
Abstract
Abstract
Purpose:
Corticosteroids, the main treatment option in acute attacks of ocular Behcet's disease (BD), are ineffective in preventing recurrent inflammation. Even combined therapy with systemic corticosteroids and azathioprine, cyclosporine, chlorambucil, or cyclophosphamide may be ineffective in controlling the disease in severe cases. We report our clinical experience with the efficacy and tolerability of interferon alpha-2a (IFN-α-2a) monotherapy in patients with Behcet uveitis refractory to conventional immunosuppressive agents.
Methods:
We retrospectively analyzed the medical records of 12 Turkish Behcet patients who had been treated with IFN-α-2a between February 2009 and October 2011 because of severe uveitis refractory to traditional immunosuppressants. IFN-α-2a was initially administered at 4.5×106 IU/day subcutaneously; then, the dosage was tapered gradually depending on the clinical response. Previous immunosuppressive drugs such as systemic corticosteroids, azathioprine, and cyclosporine were stopped 1 day before the initiation of IFN-α-2a treatment.
Results:
The mean duration of IFN-α-2a use was 13.3 months (range: 3–28 months). Eighty-three percent of patients with ocular BD achieved partial or complete response. Best-corrected visual acuity improved or remained stable in all of patients. All patients experienced flu like symptoms responding to oral acetaminophen, hair loss was also developed in 7 of them (58%), and psoriatic skin rash was seen in 3 patients (25%) during treatment with IFN-α-2a. No other side effects were observed.
Conclusions:
IFN-α-2a treatment is effective in Behcet uveitis refractory to traditional treatment regimens and provides significant improvement in visual prognosis.
Introduction
While corticosteroids are the main treatment option in acute attacks of ocular BD, they are ineffective in preventing recurrent inflammation, and adverse effects limit their long-term use. 10 Systemic corticosteroids can be combined with 1 or more of the following drugs: azathioprine, cyclosporine, chlorambucil, and cyclophosphamide. In severe cases, conventional therapy may be ineffective in controlling the disease, or the side effects may limit their use in BD. Biologic agents, used in the treatment of juvenile idiopathic arthritis, rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, and inflammatory bowel disease, target molecules functioning in the inflammatory process. 13 Biological drugs, first used in the late 1980s to treat ocular inflammation, improved the visual prognosis in patients with BD. 11 In 1986, interferon alpha-2a (IFN-α-2a) was introduced in the treatment of BD, as herpes simplex virus type 1 was considered as playing a role in the pathogenesis of BD. 14 IFN-α has been included in the European League Against Rheumatism 2008 guidelines as a second-line agent for the treatment of BD. 10 Although recent studies revealed that IFN is effective in BD, there is no consensus about the ideal dose or the duration of therapy.4–7,12,13,15–17 Flu-like symptoms, the most common side effects of IFN-α-2a during the first weeks of the therapy, do not require dose reduction; but some of the side effects such as hair loss, psoriatic skin rashes, neutropenia, elevated liver enzymes, epilepsy, development of antinuclear or antithyroid antibodies, and depression may require dose reduction or discontinuation of the therapy.
IFN-α-2a and anti-tumor necrosis factor α (TNF-α) are the most frequently studied biological agents. However, there are still questions to be answered on the use of biological agents in Behcet uveitis. Due to the cost and the limited experience about the long-term results of biological drugs, their use in uveitis remains restricted to patients refractory to traditional treatment regimens. 13 Although there are some reports on the efficacy and tolerability of IFN-α-2a in patients with ocular BD in literature, in most of these studies, IFN-α-2a was used in combination with systemic corticosteroids. The aim of this study is to report our clinical experience with the efficacy and tolerability of IFN-α-2a monotherapy in patients with Behcet uveitis refractory to conventional immunosuppressive agents.
Methods
We retrospectively analyzed the medical records of 12 Turkish patients with BD who had been treated with systemic IFN-α-2a between February 2009 and October 2011. All these patients met the international diagnostic criteria of the International Study Group for BD and underwent a complete ophthalmic examination, including visual acuity, measurement of intraocular pressure using a Goldmann applanation tonometer, slit-lamp biomicroscopy, and fundoscopy. Visual acuity was measured using the Snellen chart. Digital color fundus photographs, fluorescein angiography (FA), and optical coherence tomography were performed when necessary. All patients had a sight-threatening eye disease, and all of them had previously been treated with different systemic treatment regimens, including corticosteroids, azathioprine, and cyclosporine.
Human recombinant IFN-α-2a (Roferon-A; Hellas SA, Athens, Greece) was initially administered at 4.5×106 IU/day subcutaneously at bed time. All other systemic immunomodulatory agents, including corticosteroids, azathioprine, and cyclosporine, were discontinued 1 day before the initiation of IFN-α-2a treatment. Oral acetaminophen was offered to all patients because of flu-like symptoms, a well-known side effect of the IFN-α-2a treatment. Patients with anterior uveitis were also prescribed topical corticosteroids whenever necessary. On complete disease resolution, IFN-α-2a dose was tapered to 4.5×106 IU thrice a week and later on, it was further tapered to 3×106 IU thrice a week. Patients were informed about the possible adverse effects of the therapy. All patients were examined weekly for 2 weeks, every 2 weeks for 1 month, and then every 4 weeks. A complete ophthalmic examination was performed at every control visit. FA was performed when reducing or discontinuing IFN-α-2a. Complete blood count and routine biochemical tests including thyroid functions were performed on a monthly basis. Systemic adverse effects and relapses were recorded.
Results
The medical records of 12 patients who met the international diagnostic criteria of the International Study Group for BD were analyzed. There were 3 women (25%) and 9 men (75%). The mean age was 32.2 years (range: 21–46 years); the mean duration of BD was 6.1 years (range: 1–14 years); and the mean age at onset of BD was 26.2 years (range: 15–32 years).
Before IFN-α-2a therapy, 3 patients (25%) received prednisone, azathioprine, and cyclosporine; 4 patients (33%) received prednisone and cyclosporine; 4 patients (33%) were treated with prednisone and azathioprine; and 1 patient (9%) received only prednisone. These treatment regimens were discontinued, and IFN-α-2a therapy was started because of occlusive periphlebitis in 6 patients (50%) (Fig. 1) and refractory cystoid macular edema in 6 patients (50%) (Fig. 2).

Occlusive periphlebitis in fluorescein angiograms of patient 9
Optic disc hyperfluorescence, cystoid macular edema, and vascular leakage in fluorescein angiograms of patient 5
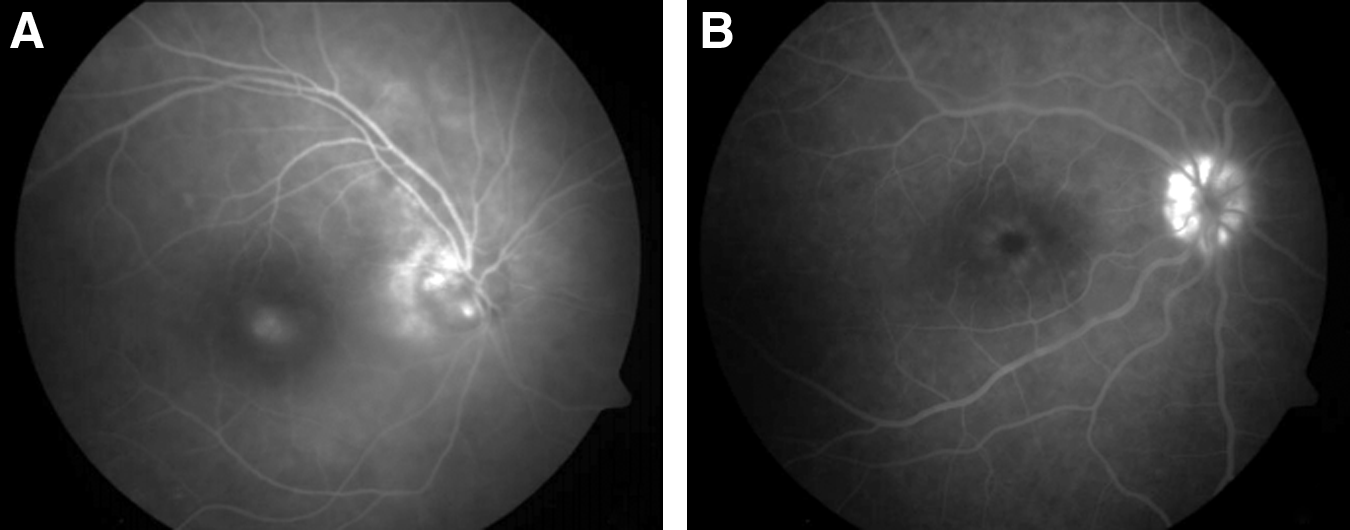
The mean duration of IFN-α-2a therapy was 13.3 months (range: 3–28 months). Nine patients are still on IFN-α-2a treatment. In patient 1, IFN-α-2a was switched to infliximab by rheumatologists due to severe arthritis that developed 3 months after the initiation of IFN-α-2a. During the period of IFN-α-2a therapy, the patient remained quiescent. Patient 2 discontinued IFN-α-2a treatment at month 5. A relapse occurred 1 week later, for which IFN-α-2a was resumed at 4.5×106 IU/day. Hyperfluorescence of the optic disc during recurrence in patient 2 is shown in Fig. 3A. After rearrangement of IFN-α-2a therapy, the optic disc was normal (Fig. 3B). Seven months later, another relapse developed, and IFN-α-2a therapy was switched to infliximab. Patient 3 received IFN-α-2a for 28 months. During this period, only one attack of posterior uveitis was seen at the fifth month of the therapy. IFN-α-2a treatment was stopped during the 28th month because of complete remission. The patient remained in remission for a follow-up period of 4 months.

Fluorescein angiograms of patient 2. Optic disc hyperfluorescence and diffuse capillary leakage during the recurrence of posterior uveitis because of the discontinuation of IFN-α-2a therapy by the patient
Six of the remaining 9 patients (67%) who were still being treated with IFN-α-2a had no more relapses during treatment. In patients 4 and 5 (22%), the dosage was increased to 4.5×106 IU thrice a week because of relapse at the dose of 3×106 IU thrice a week. No recurrence occurred for 9 months in patient 4 and for 4 months in patient 5 after the dose had been increased. A posterior uveitis attack occurred in patient 6 at the dosage of 4.5×106 IU every other day at the eighth month; the dose was increased to 4.5×106 IU/day, which resulted in complete disease resolution, and the patient remained relapse free for 2 months.
Six patients (50%) with mild anterior uveitis attacks responded well to topical corticosteroids. In the remaining 6 patients (50%), neither anterior nor posterior uveitis developed during the treatment.
Visual outcomes of patients treated with IFN-α-2a were also analyzed in 24 eyes of 12 patients. Best-corrected visual acuity (BCVA) improved at least 2 lines in 7 eyes (29%), and remained stable (±2 lines) in 17 eyes (71%). BCVA did not decrease in any eye. Initial and final visual acuities of each patient are summarized in Table 1.
VA, visual acuity; LP, light perception.
All patients experienced flu-like symptoms (low-grade fever, chills, fatigue, weakness, headache, muscle, and joint aches) during the first week of treatment with IFN-α-2a. Oral acetaminophen was used for relief of flu-like symptoms in all patients. Hair loss was also seen in 7 patients (58%). In 3 patients (25%), psoriatic skin rash developed while taking IFN-α-2a therapy. None of these side effects required dose reduction or discontinuation of the therapy. No other side effects were observed. Patient characteristics are summarized in Table 2.
CS, corticosteroids; CS-A, cyclosporine-A; AZA, azathioprine; MAU, mild anterior uveitis; PU, posterior uveitis; FLS, flu-like symptoms; HL, hair loss; PSR, psoriatic skin rash; IFN-α-2a, interferon alpha-2a.
Discussion
Ocular involvement, one of the most serious manifestations of BD, can result in severe visual loss in patients with BD.6,10,17 Treatment with systemic corticosteroids, azathioprine, and/or cyclosporine may be inadequate for preventing attacks and maintaining visual acuity.6,18 In long-term therapy, azathioprine and cyclosporine may also cause severe side effects, and relapse rates are high while reducing the doses of these drugs. 19 Colchicine, used for mucocutaneous lesions and arthritis in BD, is ineffective in uveitis attacks. Cyclophosphamide and chlorambucil can also be used for uveitis, but there are no sufficient studies available about their use in BD.
There are reports on the use of biological drugs such as anti-TNF-α, recombinant IFN-α, and monoclonal antibodies against interleukins (e.g., IL-2 and IL-1β) and vascular endothelial growth factor in uveitis.4,13 Recent reports indicate that IFN-α-2a therapy is effective in sight-threatening Behcet uveitis refractory to traditional treatment regimens.5–7,10,11,15,16,18–20
Corticosteroids are considered as antagonizing the immunomodulatory effect of IFN-α-2a by blocking nuclear factor kappa-light-chain-enhancer of activated B cells. 7 IFN-α combined with azathioprine can also cause myelosuppression. 21 Therefore, we discontinued second-line immunosuppressants and corticosteroids before IFN-α-2a. 13 However, in some studies, IFN-α-2a was initiated in association with corticosteroids. Bodaghi et al. treated patients with intravenous methylprednisolone 1 g/day for 3 days followed by oral prednisone (1 mg/kg/day) before IFN-α-2a therapy in all patients with refractory and sight-threating uveitis and started to taper the doses gradually 1 month after the initiation of IFN-α-2a. 20 In another study, Gueudry et al. administered IFN-α-2a therapy in the same way. 12 Krause et al. tapered corticosteroids to a maintenance dose of 10 mg/day and after a 6-month inflammation-free period, the corticosteroids were discontinued. 6 In Kötter et al.'s study, the corticosteroids were reduced to a maximum of 10 mg/day within 1–5 days, and the patients continued to take corticosteroids until complete remission of ocular disease after the initiation of IFN-α-2a treatment. 19 Onal et al. used the same protocol with that study and administered periocular or systemic corticosteroids (1 mg/kg/day) during a relapse to achieve rapid control. 5 Immunosuppressive drugs were ceased before the initiation of IFN-α-2a therapy in all of these studies.
In the literature data, some of the authors administered 6×106 IU/day IFN-α-2a;7,11,15,16,19 in some studies, IFN-α-2a was administered 3×106 IU/day; 5 and in the others, the patients received IFN-α-2a 3×106 IU thrice a week12,20 initially. In the current study, IFN-α-2a was initiated 4.5×106 IU/day, and systemic corticosteroids and immunosuppressive drugs were rapidly tapered and discontinued before the initiation of IFN-α-2a.
In the present study, 6 of the 12 patients (50%) remained relapse free during treatment. Five patients (42%) developed at least 1 relapse, but only one of them required switching to infliximab. The response rates with IFN-α-2a treatment were reported as being 78% by Krause et al., 6 88% by Gueudry et al., 12 91% by Tugal-Tutkun et al., 11 92% by Kötter et al., 16 and 95% by Onal et al. 5 In another study, all 7 patients included in the study achieved complete remission. 16 In Deuter et al.'s series, 98% of the patients responded to IFN-α-2a. 7 In our study, 83% (n=10) of the patients with ocular BD achieved partial or complete response. Of the responders, 4 patients (40%) had only mild anterior uveitis attacks, and these were considered partial responders. Six patients (60%) without any uveitis attack were accepted as complete responders.
In this study, BCVA, compared with baseline, improved (29%), or remained stable (71%) in all of the eyes. Stable or improved visual acuity was reported for 87.5% of the patients in a study by Gueudry et al., 12 for 92% of the patients in a study by Krause et al., 6 for 95% of the patients in a study by Tugal-Tutkun et al., 11 and for 97% of the patients in a study by Kötter et al. 19
Flu-like symptoms, the most common side effects of IFN therapy, tend to be most pronounced during the first month of the treatment and to diminish as treatment progresses, but these symptoms may be seen throughout therapy. An injection of IFN-α-2a before bed time is helpful; therefore, these symptoms will be limited primarily within the sleeping hours. In this study, all patients developed flu-like symptoms, in accordance with the literature data. Hair loss and psoriatic skin rash were also seen throughout follow up. These side effects did not require discontinuation or dose reduction of IFN-α-2a treatment. Leucopenia, itching, elevated serum liver enzymes, thyroid hormone disturbances, and development of autoantibodies are the other side effects that can also be observed with IFN-α-2a therapy.6,11,13,19,20 Depression and suicide attempts have also been reported in association with IFN-α-2a use. None of these adverse effects were encountered in the current study. Onal et al. adjusted a low-dose IFN-α-2a with dose escalation to avoid potential dose-dependent adverse effects of IFN-α-2a. 5
The limitations of the study are insufficient follow up after discontinuation of IFN-α-2a and inadequate number of patients. These results merely reflect our clinical experience. Although the effect of IFN-α-2a could not be neglected, randomized, controlled trials are required to describe the superiority of IFN-α-2a over standard immunosuppresants and to determine the optimum dosage and duration of the therapy. In conclusion, we propose the use of IFN-α-2a monotherapy in Behcet uveitis refractory to traditional treatment regimens.
Footnotes
Acknowledgment
The authors thank Radgonde Amer, M.D., for revision of the article.
Author Disclosure Statement
No competing financial interests exist.