
Abstract
Abstract
Purpose:
Bevacizumab, a monoclonal antibody targeting vascular endothelial growth factor (VEGF), specifically binds to VEGF protein, and inhibits angiogenesis. Intravitreal/intracameral injection of bevacizumab has been reported as another treatment option for patients with various ocular ischemic conditions. However, we report 4 cases of acute vision loss after bevacizumab intravitreal injection.
Methods:
Intravitreal bevacizumab injections were administrated to 2 ocular ischemic syndrome (OIS) patients and 2 central retinal vein occlusion (CRVO) patients. Best-corrected visual acuity (BCVA), intraocular pressure (IOP), funduscopic findings, and fluorescein angiography were evaluated before and after the treatments.
Results:
All 4 cases presented with acute vision loss within 1 week after bevacizumab injection, before its clearance from the eye, and showed that microcirculatory disturbances occurred in the retina.
Conclusions:
We believe that intravitreal injection of bevacizumab should be undertaken with extreme caution in patients with a history of cerebral infarction, especially with OIS or nonischemic CRVO, and with diabetic retinopathy and vitrectomized eye with pseudophakia.
Introduction
We report acute vision loss associated with retinal circulatory disturbances after an intravitreal injection of bevacizumab in patients with ocular and systemic ischemia, and suggest risk factors that may be associated with acute vision loss.
Case 1
A 72-year-old male patient with an 8-year history of hypertension and a history of recurrent brain infarctions, presented with decreased visual acuity in his left eye 5 months after cataract surgery. The best corrected visual acuity (BCVA) was 1.0 in his right eye (RE) and 0.5 in his left eye (LE). A slit-lamp biomicroscopic examination of the LE revealed neovascularization of the iris and anterior chamber angle, which was open without synechiae. The intraocular pressure (IOP) by Goldmann applanation tonometry was 16 mmHg in the RE and 32 mmHg in the LE. Fundus examination showed a few cotton wool spots, diffuse arterial narrowing but no new retinal vessels. Fluorescein angiography revealed hypofluorescence in the choroidal and retinal vessels of the LE. Magnetic resonance angiography indicated total occlusion of the left internal carotid artery (Fig. 1). The patient was diagnosed with OIS and was given the maximum tolerated medical treatment (Cosopt®, Alphagan®, and Travatan®) for 2 weeks, but his IOP remained high (25–32 mmHg). Therefore, off-label intravitreal and intracameral bevacizumab injections were recommended. The patient was fully informed about the treatment and possible side effects, and he provided written informed consent. We injected 1.25 mg (0.05 mL) of bevacizumab into the vitreous cavity of the LE and the paracentesis of anterior chamber was performed to reduce IOP. After IOP reduction was confirmed under sterile conditions, 0.02 mL of bevacizumab was injected into the anterior chamber. One day after injection, the patient reported deterioration of visual acuity in the LE. The BCVA in his LE was 0.02, and the IOP was 22 mmHg; Fundus examination showed extensive cotton wool spots and a cherry-red spot on the fovea. Fluorescein angiography of the LE showed diffuse nonperfusion including the fovea with blocked hypofluorescence (Fig. 1). Five months after injection, the BCVA in his LE was finger counting at 50 cm.
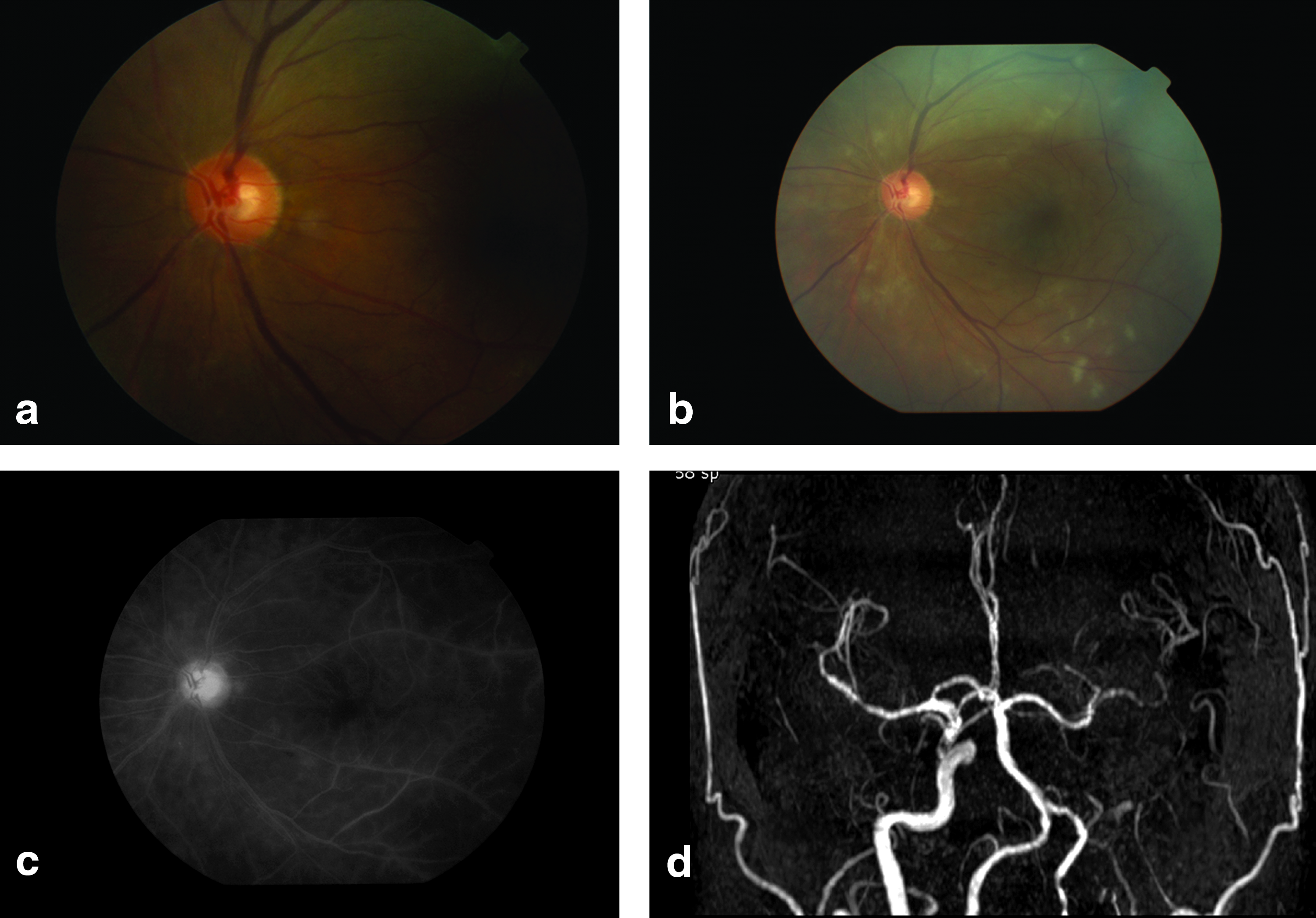
Fundus photographs, fluorescein angiogram, and magnetic resonance angiography of a patient with OIS, before and after intravitreal bevacizumab injection.
Case 2
A 57-year-old male patient with a 15-year history of diabetes was referred for decreasing visual acuity in his RE of 7-month duration. He had been treated with several retinal photocoagulations for diabetic retinopathy at a local eye clinic. He had a history of brain infarction and showed left-sided weakness. The BCVA was finger counting at 10 cm in his RE and 1.5 in his LE. Slit-lamp biomicroscopy showed neovascularization of the iris and anterior chamber angle of the RE. IOP by Goldmann applanation tonometry was 20 mmHg in the RE and 13 mmHg in the LE. Fundus examination showed multiple retinal hemorrhages, diffuse arterial narrowing, and macular edema. Fluorescein and indocyanine green angiography of the RE revealed very severe delayed filling in the choroid and severe retinal nonperfusion (Fig. 2). Carotid artery sonography showed nearly total occlusion of the right internal carotid artery, indicating OIS of the RE. He suffered from recurrent hyphema after the several retinal photocoagulations of his RE. Off-label bevacizumab injection was recommended, and the patient agreed to be treated with an intravitreal injection of bevacizumab (1.25 mg). One week after injection, the RE BCVA was no light perception and the IOP was 26 mmHg with Cosopt® treatment. Fundus examination showed extensive attenuation of the retinal vessels and whitening of the retinal arteries. Fluorescein angiography of the RE showed no filling of the retinal vessels except just around the optic disc. Five months later, right fundus examination showed a burned-out retina.
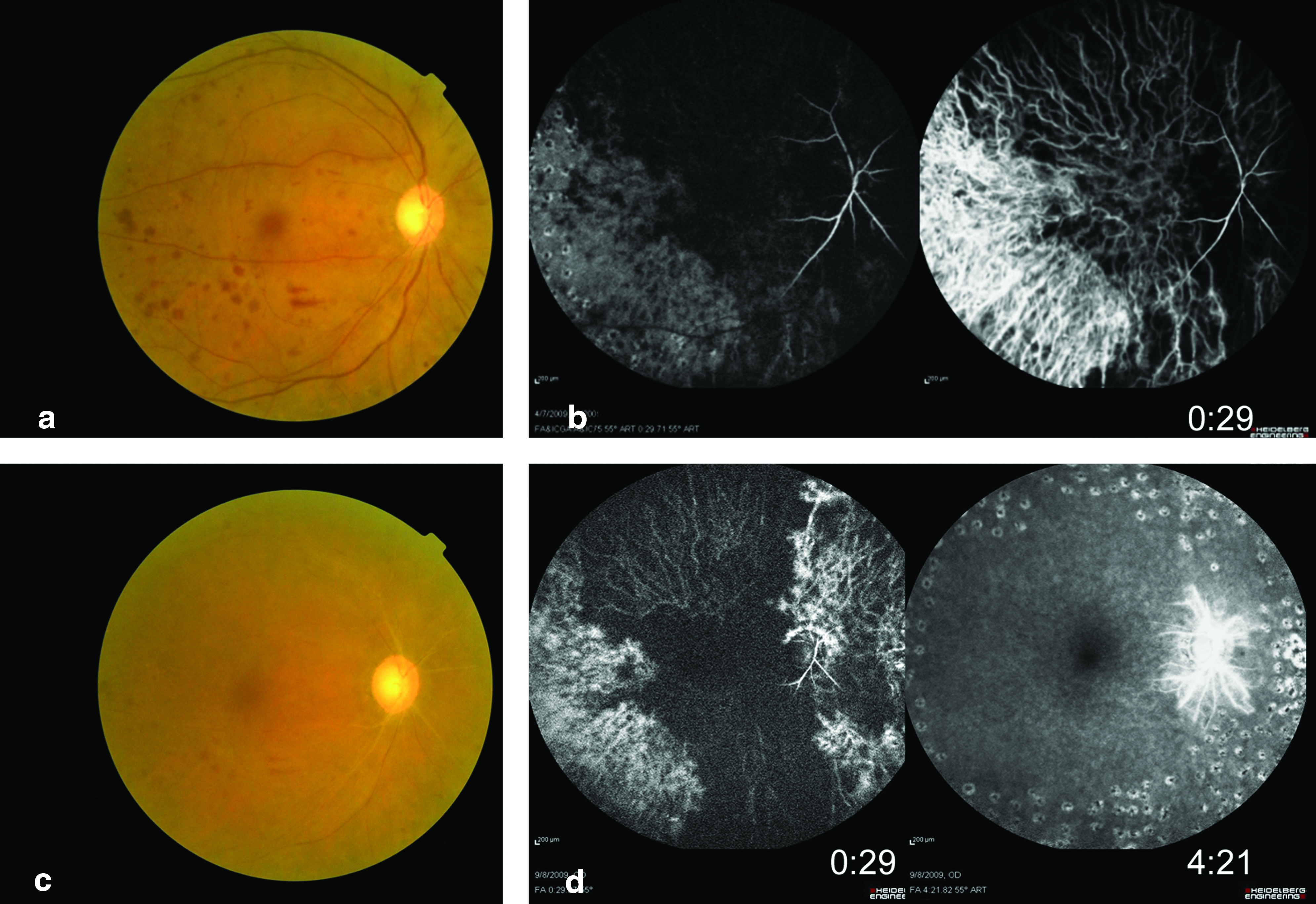
Fundus photographs, fluorescein angiogram, and indocyanine green angiography of a patient with OIS before and after intravitreal bevacizumab injection.
Case 3
A 60-year-old male patient with a 20-year history of diabetes presented with decreased visual acuity in his RE of 3-month duration. He had developed nonischemic CRVO in the RE 1 year previously. At that time, the BCVA was 1.0 in his RE and 1.0 in his LE, but at the time of presentation for decreased visual acuity, it was 0.2 in the RE and 1.2 in the LE. Slit-lamp biomicroscopy revealed severe iris and angle neovascularization. IOP by Goldmann applanation tonometry was 30 mmHg in the RE and 13 mmHg in the LE. Fundus examination of the RE revealed diffuse arterial narrowing and multiple dot-like retinal hemorrhages, but no new retinal vessels. Fluorescein and indocyanine green angiography of the RE revealed delayed filling in the choroidal and retinal vessels and diffuse leakage at the posterior pole, but no obvious occlusion of the retinal vessels (Fig. 3). We diagnosed the preproliferative diabetic retinopathy with OIS in the RE. We treated him with the maximal tolerable medical treatment for 2 weeks, but IOP remained high (26–30 mmHg). So we injected 1.25 mg of bevacizumab into the vitreous cavity of his RE. One week after injection, neovascularization of the iris and angle had regressed, but the patient reported deterioration of visual acuity in the RE. The BCVA in his RE was hand motion and the IOP was 26 mmHg with Cosopt® treatment. Fundus examination was unchanged from the exam 1 week previously. Fluorescein and indocyanine green angiography of the RE showed severe nonperfusion of the retina and choroid, including the fovea.
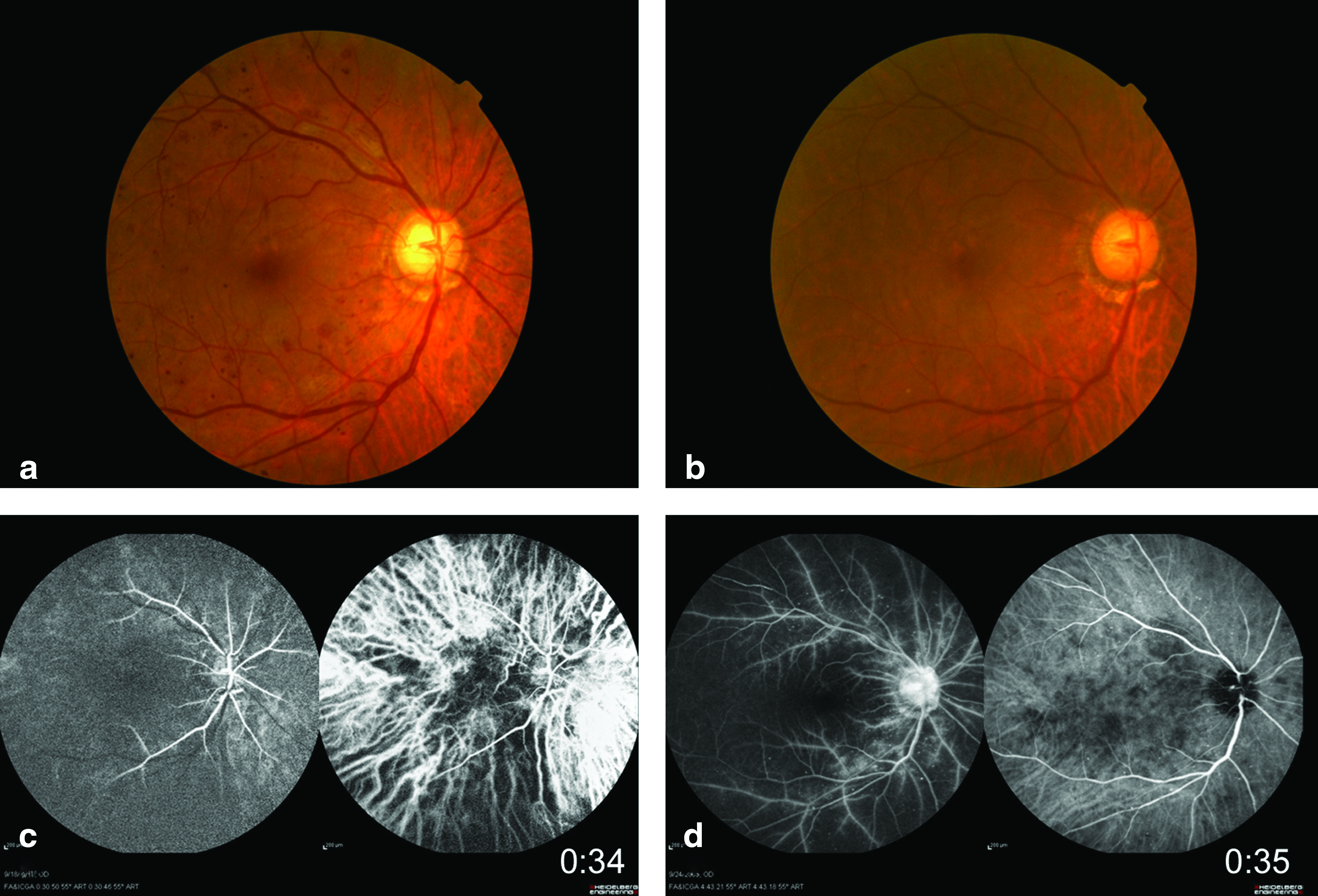
Fundus photographs, fluorescein, and indocyanine green angiography of a patient with nonischemic central retinal vein occlusion before and after intravitreal bevacizumab injection.
Case 4
An 82-year-old male patient with a 20/10-year history of diabetes/hypertension was seen for decreasing visual acuity in his LE of 8-month duration. He had developed nonischemic CRVO in the LE 8 months previously. At that time, the BCVA was 0.6 in his RE and finger counting at 50 cm in his LE, but at the time of presentation for decreased visual acuity, it was 0.4 in his RE and hand motion at 10 cm in his LE. Slit-lamp biomicroscopy revealed very severe new vessel in the iris and anterior chamber angle in the LE. IOP by Goldmann applanation tonometry was 11 mmHg in the RE and 33 mmHg with treatment using Cosopt® and Alphagan® in the LE. Fundus examination showed severe retinal hemorrhages, diffuse arterial narrowing, and macular edema. Fluorescein angiography of the LE revealed very severe delayed filling and diffuse leakage at the posterior pole, including around the optic disc. Carotid artery sonography indicated nearly total occlusion of the left internal carotid artery. One week after intravitreal injection of bevacizumab (1.25 mg), the LE BCVA was no light perception and IOP was 50 mmHg with Cosopt® and Alphagan® treatment. Fundus examination revealed extensive attenuation of the retinal vessels and whitening of the retinal arteries. Fluorescein angiography of the LE showed no filling of the retinal vessels except just around the optic disc. Four months later, photograph of the left fundus showed total sheathing of retinal vessels and a burned-out retina.
Discussion
Bevacizumab, a monoclonal antibody targeting VEGF, was approved by the United States Food and Drug Administration for systemic administration in patients with metastatic colon cancer. The use of intravitreal bevacizumab to treat ocular diseases was first reported by Rosenfeld et al. for CNV caused by age-related macular degeneration (AMD). 1 Intravitreal injection of bevacizumab is now used globally to treat diseases, including CNV caused by AMD, retinal vein occlusion, and PDR.
Systemic intravenous bevacizumab therapy for colon cancer can increase the risk of cerebral infarction, transient ischemic attacks, and myocardial infarction.2–4 However, the systemic effects caused by bevacizumab intravitreal injection are considered to be much less frequent and severe than those resulting from intravenous injection. But ocular adverse events, such as retinal pigment epithelial tears, inflammation, and lens injury, after intravitreal injections of bevacizumab have been recently reported.2–6 From among the side effects, the most critical is acute vision loss, which has been recently reported after intravitreal injection of bevacizumab for OIS and nonischemic CRVO.7–9
The pathophysiology of blindness after intravitreal injection of bevacizumab is not completely understood, but may be related to the vasoconstricting effect of anti-VEGF agents. VEGF acts as a vessel dilator by stimulating nitric oxide synthesis, and physiological levels of VEGF are thought to be necessary for retinal microcirculation. 8 Ultrastructural changes of choriocapillaris fenestrations have been reported after intravitreal bevacizumab injection in monkeys. 10 In addition, the pathophysiology may be associated with the IOP increase effect. Several reports enlighten the theory that IOP rise is followed by an intravitreal injection. A temporary elevation of vitreous volume leads to an IOP spike, which is shown to normalize within 1 h by studies with pegaptanib, another anti-VEGF.11,12 A probable explanation is the blockage of the trabecular meshwork in an ocular hypertensive patient by bevacizumab, a 148 kDa full-length antibody. Mordenti et al. 13 have reported that the clearance of the high-molecular-weight antibody from the vitreous is slow (half-life=5.6 days) with the internal limiting membrane, which acts as a barrier, and it further spreads from the vitreous to the anterior chamber. Hence, the drug might have accumulated in the trabeculum increasing the aqueous outflow resistance causing the IOP to rise acutely. This has 3-month-long effect. After considerable amount of time, the drug is clearly removed from the vitreous.
The increase in number of cotton wool spots after intravitreal bevacizumab injection in case 1 suggests that microcirculatory disturbances occurred in the retina. Diminished retinal microcirculation may also have been related to an increase in IOP up to a level that was intolerable to this eye, particularly with concurrent systemic and ocular ischemic conditions. Therefore, we always perform anterior chamber paracentesis simultaneously to prevent the increases in IOP during intravitreal injection.
Although the number of cases from which to draw conclusions is small, these findings reinforce the hypotheses that intravitreal injection of bevacizumab should be undertaken with extreme caution in patients with a history of cerebral infarction, especially with OIS or nonischemic CRVO, and with diabetic retinopathy and vitrectomized eye with pseudophakia, especially with great caution about intracameral injection of bevacizumab. The relatively high dose of bevacizumab may affect the retinas of these patients. We believe that intravitreal bevacizumab injection was related to the outcomes in our cases, because all our patients presented with acute vision loss within 1 week after bevacizumab injection, before its clearance from the eye.
Bevacizumab could be a valuable adjunct in treating many ocular ischemic conditions. But our findings indicate that particular care should be taken after an intravitreal bevacizumab injection in order to minimize microcirculatory disturbances of the retina, especially in patients with the previously mentioned risk factors. Additional large long-term studies of the effects of bevacizumab on retina circulation are necessary.
Footnotes
Author Disclosure Statement
None to declare.