
Abstract
Abstract
Purpose:
To evaluate the analgesic effect of ketorolac 0.5% drops during the intravitreal injection procedure.
Methods:
Thirty patients (n=30) received topical ketorolac 0.5% or vehicle on subsequent intravitreal drug administrations. The procedure followed for the intravitreal injections was the same for all subsequent administrations with the use of tetracaine 0.5% drops as anesthetic. Ketorolac or vehicle was instilled before the injection, and pain perception was recorded on a 0 to 100 Visual Analog Scale (VAS) immediately after the intravitreal administration.
Results:
Mean VAS pain score was 8.16±1.3 when patients received ketorolac and 12.33±1.41 when they received placebo, a difference that was statistically significant (P=0.0003) (paired t-test).
Conclusions:
Topical ketorolac 0.5% reduces patients' pain perception during intravitreal drug administration.
Introduction
The methods of anesthesia for pain alleviation during intravitreal injections that are commonly used include the use of topical anesthetic drops (or gel), the use of topical anesthetic administrated on pledget or cotton tip, and a subconjuctival injection of anesthetic.2–9 Each method has specific advantages and disadvantages, and some studies suggested a similar analgesic effect regardless of the method of anesthesia.2,4,7–9
Nonsteroidal anti-inflammatory (NSAID) eye drops such as ketorolac, diclofenac, and flurbiprofen are widely used in ophthalmology for many conditions, including the reduction of ocular discomfort after refractive surgery. 10 Furthermore, NSAID eye drops alleviate pain in corneal abrasion 11 and painful procedures involving the posterior segment, such as laser photocoagulation 12 or vitreoretinal surgery.13,14 Ketorolac eye drops efficiently control the pain and discomfort associated with cataract surgery, 15 cyclodestructive procedure, 16 and refractive surgery.17.18
To the best of our knowledge, the analgesic effect of NSAID eye drops during the intravitreal injection procedure has never been studied. The purpose of our study is to evaluate the effectiveness of ketorolac 0.5% eye drops on pain alleviation during intravitreal drug administration.
Methods
We evaluated the effectiveness of topical ketorolac eye drops on pain alleviation during the intravitreal injection of drugs. Patients undergoing intravitreal injections of ranibizumab (Lucentis; Novartis Pharma S.A.S., Huningue, France) for the treatment of wet AMD were invited to participate in the study. Exclusion criteria were previous ocular surgery, other than cataract surgery, history of ocular herpetic infection, and concurrent use of systemic NSAIDs. This study was conducted in compliance with the Declaration of Helsinki. The Institutional Review Board's approval was obtained, and all patients provided a signed informed consent.
Thirty patients enrolled to the study. Attempting to control the large variability in pain perception, patients were randomized to receive ketorolac trometamol 0.5% (Acular, Allergan Pharmaceuticals, Westport, Ireland) or vehicle on subsequent injections of ranibizumab. In this way, each patient served as his or her own control. All patients had undergone at least one intravitreal injection of ranibizumab before entering the study. Study medication (ketorolac or vehicle) eye drops were administered in a blinded fashion before the intravitreal injection. One drop of ketorolac or vehicle was instilled 1 h before and a second drop was administered 15 to 10 min before the injection. All intravitreal injections were conducted with the same technique, under aseptic conditions. 1 The injections were administered by the same surgeon in each patient. Tetracaine hydrochloride 0.5% eye drops (Tetracaine Hydrochloride, COOPER S.A., Athens, Greece) were used as anesthetic. One drop of tetracaine was instilled every 5 min for 3 times before the injection, and then, an eyelid speculum was inserted into the conjunctival fornices. Povidone iodine 5% and one more drop of tetracaine hydrochloride were applied on the ocular surface. Intravitreal injections of 0.05 mL ranibizumab were done at the pars plana, at the inferotemporal quadrant, with a 30-gauge needle, 3.5–4 mm posterior to the limbus.
The visual analog scale (VAS) was used as a pain measurement tool. 19 It consisted of a horizontal line, 100 mm in length, anchored by word descriptors at each end (no pain at one end and the worst pain at the other end). Within 15 min from the intravitreal injection, patients were asked to evaluate their pain perception from the intravitreal injection procedure, by the same blinded investigator, using the visual analog scale. Earlier, the VAS had been analytically explained to all patients, and the patients were prompted to mention and evaluate their past pain experiences with the “worst pain” or “no pain,” in order to familiarize with the scale. The patients marked on the line the point that indicated their pain perception. Those who could not clearly visualize the scale were prompted to state a number from 0 to 100. The VAS score (0–100) was determined by measuring from the left-hand end of the line to the point marked by the patient.
Statistical analysis of the VAS pain scores was performed with SPSS (SPSS 17.0 for Windows; SPSS, Inc., Chicago, IL), and paired t-test was used for parametric data. Previous studies identified that a difference of 9 to 13 on the 0 to 100 VAS pain score is required for the pain experience to have clinical significance.20–22 The sample size in this study was calculated as 30 for each intervention, with a 13-point statistically significant difference, a significance level ≤0.05, and a statistical power of 0.8. The standard deviation (SD) was a compromise between similar previous studies and clinical decisions.14,17,18 Regression analysis was performed with pain score as the dependent variable; independent variables included age, sex, and number of injections. Data were expressed as mean±SE, and differences were considered significant at P<0.05.
Results
A total of 30 patients (30 eyes) were recruited in the study, and all patients completed the study. No complications or side effects occurred during the study. The patients' mean age was 73.63±6.94 years (range 67–82). Nine patients (30%) were men, and 83.3% had undergone cataract surgery. The indication for intravitreal injections was exudative AMD.
Pain perception from the intravitreal injection procedure was usually lower when ketorolac was applied. The mean pain score when patients received ketorolac was 8.16±1.3, while when they received vehicle, the pain score was 12.33±1.41, a difference that is statistically significant (P=0.0003, paired t-test). Nine patients (30%) felt the same amount of pain in both treatments, and 3 patients reported less pain with placebo than with ketorolac (Figs. 1, 2).
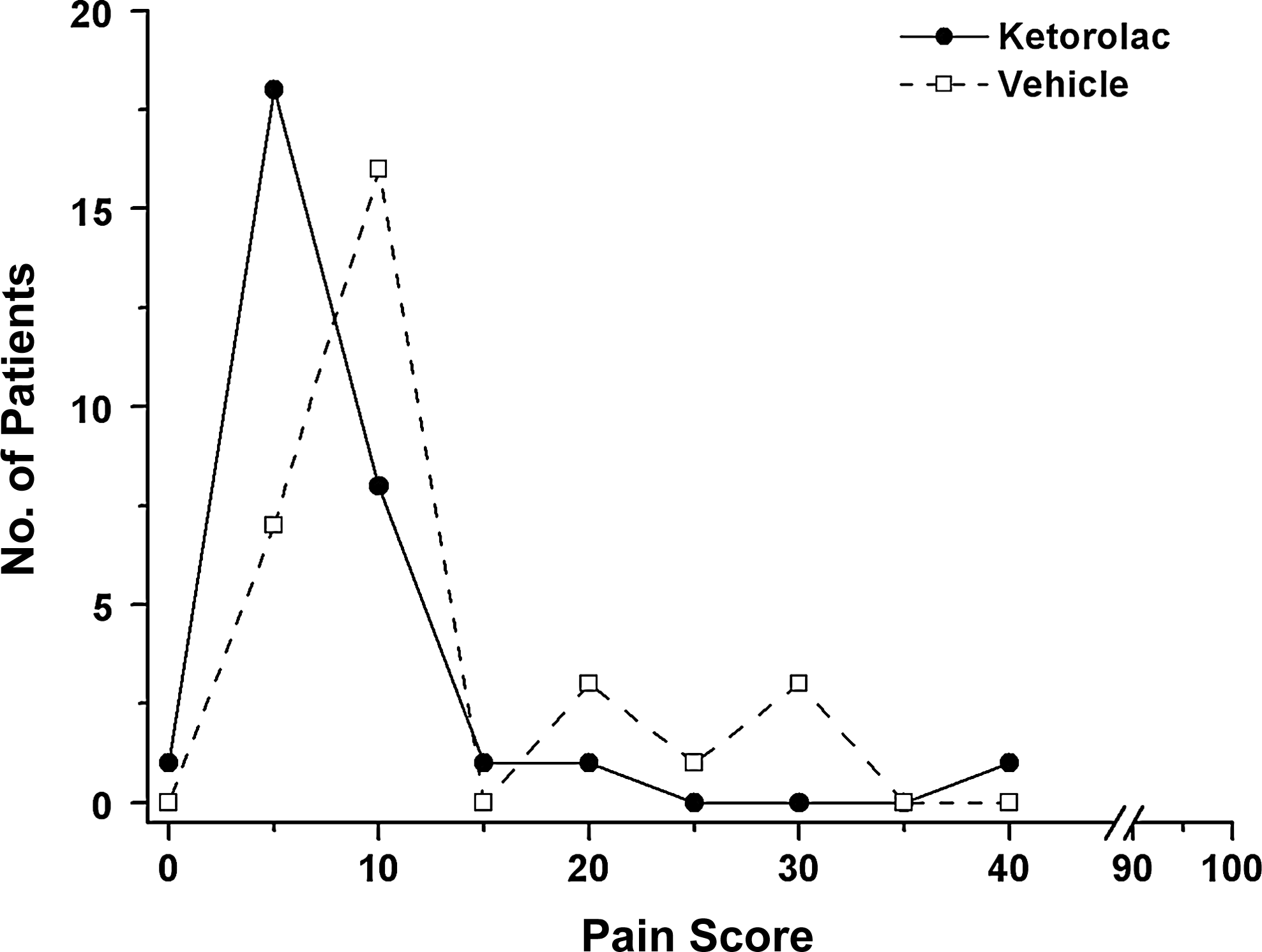
Distribution of pain scores in patients who received either ketorolac 0.5% or vehicle for pain alleviation before intravitreal drug administration.

Visual analog scale pain scores (mean±SE) for ketorolac- and vehicle-instilled eyes. *P=0.0003.
Many factors can influence the perception of pain, including sex.5,20 In our study, the mean VAS pain score was 11.15±2.12 in men when placebo was instilled and 7.3±1.34 when ketorolac was administered, and the difference was statistically significant (P=0.0024). In women, the mean VAS pain score was 13.23±1.91 when placebo was instilled and 8.82±2.07 when ketorolac was used, and the difference was also statistically significant (P=0.0169), (Fig. 3).
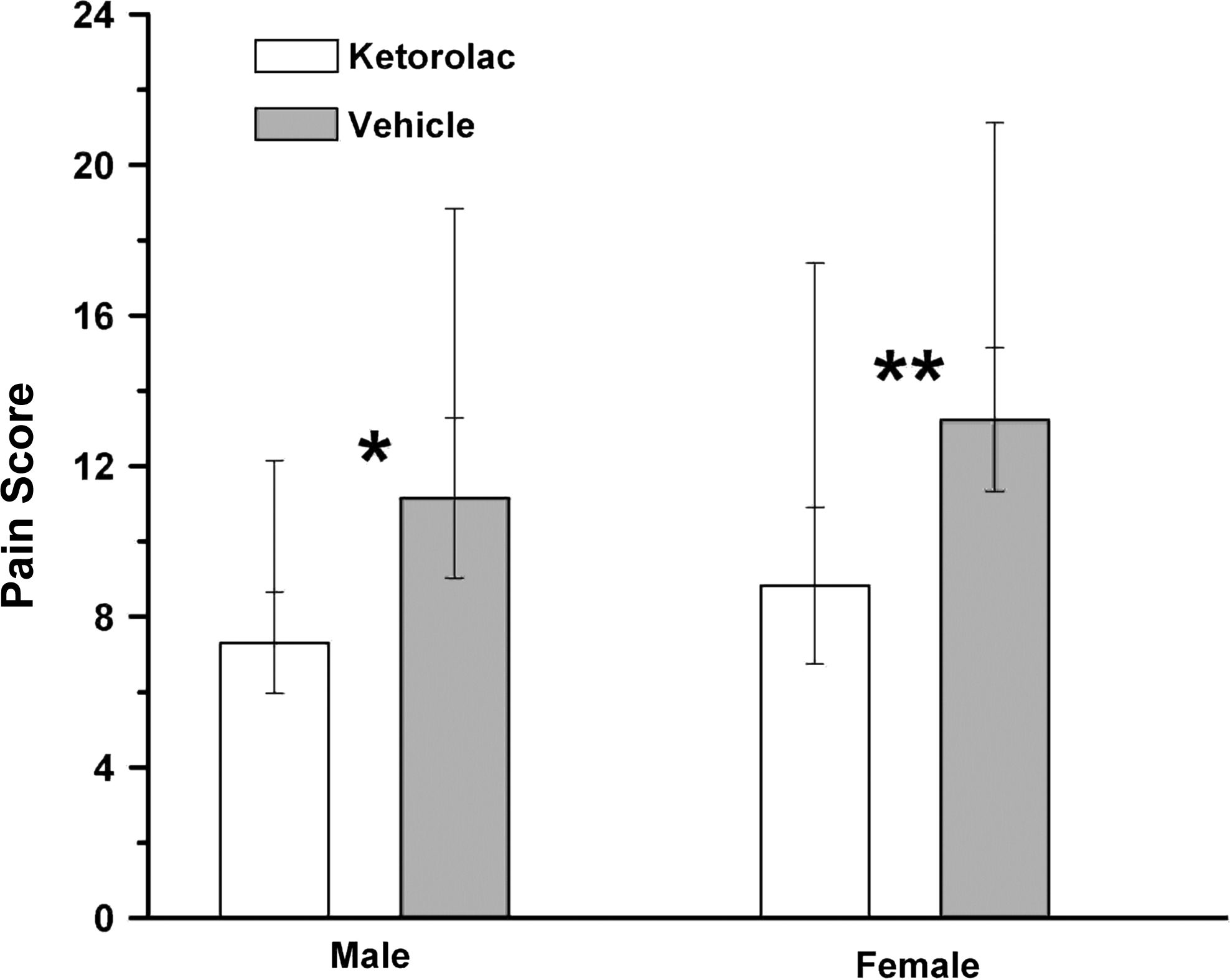
Visual analog scale pain scores (mean±SE) for ketorolac- and vehicle-instilled eyes in gender subgroups (men and women). *P=0.0024 **P=0.0169
There was no relationship between VAS score and age, gender, and number of intravitreal injections in ketorolac- and vehicle-instilled eyes (P=0.528 and 0.772 respectively).
Discussion
Treatment of the posterior segment diseases of the eye requires drug delivery systems that are able to overcome the protective barriers and lead to therapeutic drug concentrations. Intravitreal injections are used for a wide variety of therapeutic agents such as antibiotics, antifungal agents, antivirals, corticosteroids, antineoplasmatic, and anti-VEGF agents as a mainstay for the treatment of various diseases such as endophthalmitis, viral retinitis, posterior uveitis, diabetic retinopathy, cystoid macular edema, AMD, and retinal vascular occlusions.23,24 The intravitreal injections (especially with the use of anti-VEGF agents) have become a common route for drug delivery.
The use of topical anesthetic drops before the intravitreal injection provides convenient, safe, and rapid onset of anesthesia. However, it is reported that the use of these agents does not provide complete anesthesia of the conjunctiva and the sclera with a single application. 25 Although the use of subconjuctival anesthesia provides adequate pain control during the procedure, its application is more painful and leads to adverse effects such as subconjuctival hemorrhage. 9 Furthermore, the use of topical anesthetic gel (lidocaine) provides sufficient pain control but is often an inconvenient procedure, because it needs a few minutes to provide adequate anesthesia, has to be removed before the intravitreal injection, and may theoretically interfere with the antiseptic action of povidone iodine, increasing the risk of endophthalmitis.2,4,25 Moreover, some studies concluded that these different anesthetic techniques have a similar analgesic effect during the procedure of the intravitreal injection.2,4,7–9
Topically applied NSAIDS are used to alleviate pain in many painful surgical conditions of the anterior and the posterior segment of the eye. The mechanism of the analgesic effect of NSAIDs is believed to be the inhibition of the arachidonic acid cascade, while even weak inhibitors of prostaglandin synthesis exhibit strong analgesic action. 26 More specifically, NSAIDs target cyclooxygenase, the enzyme that facilitates the formation of endoperoxides from arachidonic acid by participating in the cascade of reactions which ultimately generate prostaglandins (cyclo-oxygenase pathway). Prostaglandins can produce miosis, increase permeability of the blood-ocular barriers, conjunctival hyperemia, and changes in intraocular pressure. Furthermore, prostaglandins have chemokinetic activity, serve as mediators of inflammatory responses, and are associated with the pain response and allergic reactions. 10 By inhibiting prostaglandin biosynthesis, NSAIDs exhibit potent analgesic, anti-inflammatory, and antipyretic effects. NSAIDs can reduce not only the pain induced by a noxious stimulus that acts for a long time (corneal trauma) but also the pain induced by a single stimulus (acute pain that results from sudden trauma). 26
Ketorolac, which belongs to the phenylalkanoic acids class, is a topically effective NSAID and was studied for pain alleviation during anterior segment procedures. Walters et al. reported that when one drop of ketorolac 0.4% was topically applied, its aqueous humor concentration peaked at 60 min and slowly decreased throughout the remaining 3 h. 27 Ling et al. reported that after the topical administration of ketorolac 0.5% in rabbits, peak concentrations were achieved in the ocular tissues and in plasma within 1 h post instillation. In addition, concentrations were highest in the cornea and sclera. 28 In our study, we used one drop of ketorolac 0.5% 60 min before the intravitreal injection and a second drop 15 to 10 min before the procedure in order to ensure that the maximum potential analgesic effect by the medication will be achieved. It is unknown what effect would have a longer or shorter waiting time or a dosing starting a day before the injection.
The experience of pain is very variable between the patients who have undergone intravitreal injections. Many factors can influence the perception of pain, including patient's sex, age, past experience, culture, and anxiety levels, and anticipate benefits from the procedure (vision improvement). 5 In order to eliminate the possible influence of anxiety on patients receiving their first injection, all the patients enrolled in the study had undergone at least one intravitreal injection of the same agent at the past. In addition, for the same reason, each patient received the subsequent intravitreal injections from the same investigator.
During the study, no side effects were noticed. The major finding of this study was that a topical application of ketorolac 0.5% reduced pain perception from the intravitreal injection procedure. We evaluated the combined level of pain from the whole procedure (anesthesia and injection), because the instillation of ketorolac does not cause significant local symptoms. 10
In our study, the difference between mean VAS pain scores of ketorolac and vehicle was 4.17. A difference of 9 to 13 on the 0 to 100 VAS scale between pain scores is required for the pain experience to have clinical significance, as identified from previous studies.20–22 This might indicate that the difference between VAS pain scores between ketorolac and placebo is not clinically significant. However, the difference of 9 to 13 in pain scores has been identified by studies that referred to an emergency room setting and should be interpreted with caution.
Delayed pain and discomfort after the intravitreal injection can not only be caused by the irritation of the cornea, but also be caused by the intravitreal injection procedure itself (tissue trauma). One interesting observation was that most patients who received ketorolac reported (over telephone assessment) less discomfort the next few hours after the procedure (data are not shown). Since the study was not designed to investigate this parameter, the outcome just mentioned should be approached with caution. However, it is an interesting observation that the use of ketorolac can also alleviate late pain and discomfort after the intravitreal injection.
To our knowledge, this is the first study that evaluates the analgesic effect of topically applied NSAIDs during the intravitreal injection procedure. Limitations of our study arise from the very nature of pain; its variability and difficulty in direct measurement. We tried to overcome these issues by randomizing patients to receive ketorolac drops or vehicle on subsequent injections in a blinded fashion. Moreover, all patients had undergone at least one intravitreal injection in the past and received the subsequent intravitreal injection from the same investigator to avoid any bias from factors affecting pain perception. Furthermore, the VAS was analytically explained to all patients, and the evaluation of the pain perception scales was performed by the same blinded investigator.
In conclusion, this study demonstrates that topically applied ketorolac 0.5% may alleviate the pain induced by the intravitreal injection. Larger studies are needed to elucidate the role of NSAIDs as analgesics during the procedure of intravitreal injections.
Footnotes
Author Disclosure Statement
No competing financial interests exist for any of the authors.