
Abstract
Abstract
Purpose:
The purpose of the present study is to evaluate the effects of a fixed combination of 0.5% timolol maleate (TM) and 1% dorzolamide hydrochloride (DZ) (FCTD1%) on optic nerve head (ONH) blood circulation.
Subjects and Methods:
A drop of 0.5% TM, 1% DZ, or FCTD1% was topically administered to the right eyes of 15 healthy Japanese subjects, and a drop of saline was likewise administrated to their left eyes. Systemic blood pressure, heart rates (HRs), intraocular pressures (IOPs), ocular perfusion pressures, and blood circulation by a laser speckle flowgraphy at the ONH were measured before administration, and again at 1.5 and 6 h afterward.
Results:
FCTD1% caused a significant increase in ONH blood circulation 6 h after the administration, while 0.5% TM and 1% DZ had no significant effect. The IOPs were significantly decreased in 0.5% TM (P<0.01) and FCTD1% (P<0.05) when compared with the saline-treated eyes at 1.5 and 6 h after administration, while 1% DZ did not show a statistically significant decrease. There were no significant changes in other systemic parameters except for a significant transient decrease in the HRs observed in 0.5% TM (P<0.01) when compared with the baseline at 1.5 h after the administration.
Conclusion:
Our current results suggest that FCTD1% caused a significant increase in ocular blood circulation on the ONH in healthy Japanese subjects, presumably by a synergistic effect of 0.5% TM and 1% DZ, although neither 0.5% TM nor 1% DZ on their own had a significant effect.
Introduction
For the purpose of lowering IOP levels in patients with GON, many anti-glaucoma medications are available. Among these, recently fixed combinations of several anti-glaucoma drops have been frequently used in our glaucoma clinic, requiring a better compliance of the anti-glaucoma medication. In Japan, a fixed combination of 0.5% TM and 1% DZ fixed combination of 0.5% timolol and 1% dorzolamide hydrochloride (FCTD1%) has been available since 2010. In other countries, a different fixed combination composed of 0.5% TM and 2% DZ (FCTD2%) had already been used, and several reports have been published concerning its efficacy in lowering IOP levels and increasing the retrobulbar hemodynamics.8–10 However, in contrast, no study of FCTD1% is available as yet in terms of its efficacy toward ocular hemodynamics. It is, therefore, of great interest to know whether the FCTD1% affects ONH blood circulation, as it has been reported that DZ improves the ocular hemodynamics.11–13
In the current study, to determine these possible effects, we evaluated the effects of 0.5% TM, 1% DZ, and FCTD1% FCTD1% on ONH blood circulation in eyes from healthy subjects.
Methods
Subjects
The current study was conducted on 30 eyes from 15 healthy Japanese volunteers (4 men and 11 women; age distribution, 20 to 23 years old). The subjects had no history of smoking, systemic diseases, or ocular diseases other than refractive errors, and were not using any systemic or ocular medications, or supplements. The present study protocol was approved by the Ethics Committee of the Sapporo Medical University School of Medicine and was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all subjects before their enrollment.
Study protocol
As shown in Fig. 1, immediately after the measurements of systemic blood pressure (SBP), heart rates (HRs), IOPs, ocular perfusion pressures (OPPs), and ONH blood circulations by laser speckled flowgraphy (LSFG) at baseline (9 a.m.), each subject received a drop of TM (MSD) to the right eye and a drop of saline to the left eye, which served as the control. At 1.5 and 6 h after the baseline, SBP, HRs, IOPs, OPPs, and LSFG measurements were repeated. This set of study protocol was repeated by using 1% DZ (MSD) or FCTD1% (MSD) instead of 0.5% TM with an interval of 10 days to avoid the influence of each anti-glaucoma drop between sets of the study protocol. Since these physiological and ocular parameters may be affected by intake of fluids or other compounds with pharmacological effects such as caffeine, nicotine, or exercise, subjects did not intake any foods and fluids other than minimum amounts of water, and did not take exercise until the completion of the protocol from 2 h before baseline (total 8 h).
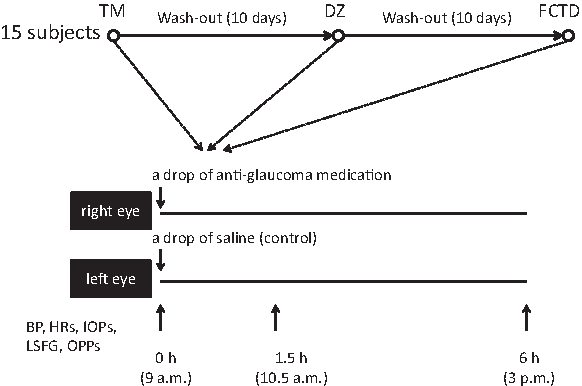
Schema of present study protocol. Overall, 15 healthy subjects received a drop of 0.5% timolol maleate (TM) to the right eye and a drop of saline to the left eye, which served as the control. At baseline (9 a.m.), and 1.5 and 6 h after the baseline, systemic blood pressure (SBP), heart rates (HRs), intraocular pressures (IOPs), ocular perfusion pressures (OPPs), and optic nerve head (ONH) blood circulations by laser speckled flowgraphy (LSFG) were measured. This set of study protocol was repeated by using 1% DZ or FCTD1% instead of 0.5% TM with an interval of 10 days to wash out.
In determining a suitable sample size for the present pilot study, based on a previous study of 2% DZ on ocular blood flow measurement, 11 we estimated that more than 10–13 subjects would be required in order to detect a difference in the effectiveness toward ocular blood hemodynamics by the anti-glaucoma medication.
Measurement of ONH blood circulation
For evaluation of ONH blood circulation, LSFG (LSFG NAVI®; Softcare Co.,) was used. Briefly, the pupil was dilated with 1 drop of 0.5% tropicamide and 0.5% phenylephrine hydrochloride (Mydrin P®; Santen), and the subject remained in a sitting position for at least 30 min. To obtain 3 suitable qualified images, LSFG at ONH was measured more than thrice consecutively using a laser wavelength at 830 nm and a visual angle of 35 degrees. The mean blur rate (MBR), a quantitative index of tissue blood velocity, at 5 points, including the whole ONH, the superior, inferior, nasal, and temporal quadrants of ONH, was calculated by an LSFG Analyzer, a software belonging to the LSFG NAVI apparatus.
Additional analytical methods
The mean blood pressure (MBP) was calculated according to the following formula: MBP=diastolic pressure + 1/3 (systolic pressure–diastolic pressure). IOPs were measured with a Goldmann applanation tonometer. OPPs were calculated according to the following formula: OPP=2/3 [diastolic pressure+1/3 (systolic pressure–diastolic pressure)]–IOP.
Statistical analysis
The MBP and HRs were compared before and after the administration of drops. IOPs, OPPs, and MBR were compared between the right and left eyes at each time point. The Wilcoxon signed-ranks test, Steel's multiple-comparison test, and Mann–Whitney U test were used for statistical analysis. P values less than 0.05 were set as statistically significant.
Results
Effects of 0.5% TM, 1% DZ, and FCTD1% on IOPs, OPPs, and MBP
In comparison with the baseline and their controls, IOPs were significantly decreased in 0.5% TM (P<0.01) and FCTD1% (P<0.05) at 1.5 and 6 h, respectively, after the administration of drops. A drop of 1% DZ did not significantly reduce IOP (Table 1).
Values represent mean±the standard deviation.
Mann–Whitney U test, aP<0.01, bP<0.05.
IOPs, intraocular pressures; TM, timolol maleate; DZ, dorzolamide hydrochloride.
OPPs (Table 2) and MBPs (Table 3) were not changed by the administration of 0.5% TM, 1% DZ, or FCTD1%. In fact, 1% DZ and FCTD1% had no effects on HRs, while 0.5% TM caused a significant and transient decrease in HRs at 1.5 h after the administration (P<0.01), but these effects dissipated by 6 h after administration (Table 3).
Values represent mean±the standard deviation.
Values represent mean±the standard deviation.
Steel's multiple-comparison test, aP<0.01 versus 0 h.
MBP, mean blood pressure; HRs, heart rates.
Effects of 0.5% TM, 1% DZ, and FCTD1% on ONH blood circulation
As shown in Fig. 2a and b, 0.5%TM or 1% DZ caused no significant effect on ONH blood circulation. However, FCTD1% (Fig. 2c), a mixture of both 0.5% TM and 1% DZ, caused a statistically significant increase in the whole ONH (P<0.05), and the nasal (P<0.05) and inferior quadrants (P<0.01) of ONH from the baseline at 6 h after administration. Therefore, FCTD1% had a synergistic and beneficial effect from 0.5% TM and 1% DZ on the ONH blood circulation.
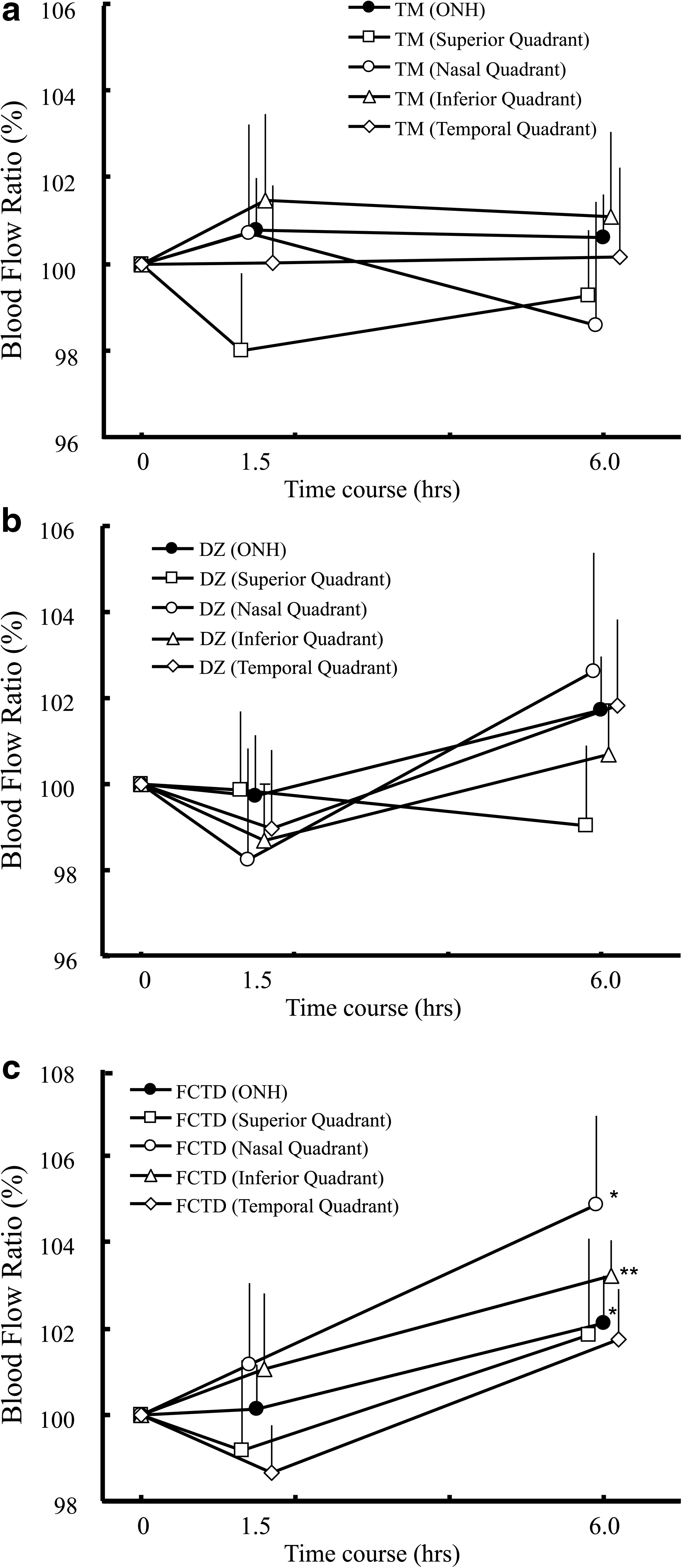
Mean blur rate (MBR) change ratio at ONH before and 1.5 and 6 h after the administration of 0.5% TM
Discussion
Carbonic anhydrase (CA) is a ubiquitous enzyme that catalyzes the reversible hydration of a carbon dioxide reaction (H2O+CO2↔H2CO3↔H++HCO3−), and is recognized as playing a pivotal role in aqueous secretion and pH balance in various organs. 14 To date, 15 isozymes have been identified, 15 of which 3, CA-I, CA-II, and CA-IV, are present in the eye.16,17 An immunohistochemical study has revealed that only CA-II is localized within the ciliary epithelium of the human eye. 16 It was reported that acetazolamide did not decrease IOPs in patients with CA-II deficiency. 18 These suggest that CA-II is mainly involved in the regulation of the aqueous production in the human eye. Carbonic anhydrase inhibitors (CAIs) are known to reduce IOPs by reducing aqueous humor secretion caused by the inhibition of CA-II in the ciliary process. 14 Topical administration of DZ (2%), a potent inhibitor of CA-II, has been revealed to decrease IOPs as well as increase ocular blood flow in healthy and glaucoma patients. 11 It was thought that since localization of CA-I, CA-II, and CA-IV is also identified in the retina and choroid,16,17 DZ blocks the conversion of CO2 into bicarbonate, thereby inducing an increase in tissue CO2 concentrations, and in turn, CO2-dependent vasodilation. In fact, it was reported that the CAI-induced increase in cerebral blood flow was closely similar to that of CO2 inhalation. 19
TM, a nonselective β-adrenergic antagonist, is one of the most widely used anti-glaucoma drugs, and it has a powerful and stable hypotensive effect. It is recognized that β-adrenergic receptors work toward systemic vasodilatation, meaning that TM can cause constriction of ocular and systemic vessels, thus affecting the ocular blood supply. At present, there have been many reports on topical TM effects on retinal and ONH circulation in human eyes,20–22 but a consistent concept of TM effects on ocular hemodynamics has not yet been obtained. In the present study, TM showed a significant hypotensive effect, but had no effect on either OPPs or ONH blood circulation.
Several studies have reported that the instillation of a fixed combination of 0.5% TM and 2% DZ (FCTD2%) causes a significant increase in the blood flow at the neuroretinal rim, in addition to its hypotensive effect in the eyes of patients with glaucoma as well as healthy subjects.8–10 Martínez and Sanchez 23 conducted a prospective, 4-year, open-label intervention study and reported that the instillation of 2% DZ in addition to 0.5% TM twice a day showed a significant increase in the retrobulbar hemodynamic parameters in both the ophthalmic and short posterior ciliary arteries, in addition to affecting a significant decrease in IOPs. A controlled, randomized, and double-masked clinical trial reported by Fuchjäger-Mayrl et al., in their initial study using a small numbers of POAG and ocular hypertension patients, demonstrated that an improvement in the retrobulbar hemodynamics parameter was associated with IOP reduction by 2% DZ, but not by 0.5% TM. 8 However, in a follow up to their initial study, when using the same protocol with a larger numbers of patients, they found that both 2% DZ and 0.5% TM caused an improvement in the retrobulbar hemodynamics. 24 Based on these observations, they reached 3 conclusions. First, the impaired ocular blood flow parameter found in POAG and ocular hypertensive patients indicated abnormal autoregulation in the ocular vascular beds. Second, such abnormal autoregulation may be beneficially affected by IOP-lowering therapy by 2% DZ and 0.5% TM. Finally, its mechanism may be different between 2% DZ and 0.5% TM.
Recently, we have reported that instillation of a lower concentration of DZ (1%) in patients with glaucoma caused an increase in blood flow in the ONH as well as a decrease in IOPs. 13 Furthermore, we have also reported that 1% DZ thrice a day in addition to 0.5% TM twice a day for 8 weeks significantly increases blood flow levels at the infero-temporal neuroretinal rim in patients with glaucoma and causes a further decrease in IOPs. 25 Thus, 1% DZ consistently caused a beneficial effect on ocular hemodynamics in addition to the hypotensive effect in patients with glaucoma. However, in contrast, we found that a fixed combination of 0.5% TM and 1% DZ (FCTD1%) showed a significant increase in ONH blood circulation in eyes from healthy subjects, while this effect was not observed in the medication of 0.5% TM or 1% DZ. Thus, 1% DZ did not have a significant effect on the ONH blood flow in normal subjects. Consistent with the current result, it was reported that an instillation of 1% DZ did not change the ONH blood flow in healthy subjects, 12 although 2% DZ caused an increase in the ocular hemodynamics of both healthy and glaucoma patients. 11 Since the ONH blood flow may already be decreased in patients with glaucoma, but not in healthy subjects, we speculated that CA inhibitory effects by a lower concentration of DZ (1%) may be more evident in eyes from patients with glaucoma than in healthy subjects.
In addition to the IOP-lowering effect of FCTD1% as just mentioned, we found that a statistically significant and transient decrease of HR by 0.5% TM had disappeared by the addition of 1% DZ (Table 3), and a potent increase in effect on ONH blood flow by 1% DZ was evident by the addition of 0.5% TM in healthy subjects (Fig 2). These observations suggested that 0.5% TM and 1% DZ may synergistically have an effect on ocular and systemic conditions. As for ONH blood circulation, we speculated that 0.5% TM may work as a facilitator for the penetration of 1% DZ to the posterior pole and, therefore, its potent effect on ONH blood circulation could be evident. This idea may be supported by the independent effects of DZ and TM on their IOP-lowering dependent vasodilation as just described. In addition, Martínez and Sanchez-Salorio 6 recently reported that the addition of 2% DZ to 0.5% TM in a POAG patient caused a significant decrease in IOP and an improvement in retrobulbar hemodynamics, while the addition of 1% BZ to 0.5% TM showed an IOP reduction that was identical to the case involving the addition of 2% DZ, but had no effects on the retrobulbar hemodynamics. Such differences between DZ and BZ may be ascribed to their different pharmacokinetics toward CA in the eye as well as the synergistic effect of their combinations as just proposed.
A limitation in the present study is its single-centered nature, with a limited number of subjects. Nevertheless, the sample size was estimated before the study. Another limitation of the study is that the evaluation of ocular hemodynamics was measured by only LSFG. Even if the current LSFG facility is good at data reliability and reproducibility, further measurements by other facilities such as color Doppler imaging would add credence to our conclusions. A third limitation is that the present study monitored the short-time effects after a single administration of anti-glaucoma drops. These limitations will need to be addressed as we embark on our next project, which is to investigate the molecular mechanisms that cause the synergistic effect of 0.5%TM and 1%DZ on the ocular blood circulation.