The rate of decline was slow through day 14 for the 22 and 66 μg dose groups and day 29 for the 220 μg dose group.
PK after repeat dosing in NZW rabbits
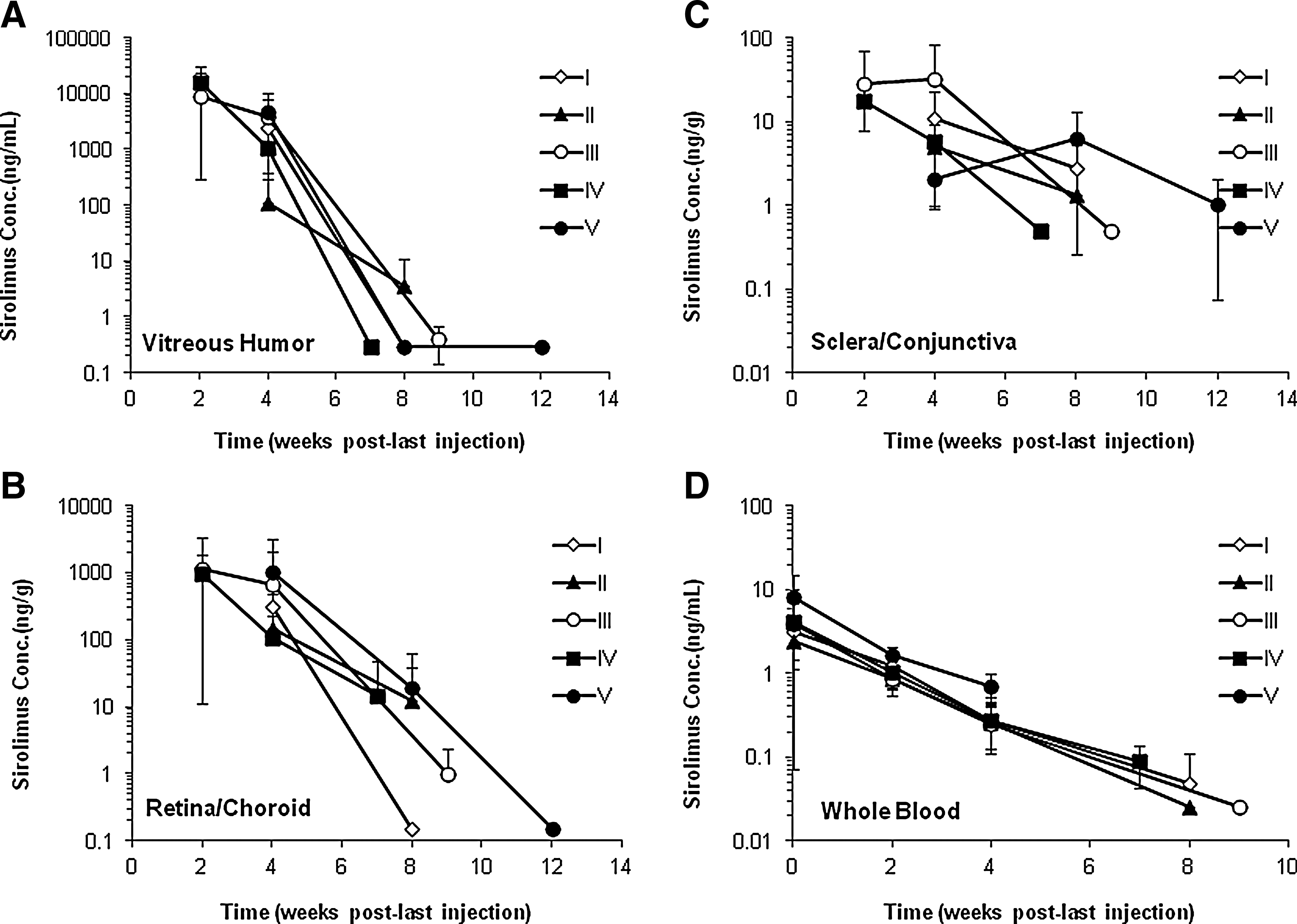
In a multiple-dose PK study (Study-3), the rabbits were administered 132 μg of sirolimus for approximately 5 injections. The injections were given approximately every 8 weeks over an 11-month period.
VH levels
After the first injection, 71% of the eyes had a visually detectable depot and after the fourth injection, 97% of the eyes had a visually detectable depot. As expected, the maximum sirolimus concentration was observed in the VH 2–4 weeks after approximately 5 IVT injections (Fig. 3A).
VH
Retina/choroid levels
At 2–4 weeks after each injection, the target tissue, retina/choroid, had significant levels of sirolimus (Fig. 3B), which remained for approximately 8 weeks. Sirolimus could be quantified in the sclera/conjunctiva tissues 2–4 weeks after each of the 5 IVT injections.
Sclera/conjunctiva levels
Sirolimus could be quantified in the sclera/conjunctiva tissues 4 weeks after each of the 5 IVT injections at a dose of 132 μg sirolimus/eye (Fig. 3C). By 7–12 weeks after the last injection of approximately 5 IVT injections, sirolimus levels in the sclera/conjunctiva tissues were either below quantification limit or minimally quantifiable.
WB/systemic levels
Peak systemic concentrations were observed in WB at 1 h after each injection at a dose of 132 μg sirolimus/eye (Fig. 3D). The highest level measured was 8.02 ng/mL (1 h after the last injection), which decreased to 1.64 ng/mL 2 weeks later. Sirolimus concentrations declined exponentially over time, with elimination half times (t1/2) of 8–9 days.
No accumulation
Sirolimus concentrations in the VH and retina/choroid were minimally quantifiable by 7–12 weeks after each injection. In WB, sirolimus levels were negligible within 2 weeks and became minimally quantifiable by 7–9 weeks after each injection. Furthermore, systemic exposure was transient and minimal after approximately 5 injections.
Tolerability and safety after IVT administration in NZW rabbits
Across the tolerability and safety studies (Table 1), no significant findings were observed for clinical observations, body weights, feed consumption, ERGs, IOP, organ weights, and clinical or gross pathology.
After single dosing (Study-4), ophthalmoscopic examinations did not reveal any apparent adverse effects. Vitreal inflammation and lenticular changes were mild and reversible. On days 27–29, there was an increased incidence in the pupillary response finding. Slow or no pupillary response was seen in 1 animal (2 eyes) in the 66 μg dose group. Pupillary light response may be commonly affected by elevated IOP, iris atrophy, mydriatic drugs, retinal degeneration, and sympathetic stimulation (flight or fight response). In the affected eyes, there was no evidence of increased IOP, iris atrophy, or retinal degeneration. Single IVT injections of 66 and 220 μg were well tolerated with the vitreal inflammation and lenticular changes of minimal severity and appearing to be reversible in nature.
After repeat dosing in Study-5, conjunctival discoloration and lacrimation, redness around the eyelids, and ocular discharge were observed and considered to be procedure related. Ocular microscopic findings included minimal swelling of the posterior lens fibers and the presence of epithelial cells in the posterior region of the lens. Minor incipient cataract findings were also considered to be sirolimus related.
PK after IVT administration in humans
PK data from clinical studies indicate that with IVT administration, systemic exposure was negligible. In a Phase 1/2 clinical study conducted in patients with diabetic macular edema (Study-7; Table 2), the highest sirolimus blood concentrations after single IVT injections were seen at day 2, with levels <0.5 ng/mL for doses of 44, 110, and 176 μg and <1.0 ng/mL for doses of 264 and 352 μg. In another study for age-related macular degeneration (Study-7), at an IVT dose of 352 μg, the maximum sirolimus concentration was 1.99 ng/mL, which is still well below the level that causes systemic immunosuppression (5–15 ng/mL). There was a clear dose-dependent change in both sirolimus concentration and duration of exposure. Sirolimus concentrations declined exponentially over time, with t1/2 of 7–8 days.
Tolerability and safety after IVT administration in humans
Across the clinical studies where sirolimus was intravitreally administered (Table 2), injections were generally well tolerated. Non-ocular adverse events and serious adverse events were infrequently seen and, in general, not related to study drugs. Adverse events considered related to the injection procedure, such as conjunctival hemorrhage and eye pain, were common after the IVT injection.
Discussion
Intraocular inflammation in uveitis causes retinal hemorrhages, retinal exudates, vitreous opacity, retinal detachment, retinal neovascularization, and cystoid macular edema. Most patients with uveitis have been treated with systemic corticosteroids or immunosuppressive agents such as cyclosporine and tacrolimus (FK506). Systemic administration of both corticosteroid and immunosuppressive agents can cause serious side effects. Many reports have shown the effects of IVT corticosteroids in patients with uveitis.15–17 However, corticosteroids have ocular serious side effects such as increased IOP and cataracts. When intravitreally administered, the drug's anti-inflammatory effect is confined to the eye, and systemic side effects are minimized. However, adequate therapeutic levels of drug should be reached and maintained in the target tissues when treating conditions such as posterior uveitis.
When sirolimus formulations are injected into the VH, sirolimus aggregates to form a depot. The major factors leading to the depot formation appear to be the hydrophobicity of sirolimus coupled with the relatively high viscosity of the sirolimus formulations. The VH is primarily composed of water. When the sirolimus formulation comes in contact with the VH, as a viscous droplet, it is believed that the excipients used in the formulation rapidly diffuse out of the droplet and water diffuses in, resulting in the local concentration of sirolimus becoming higher than its saturation solubility. As the local concentration of sirolimus reaches its saturation solubility, the drug subsequently precipitates to form a solid depot in lieu of the initial viscous droplet.
The PK of a depot-forming ocular formulation of sirolimus after the IVT injection was evaluated. Sirolimus precipitates to form a depot in the VH after the IVT administration of the injectable formulation. Once the depot is formed, the release of drugs is dependent on the dissolution rate of sirolimus into the VH, and the VH compartment with depot measured high levels of sirolimus compared with the one without depot (Fig. 1A, B). In the retina/choroid, sclera, and other ocular tissues, sirolimus levels were influenced by the levels in the VH compartment (Fig. 2). Transretinal diffusion of sirolimus from the vitreous through retina/choroid tissues to the sclera/conjunctiva tissues was evident from this study. The dissolution rate into VH, in turn, was dependent on the clearance of sirolimus from the VH into other ocular peripheral tissues, including retina/choroid. During this dissolution process, a near steady-state concentration of sirolimus was thought to be maintained in the VH.
In the repeated-dose PK study (Fig. 3), significant sirolimus levels were detected in the retina/choroid with concentrations ranging from 109 to 1050 ng/g 4 weeks after 1–5 injections. Sirolimus was quantified in the VH and target tissues at 2–4 weeks after the injection. These findings indicate the diffusion of intravitreally administered sirolimus to the target tissues and support the potential use to treat posterior uveitis. On the other hand, drug accumulation over time is a common concern for a potent immunosuppressant, especially for an agent that requires the monitoring of therapeutic blood levels. In the repeat-dose study, ocular concentrations of sirolimus (VH, retina/choroid levels, and sclera) were minimal by 7–12 weeks even after 5 injections (administered approximately 8 weeks apart). Levels in WB were negligible within 2 weeks and minimally quantifiable by 7–9 weeks after the drug administration. These findings indicate no drug accumulation in ocular tissue or WB with repeat dosing in rabbits. In a clinical study (Study-7), the highest blood levels were reported at day 2 and were <2 ng/mL with an elimination half life of 7–8 days (Fig. 4); this was close to 8–9 days in rabbits. These levels are well below the daily trough systemic blood level range (5–15 ng/mL) required for systemic immunosuppression.18,19 There was no accumulation at day 30 after the IVT injection (352 μg) bimonthly.
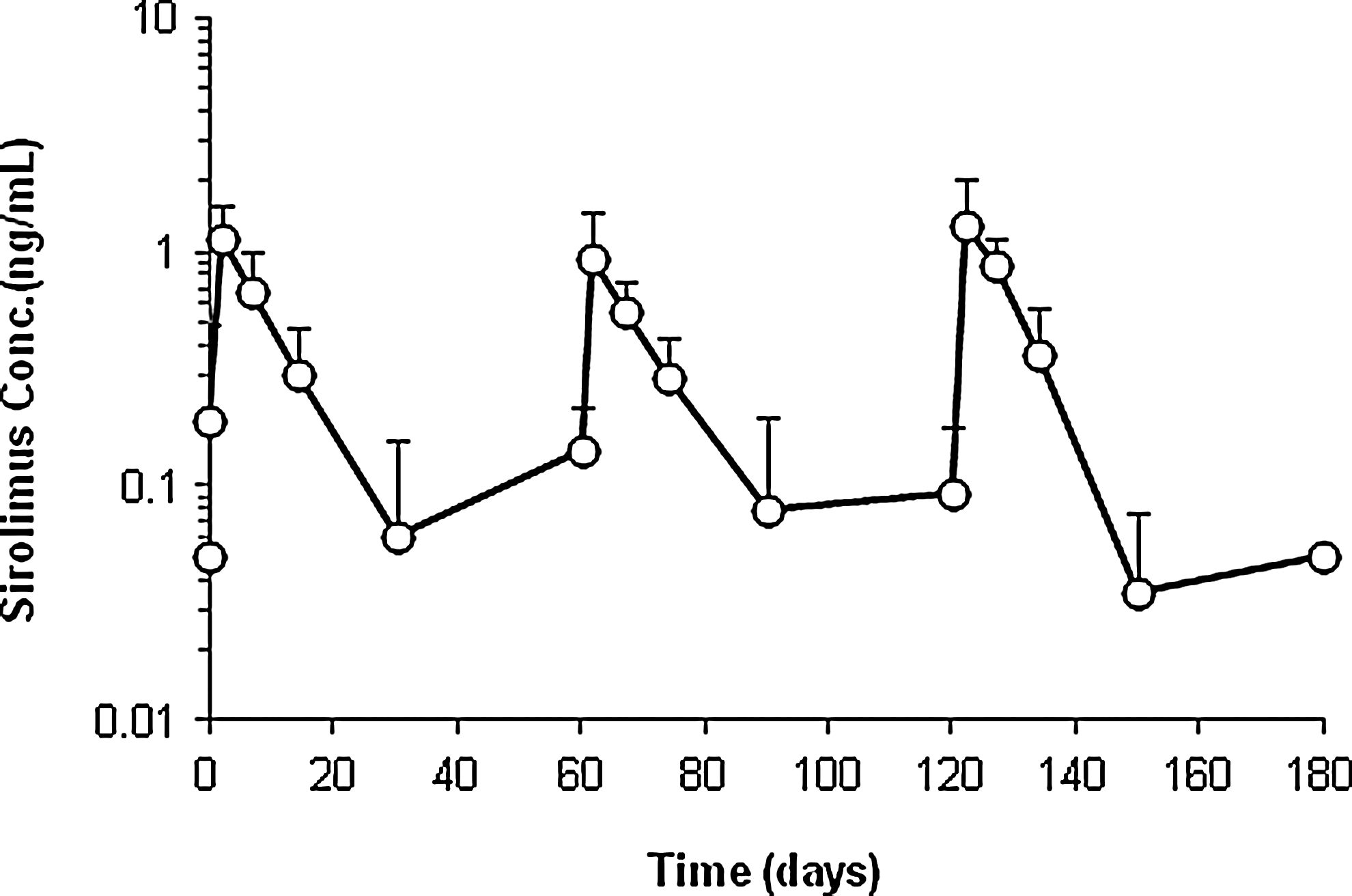
WB concentration of sirolimus after a repeat IVT injection every 60 days in patients. The study design is described as Study 7 in Table 2. Mean±SD, 6–10 eyes. WB samples were collected at baseline and on days 0 (60 min [±10 min] post-injection No. 1), 2, 7, 14, 30, 60 (60 min [±10 min] post-injection No. 2), 62, 67, 74, 90, 120 (60 min [±10 min] post-injection No. 3), 122, 127, 134, 150, and 180.
In the toxicology studies in NZW rabbits, sirolimus IVT injections were generally well tolerated. There were no sirolimus-related mortalities or changes in body weight, feed consumption, ERGs, IOP, organ weights, and clinical or gross pathology. Histopathology of ocular tissues revealed some sirolimus-related effects limited to lenticular changes, all of which were mild and reversible. These included increased incidence of minimal swelling of the posterior lens fibers and/or minimal epithelial cell presence in the posterior portion of the lens. These findings are consistent with the tolerability seen in another study that investigated potential retinal toxicity. 20 In Manzano's study, New Zealand albino rabbits received IVT doses of 20, 50, 200, and 1000 μg sirolimus. They performed slit-lamp and fundoscopic exams, and animals were observed for 2 weeks post IVT injection. The ERGs were performed at baseline and 14 days later; then, eyes were enucleated, and a histological examination showed no retinal damage. Follow-up ERGs showed some decrease in amplitude in the 50, 200, and 1000 μg, but this decrease was not dose related. In addition to this study, 20 we conducted preliminary toxicity studies in rabbits using IVT doses of approximately 880 μg; sirolimus appeared to be well tolerated.
In another study, ocular distribution of sirolimus was also evaluated in horses. 21 Animals scheduled for euthanasia due to orthopedic disease received IVT injections of 5 or 10 mg (n=2). One eye was injected with sirolimus, and the contralateral eye received 1 mL polyethylene glycol 400 intravitreally. One horse in each dose group was euthanized on day 7 or day 21. A depot could be visually detected after IVT administration. Measurable sirolimus levels were detected in both the aqueous and VH at 21 days after injection in horses. With IVT administration, there was a precedent for extrapolating doses across species based on the relative differences in the VH volume and lens size. For rabbits and horses, the vitreous volume has been reported to be 1.5 mL and 25 mL, respectively, whereas a range of volumes around 4.5 mL have been reported for the human eye. Based on those vitreous volumes, the maximum vitreous level (sirolimus/VH volume) were 667 and 400 μg/mL in rabbits and horses, respectively, and 78 μg/mL in humans dosed at 352 μg per eye.
The mild lenticular findings of the rabbit safety studies are unlikely to be seen in humans due to the anatomical difference between a rabbit and human eye. In rabbits, the smaller vitreal volume, larger lens, decreased retinal vascularity, and/or decreased aqueous humor outflow could have a potential impact on the rate of drug elimination, tissue distribution, thereby resulting in the minor ophthalmic and lenticular changes as shown in Study 4–6. In addition, inflammatory effects are known to be more pronounced in rabbit eyes than human eyes, as rabbit eyes are more sensitive to ocular drug formulations.
In order to explore the therapeutic potential of using an ocular formulation of sirolimus to treat non-infectious posterior uveitis in humans, a small pilot clinical study (SAVE 1) was conducted. Patients were required to have non-infectious posterior uveitis to participate and receive 352 μg every 2 months for 3 doses IVT (n=9). Sirolimus demonstrated bioactivity as an immune-modulatory therapeutic agent and a steroid-sparing agent in reducing vitreous haze and cells, improving visual acuity, and decreasing the need for systemic corticosteroids. 22 No dose-limiting toxicity, drug-associated ocular events, or systemic adverse events were noted in this study.
In conclusion, after IVT administration of sirolimus, the formation of a depot in the VH that dissolves over time allows continuous availability of sirolimus to the retina/choroid and other ocular tissues with negligible systemic exposure, thus reducing the potential of systemic side effects. The favorable PK and safety profile of intravitreally administered sirolimus makes it a promising candidate for the treatment of non-infectious posterior uveitis that warrants further investigation in well-controlled human trials.
Footnotes
Author Disclosure Statement
No competing financial interests exist.