
Abstract
Abstract
Purpose:
The goal of this study was to develop and characterize indomethacin-loaded solid lipid nanoparticles (IN-SLNs; 0.1% w/v) for ocular delivery.
Methods:
Various lipids, homogenization pressures/cycles, Tween 80 fraction in the mixture of surfactants (Poloxamer 188 and Tween 80; total surfactant concentration at 1% w/v), and pH were investigated in the preparation of the IN-SLNs. Compritol® 888 ATO was selected as the lipid phase for the IN-SLNs, as indomethacin exhibited a highest distribution coefficient and solubility in this phase.
Results:
Homogenization at 15,000 psi for 6 cycles resulted in the smallest particle size. Increase in the Poloxamer 188 fraction resulted in decrease in the entrapment efficiency (EE). The mean particle size, polydispersity index, zeta-potential, and EE of the optimized formulation were 140 nm, 0.16, −21 mV, and 72.0%, respectively. IN-SLNs were physically stable post-sterilization and on storage for a period of 1 month (last timepoint tested). A dramatic increase in the chemical stability and in vitro corneal permeability of indomethacin was observed with the IN-SLN formulation in comparison to the indomethacin solution- (0.1% w/v) and indomethacin hydroxypropyl-beta-cyclodextrin-based formulations (0.1% w/v).
Conclusion:
Results from this study suggest that topical IN-SLNs could significantly improve ocular bioavailability of indomethacin.
Introduction
In the past, a number of strategies attempting to improve the ocular bioavailability and to reduce the side effects of indomethacin have been investigated. These include the use of nanocapsules, surfactants, oils, polymeric nanoparticles, and emulsions.3,4,6–8 However, the use of oils is limited due to their irritation potential, difficulty in sterilization, and their influence on intraocular pressure.9,10 On the other hand, the potential of emulsions for topical delivery of indomethacin is limited by its physical instability, which can lead to agglomeration, drug expulsion, and eventual cracking of the emulsions. 11 In ophthalmology, topical polymeric nanoparticles, primarily developed for intravenous administration, have demonstrated promising results over the last 10 years. These systems protect the drug against chemical and enzymatic degradation, improve tolerance, reduce systemic side effects, and increase corneal uptake and intraocular half-lives. However, issues such as cytotoxicity of polymers before or after internalization into the cells, lack of suitable large-scale production method, and generation of toxic degradation products hindered progress in the development of polymeric nanoparticles. 12
In recent years, solid lipid nanoparticles (SLNs) have attracted a lot of attention for the delivery of water-insoluble drugs. SLNs were especially developed to deliver lipophilic drugs, combining the advantages of the traditional colloidal systems (emulsions, liposomes, and polymeric micro- and nanoparticles) while avoiding some of their major disadvantages. 11 These particulates are in the submicron-size range and are made up of biocompatible and biodegradable materials. All the excipients used in their manufacture have an approved Generally Regarded as Safe status and are free from the risk of acute or chronic toxicity.13–15 A striking advantage of these particles is that large-scale production can be undertaken in a cost-effective and relatively simple manner using a high-pressure homogenizer.13–15 The use of a solid lipid matrix also provides greater flexibility with respect to modifying drug release and improving drug stability by protecting from chemical degradation. SLN colloidal dispersions can be administered as eyedrops. Such formulations would neither lead to blurred vision nor pose any ocular discomfort issues due to their small particulate size. 16 Moreover, the small size and mucoadhesive characteristics 15 of SLNs could lead to enhanced ocular bioavailability by increasing their residence time in the cul-de-sac and promoting uptake into corneal or conjunctival tissues through endocytotic mechanisms. 17
Therefore, the objective of the present investigation was to develop and characterize indomethacin-loaded SLNs (IN-SLNs; 0.1% w/v) for ocular delivery. Another objective of this project was to compare in vitro drug permeation across the isolated rabbit cornea from IN-SLN formulations with that from indomethacin solution (IN-SOL; 0.1% w/v) and indomethacin hydroxypropyl-β-cyclodextrin- (IN-HPβCD; 0.1% w/v) based formulations.
Methods
Materials
Compritol® 888 ATO (glyceryl behenate) and Precirol® ATO 5 (glyceryl palmitostearate) were obtained as gift samples from Gattefossé (Paramus, NJ). Dynasan® 118 (glyceryl tristearate), Dynasan® 114 (glyceryl trimyristate), and Softisan® 154 (hydrogenated palm oil) were kindly supplied by Salsol Germany GmbH (Anckelmannsplatz, Hamburg, Germany). HPβCD (average molecular weight: 1,380, degree of substitution 0.6) was procured from Sigma Chemical Co. Amicon® Ultracentrifugal filter devices with regenerated cellulose membrane (molecular weight cut off 100 kDa), Poloxamer 188, Tween 80, indomethacin, high performance liquid chromatography (HPLC)- grade solvents, and other chemicals (analytical grade) were obtained from Fisher Scientific. Whole eyes from male albino New Zealand rabbits were obtained from Pel-Freez Biologicals. Eyes were shipped overnight in solution (Hanks' balanced salt solutions) over wet ice and were used immediately on receipt.
Saturation solubility studies
Saturation solubility studies as a function of pH were carried out following the standard shake-flask method. An excess amount of indomethacin was added to screw-capped glass vials containing various buffers. To achieve uniform mixing, samples were constantly agitated at 100 rpm for 24 h at 25°C in a reciprocating water bath (Fisher Scientific). At the end of 24 h, the samples were centrifuged (AccuSpin 17R; Fisher Scientific), and the supernatant was analyzed for drug content. Solubility studies were carried out in buffers: phosphate (pH 1.2, 3.0, 6.8, and 7.4) and acetate (pH 5.0) with a buffer strength and ionic strength of 15 mM and 0.03, respectively.
Formulations
IN-SOL formulation
IN-SOL (100 mL) was prepared by mixing indomethacin (0.1% w/v) with Tween 80 (1% w/v) and propylene glycol (29.3% w/v). To this mixture, 1 N sodium hydroxide (NaOH) (prepared in bidistilled and 0.2-μM filtered water) was added in small increments under continuous mixing and stirring to dissolve the drug. NaOH was added until the pH reached 6.8. Finally, the phosphate buffer (pH 6.8) was added to bring the final volume to 100 mL. This composition is based on previously published reports.18,19
Indomethacin-loaded solid lipid nanoparticles
Selection of lipid
Distribution behavior of indomethacin between lipids and phosphate buffer
The distribution behavior of indomethacin between lipids {Compritol 888 ATO [melting point (MP): 70°C–72°C], Precirol ATO 5 (MP: 56°C), Dynasan® 116 (MP: 61°C–65°C), Dynasan 118 (MP: 70°C–73°C), and Softisan 154 (MP: 53°C–55°C)} and phosphate buffer (15 mM, pH 6.8) was determined as described previously.
20
Briefly, indomethacin (5 mg) was dispersed in a mixture of melted lipids (500 mg) and 2 mL of, pH 6.8, hot phosphate buffer. The temperature of the phosphate buffer and the lipids was 10°C above the MP of lipids under investigation. The mixture was constantly agitated at 100 rpm for 30 min (at 10°C above the MP of lipids) in a reciprocating water bath. At the end of 30 min, the mixture was cooled and centrifuged (13,000 rpm for 20 min) (AccuSpin 17R; Fisher Scientific), and the aqueous phase was analyzed for drug content. All experiments were carried out in triplicates. The distribution coefficient (DpH 6.8) of indomethacin was determined using Equation (1):
where AIND is the amount of indomethacin added (5 mg), and AINDA is the amount of indomethacin determined in the aqueous phase.
Solubility of indomethacin in different lipids
Indomethacin (100 mg) was added to 2 or 5 g of Compritol 888 ATO, Precirol ATO 5, Dynasan 116, Dynasan 118, or Softisan 154, and the samples were incubated at 10°C above the MPs of lipid for 15 min. The samples showing good solubility were allowed to cool at room temperature for 24 h and were observed for the presence of crystals using light microscopy.
Preparation of IN-SLNs
IN-SLNs were prepared using a hot homogenization method as previously described.15,21 Accurately weighed Compritol 888 ATO was melted, and indomethacin (5% w/w with respect to the lipid) was dissolved therein to obtain a clear lipid phase. Simultaneously, an aqueous phase, containing surfactants (Poloxamer 188 and/or Tween 80) and glycerin (2.25% w/v) in bidistilled water, was heated. The hot aqueous phase was then added to the melted lipid phase under stirring (magnetic stirrer) to form a premix (600 rpm, 1–2 min). The premix was then subjected to emulsification at 16,000 rpm for 6 min using T 25 digital Ultra-Turrax (IKA® Works, Inc.) to form a hot pre-emulsion. The pre-emulsion obtained, after adjusting to the required volume, was subjected to high-pressure homogenization using thermostated Emulsiflex C5 (Avestin) resulting in the formation of hot emulsion dispersion. The temperature during the entire process was maintained at 80°C±2°C. The obtained hot emulsion was slowly cooled to room temperature to form IN-SLNs. The pH of the resulting formulation was adjusted using NaOH or hydrochloric acid (HCL; 1 N). The final concentrations of Compritol 888 ATO and indomethacin in the formulation were kept constant at 2% w/v and 0.1% w/v, respectively.
In the present study, the threshold parameters for the preparation of the IN-SLN dispersion were selected by studying the effect of homogenization pressure, number of homogenization cycles, fraction of Tween 80 in the mixture of surfactants (Poloxamer 188 and Tween 80) at constant total surfactant concentration (1% w/v), and pH on mean particle size, polydispersity index (PI), and entrapment efficiency (EE). Efforts were directed toward minimizing the particle size, maximizing the EE, and maximizing the zeta-potential.
Indomethacin hydroxypropyl-β-cyclodextrin (IN-HPβCD) formulation
For the preparation of the IN-HPβCD formulation, indomethacin (0.1% w/v) was dissolved in the 2.5% w/v HPβCD solution prepared in phosphate-buffered saline (pH 6.8). The final pH of the IN-HPβCD solution was selected as 6.8, because Indocollyre is available commercially at this pH.
Particle size and zeta-potential measurement
The mean particle size and the PI of the SLN dispersion were determined by photon correlation spectroscopy using Zetasizer Nano ZS Zen3600 (Malvern Instruments, Inc.) at 25°C and 173° backscatter detection in disposable folded capillary clear cells. The measurements were obtained using an helium-neon laser of 633 nm, and the particle size analysis data were evaluated using volume distribution. Zeta-potential measurements were carried out at 25°C in folded capillary cells using the same instrument. The zeta-potential values were obtained from the electrophoretic mobility using the Smoluchowski equation. For measurement of particle size distribution and zeta-potential, SLN samples were diluted (1:500) with water and 10 mM 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid buffer (pH 6.8), respectively. Bidistilled and 0.2-μM filtered waters were used for these measurements. All measurements were performed in triplicates.
Assay and EE
The lipid in the IN-SLN dispersion was precipitated using 190-proof alcohol, and the drug content in the supernatant after centrifugation (13,000 rpm for 20 min), as such or after further dilution with 190-proof alcohol, was measured using an HPLC system. Indomethacin content in IN-SOL and IN-HPβCD was also determined after dilution with 190-proof alcohol.
The percentage of indomethacin entrapped in the SLNs (% EE) was determined by measuring the concentration of free drug in the aqueous phase of an undiluted IN-SLN dispersion. The EE was evaluated by an ultrafiltration technique with a 100-kDa centrifugal filter device composed of a regenerated cellulose membrane (Amicon Ultra). An aliquot (500 μL) of undiluted IN-SLN was added to the sample reservoir and centrifuged at 5,000 rpm for 10 min. The obtained filtrate was further diluted with alcohol (190 proof) and analyzed for drug content using HPLC. The EE was estimated using Equation (2):
where Wi=total drug content, and Wf=amount of free drug in aqueous phase.
Osmolality and pH measurement
Osmolality was measured by the freezing-point depression method using Osmette S, model 4002 (Precision Systems, Inc.). After calibration of the osmometer with reference standards (100 and 500 mOsm/kg H2O), the osmolality was measured (2-mL sample vials were used). The pH was measured using a calibrated Mettler Toledo Seven Easy pH meter (Fisher Scientific).
Sterilization and stability of the formulations
Three batches of optimized IN-SLNs were evaluated for physical and chemical stability after autoclaving (110°C for 30 min) and on storage (40°C, 25°C, and 4°C). The stability parameters evaluated were particle size, PI, zeta-potential, EE, pH, and drug content. Initial values for the parameters mentioned above were determined 24 h post-preparation and post-sterilization. IN-SLNs were subjected to moist-heat sterilization at 110°C for 30 min using a Tuttnauer Brinkmann 3545 EP autoclave (Fisher Scientific). The samples were then subjected to stability studies at 40°C, 25°C, and 4°C for a period of 1 month (last point tested). Additionally, the drug content in the IN-HPβCD and IN-SOL formulation was also monitored post-sterilization (110°C for 30 min) and on storage (40°C, 25°C, and 4°C).
Differential scanning calorimetry analysis
The differential scanning calorimetry (DSC) analysis was carried out using a Diamond Differential Scanning Calorimeter (Perkin-Elmer Life and Analytical Sciences). The samples were weighed and hermetically sealed in aluminum pans and were heated from 20°C to 200°C at a heating rate of 10°C/min under nitrogen purge (20 mL/min). An empty aluminum pan was used as the reference.
The DSC analysis was carried out on the following samples: (1) indomethacin (∼0.5 mg), (2) bulk Compritol 888 ATO, (3) lyophilized IN-SLN formulation, (4) lyophilized blank SLNs, and (5) physical mixture (indomethacin and Compritol 888 ATO). Additionally, hyper-DSC studies (20°C–200°C at a heating rate of 200°C/min) on lyophilized IN-SLNs and physical mixture (indomethacin and Compritol 888 ATO) were also performed. Approximately 10 mg of Compritol 888 ATO, lyophilized IN-SNLs, and blank SLNs was used for the DSC analysis. The physical mixture consisted of ∼0.5 mg indomethacin and ∼9.5 mg of Compritol 888 ATO. The ratios of drug and lipids, used in these set of studies, were similar to the weight ratios in IN-SLNs.
In vitro corneal permeation studies
The corneas excised from whole eyes, obtained from Pel-Freez Biologicals, were used for the determination of in vitro transcorneal permeability. Whole eyes were shipped overnight in Hanks' balanced salt solution, over wet ice, and were used immediately upon receipt. The corneas were excised with some scleral portion adhering to help secure the membrane between the diffusion half-cells during the course of a transport study. After excision, the corneas were washed with the ice-cold Dulbecco's phosphate buffer saline (DPBS; pH 7.4) and mounted on side-by-side diffusion half-cells (PermeGear, Inc.) with the epithelial side facing the donor chamber. The temperature of the half-cells was maintained at 34°C with the help of a circulating water bath.
Two milliliters of the optimized IN-SLNs (pre- and poststerilization), or IN-SOL or, IN-HPβCD was diluted with 1 mL of 3 mM acyclovir (ACV) solution (in DPBS pH 7.4) and immediately added to the donor chamber after adjusting the pH to 6.8. The indomethacin content in all the formulations was 0.1% w/v. The receiver chamber medium consisted of 3.2 mL of HPβCD (2.5% w/v) in the DPBS (pH 7.4) solution for all the transport studies. A slight difference in the donor and receiver chamber volumes helped maintain the normal shape of the cornea through marginally elevated hydrostatic pressure. The contents of both chambers were stirred continuously with a magnetic stirrer. Aliquots (400 μL) were withdrawn from the receiver chamber at predetermined time points (30, 60, 90, 120, 150, and 180 min), and replaced with an equal volume of the 2.5% w/v HPβCD in DPBS (pH 7.4). Samples were stored at −80°C until further analysis of indomethacin and ACV content. ACV is known to cross the corneal epithelium by passive paracellular diffusion and was thus added to monitor the integrity of the corneal epithelium in the presence of the formulation components. Transcorneal permeation of ACV alone (control) was also evaluated as described above, except that in this study, the donor solution consisted of 1 mL of ACV (3 mM in DPBS, pH 7.4) diluted with 2 mL of DPBS (pH 6.8). Additionally, transcorneal permeation of indomethacin from the IN-HPβCD formulation was also monitored in the presence of surfactants (0.75% w/v Tween 80 and 0.25% w/v Poloxamer 188). ACV content in the donor chamber was analyzed using an ultrafiltration technique (Amicon Ultra-100-kDa centrifugal filter device). An aliquot (200 μL) of ACV containing the IN-SLN dispersion sample was added to the sample reservoir and centrifuged at 5,000 rpm for 10 min. The obtained filtrate was further diluted with water and analyzed for ACV content using HPLC.
To evaluate the effect of the addition of ACV on the physiochemical properties of the IN-SLNs during the transport experiment, additional experiments were undertaken. In these experiments, 1 mL of 3 mM ACV solution (in DPBS, pH 7.4) was added to 2 mL of the formulation, and at the end of 3-h osmolality, zeta-potential, particle size, and EE of IN-SLNs were determined.
Histology studies
At the end of the in vitro permeation experiments with the IN-SLNs, as described in the section In vitro corneal permeation studies, the corneas were collected from the side-by-side diffusion cells. The corneas exposed to PBS, under similar experimental conditions, were used as a control. The corneas were fixed in a solution containing 2% v/v paraformaldehyde and 2% v/v glutaraldehyde in PBS (pH 7.4). The rabbit corneas were sectioned and stained with hematoxylin and eosin by Excalibur Pathology, Inc. After fixing, the corneas were processed and embedded in paraffin. Five-micron cross-sections were cut using a microtome (American Optical 820). The sections were then deparaffinized with xylene and rehydrated gradually with decreasing concentrations of alcohol and washed in running water. The sections were then stained with Gill III hematoxylin (StatLab Medical) for 10 min, washed in running water, dipped 3 times in acid alcohol, washed in running water, blued in 1% ammonia water for 1 min, and washed in running water. The sections were then rinsed in 95% alcohol, stained with Treosin (StatLab Medical) for 15 s, followed by 3 washings in 100% alcohol and 3 washings in xylene. Finally, the sections were cover-slipped and examined under a microscope (Chromavision ACIS II).
Data analysis
The rate of indomethacin and ACV transport across the excised rabbit cornea was obtained from the slope of a cumulative amount of indomethacin or ACV transported versus time plot. The steady-state flux (SSF) was determined by dividing the rate of transport by the surface area as described in Equation (3):
where, M is the cumulative amount of drug transported, and A is the corneal surface area exposed to the permeant.
The corneal membrane permeability was determined by normalizing the SSF to the donor concentration, Cd, according to Equation (4):
Analytical method
Samples were analyzed for indomethacin and ACV content using an HPLC system comprised of Waters 717 plus autosampler, Waters 2487 Dual λ Absorbance detector, Waters 600 controller pump, and Agilent 3395 integrator. A Symmetry® C18 4.6 mm×250 mm column was used for both compounds. The mobile phase for ACV consisted of 20 mM phosphate buffer (pH 2.5) and acetonitrile (98:2), and for indomethacin, the mobile phase used was methanol, water, and orthophosphoric acid (70:29.05:0.05). The λmax for indomethacin and ACV was 270 and 254 nm, respectively. The flow rate was set at 1 mL/min for both compounds.
Results
Saturation solubility studies
Saturation solubility of indomethacin as a function of pH was studied at 25°C for 24 h in a reciprocating water bath. The solubility of indomethacin was observed to be highly dependent on the solution pH. The solubility of the drug in an acid pH (pH 1.2, 3.0, and 5.0) was observed to be significantly lower than that in the neutral buffers (pH 6.8 and 7.4). The aqueous solubility of indomethacin at pH 7.4, 6.8, 5.0, 3.0, and 1.2 was 732.0±20.0, 340.0±10.0, 10.0±0.06, 1.5±0.05, and 0.3±0.03 μg/mL, respectively.
Indomethacin-loaded solid lipid nanoparticles
Selection of lipid
The distribution coefficient (DpH 6.8) of indomethacin in various lipids is illustrated in Fig. 1. The distribution behavior of indomethacin between lipid and phosphate buffer (pH 6.8) was determined by measuring the free-drug concentration in the aqueous phase. The DpH 6.8 value was calculated using Equation (1). The DpH 6.8 values of indomethacin in Compritol 888 ATO, Precirol ATO 5, Dynasan 114, Softisan 154, and Dynasan 118 were 10.1±0.8, 5.1±0.7, 2.7±0.5, 2.7±0.3, and 2.5±0.3, respectively. The solubility of indomethacin (100 mg) in 2 and 5 g of lipids was evaluated by incubating the drug with the lipid, at a temperature 10°C above the MPs of lipid, for 15 min. Indomethacin remained undissolved, and the drug crystals were observed in 2 g of Precirol ATO 5, Dynasan 114, Softisan 154, and Dynasan 118. Indomethacin was soluble in 5 g of Precirol ATO 5, Dynasan 114, Softisan 154, and Dynasan 118; however, the drug crystals were observed in these lipids after 24 h under light microscopy. Indomethacin exhibited a good solubility (clear yellow lipid melt) in 2 or 5 g of Compritol 888 ATO, and the drug crystals were not observed on cooling to room temperature and after 24 h under light microscopy.
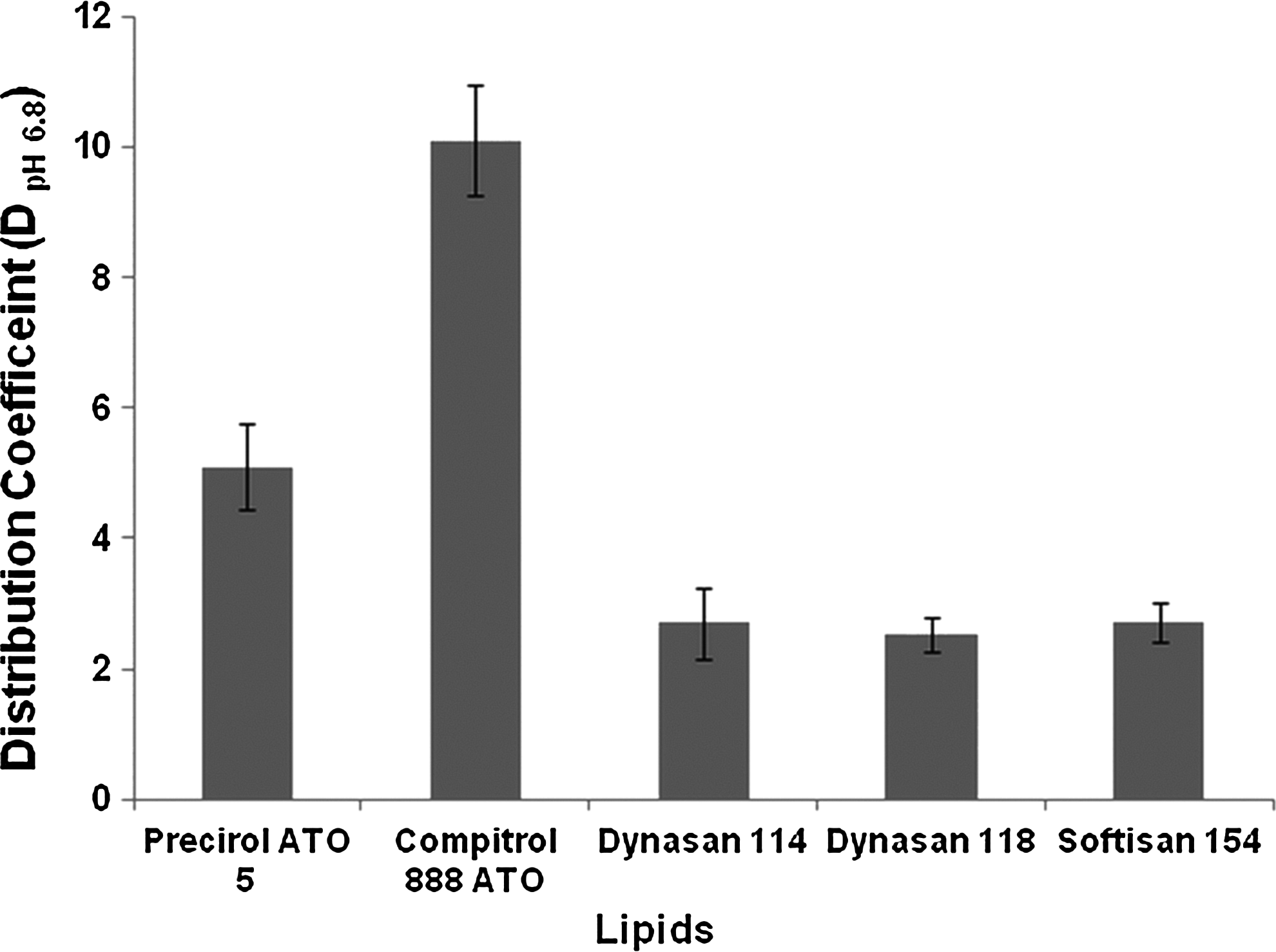
Distribution coefficient (DpH 6.8) of indomethacin in various lipids. Results are depicted as mean±SD (n=3).
Effect of homogenization pressure and the number of homogenization cycles
IN-SLNs were prepared using the hot homogenization method. For selection of the optimum homogenization pressure, the pre-emulsion was passed through the high-pressure homogenizer at 3 different homogenization pressures (7,500, 15,000, and 20,000 psi) for 5 cycles. The mean particle size of the IN-SLNs at 7,500, 15,000, and 20,000 psi was 300±10, 180±4, and 178±10 nm, respectively. Figure 2 illustrates the effect of homogenization cycles, at 15,000 psi, on the mean droplet size and PI of IN-SLNs. As the number of homogenization cycles increased from 1 to 6, there was a decrease in the particle size from 769±208 to 140±5 nm, and a decrease in PI from 0.38±0.05 to 0.16±0.01 was observed. Further increase in the number of homogenization cycles did not result in a significant decrease in either the particle size or the PI of IN-SLNs.
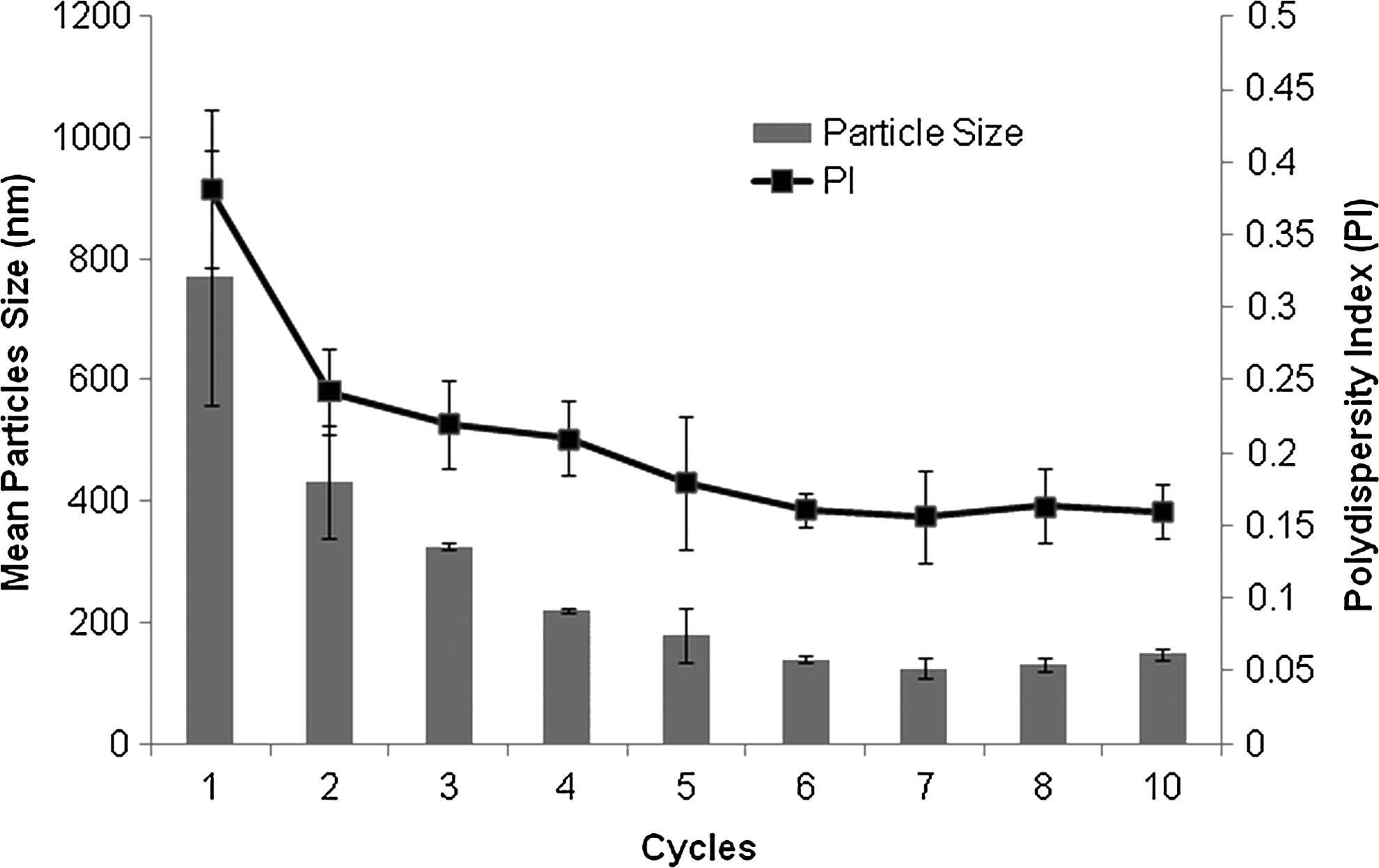
Effect of homogenization cycles on the mean particle size (nm) and polydispersity index (PI). Results are depicted as mean±SD (n=3).
The formulation used for the preparation of the pre-emulsion consisted of 0.1% w/v indomethacin, 2% w/v Compritol 888 ATO, 2.25% w/v glycerin, and 1% w/v surfactant (0.75% w/v Tween 80 and 0.25% w/v Poloxamer 188). The pH of the formulation was adjusted to 6.8. All experiments were performed in triplicates.
Effect of fraction of Tween 80
In this set of studies, a fraction of Tween 80 in the mixture of surfactants (Tween 80/Poloxamer 188+Tween 80) was varied, while keeping the total surfactant concentration at 1% w/v, and its effect on quality of IN-SLN dispersion was evaluated. Compritol 888 ATO was used as the lipid matrix (2% w/v); the aqueous phase consisted of glycerin (2.25% w/v), and homogenization was carried out at 15,000 psi for 6 cycles. The pH of the formulation was adjusted to 6.8. The particle size distribution and zeta-potential were measured 1 day post-preparation. Figure 3 represents the effect of fraction of Tween 80 concentration on the mean droplet size and PI of IN-SLNs. As the fraction of Tween 80 in the formulation increased from 0 to 0.75, a slight increase in the droplet size from 104±5 to 140±6 nm was observed. However, a significant difference in the PI was not observed. In contrast, IN-SLNs stabilized with only Tween 80 (1% w/v) as the emulsifier exhibited a significant increase in the particle size (251.0±5.0 nm) and PI (0.30±0.03) compared to all the other formulations. The zeta-potential values of the IN-SLNs stabilized with 0, 0.5, 0.75, and 1.0 fractions of Tween 80 were −23.8±2.0, −22.0±0.4, −21.0±1.8, and −20.0±2.0 mV, respectively.
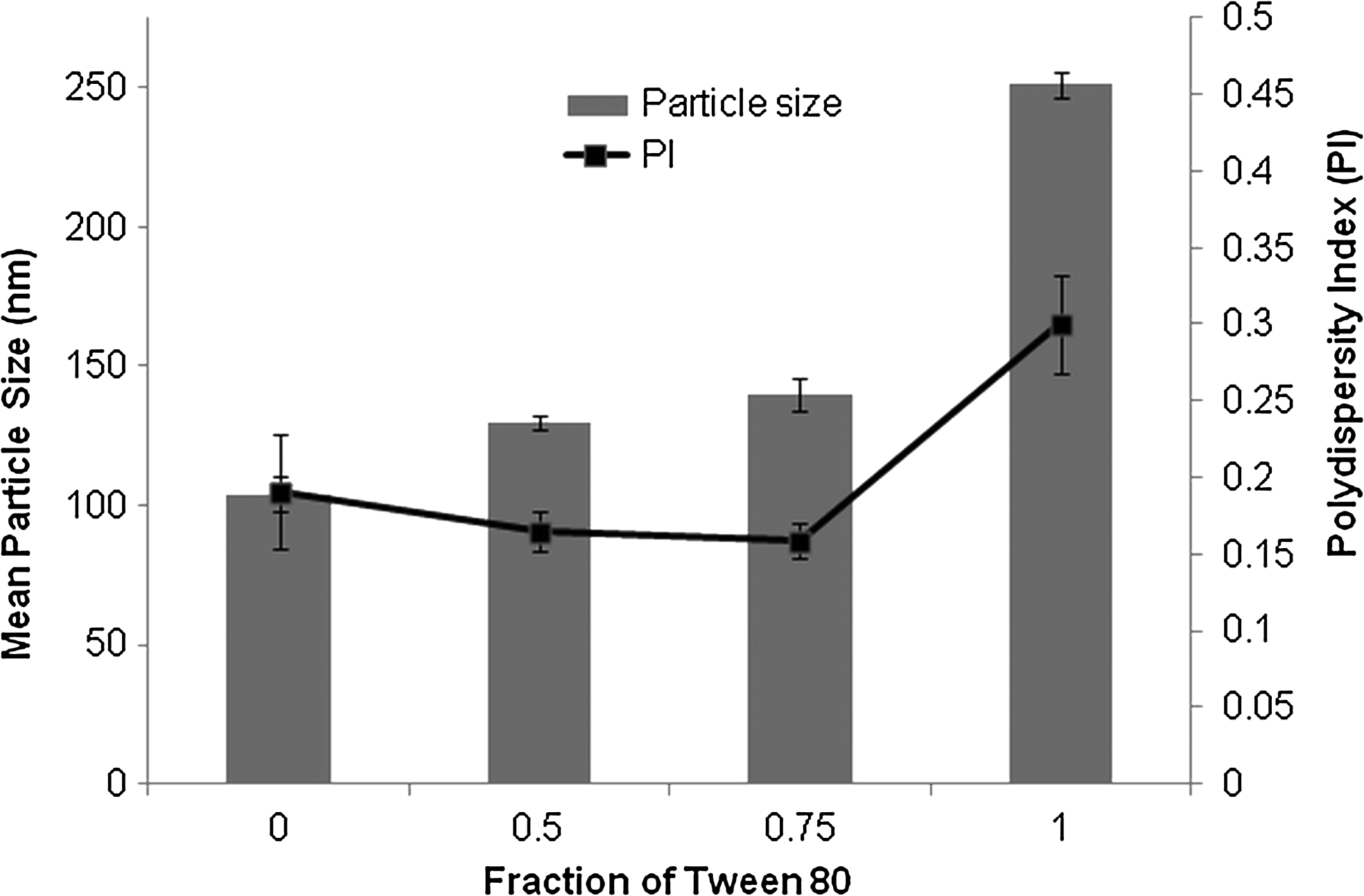
Effect of the fraction of Tween 80 in the mixture of surfactants (Poloxamer 188 and Tween 80; total concentration 1% w/v) on the mean particle size and PI of indomethacin-loaded solid lipid nanoparticles.
Solubility of indomethacin was observed to be highly dependent on the solution pH, and thus pH of the formulation could have a dramatic effect on the entrapment of indomethacin in the SLNs. Therefore, the effect of pH on EE (%) of IN-SLNs stabilized with 3 different fractions of Tween 80 (0, 0.5, or 0.75), while keeping the total concentration of surfactants at 1% w/v, was evaluated. IN-SLNs were adjusted to the pH values of 4.2, 5.5, 6.8, or 7.4 with HCL or NaOH (1 N) with each fraction of Tween 80. EE (%) was measured 1 day after adjusting the pH of the formulations. The effects of pH on the EE (%) of formulations stabilized by different fractions of Tween 80 are presented in Fig. 4. At all pH values tested, the IN-SLNs stabilized with only Poloxamer 188 (0% w/v Tween 80) as a surfactant demonstrated a lowest EE when compared to other formulations. As the fraction of Tween 80 in the formulation increased, a significant increase in the percent entrapment of indomethacin in the SLNs was observed, at all the pH values tested. For example, at pH 6.8, IN-SLNs stabilized with 0.75 fraction of Tween 80 demonstrated a highest EE of 72.0%±1.5% when compared to the formulation stabilized with the 0.5 (EE: 60.0%±2.0%) and 0 (EE: 51.0%±3.0%) fraction of Tween 80.
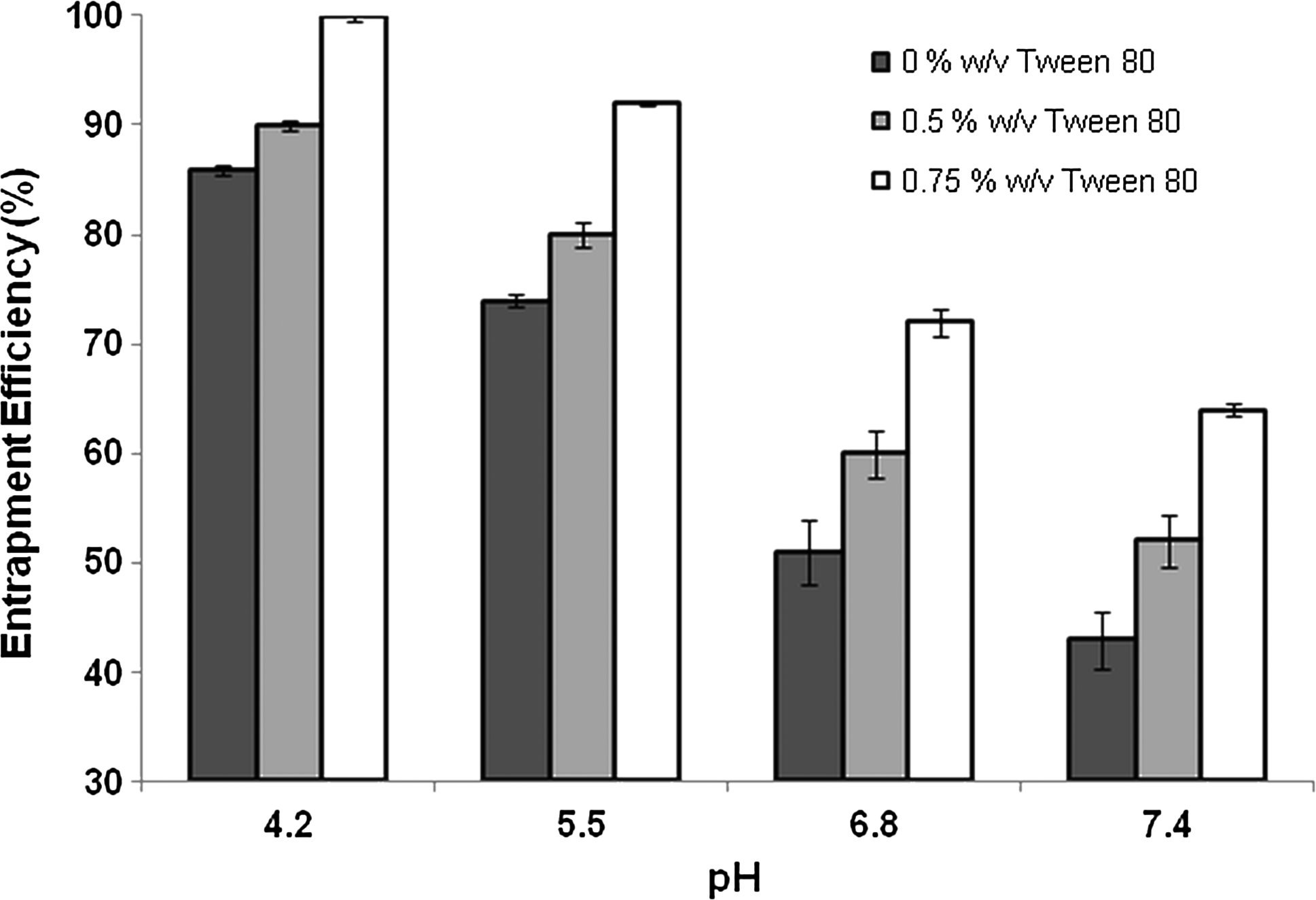
Effect of pH on the entrapment efficiency of indomethacin-loaded solid lipid nanoparticles stabilized with 0, 0.5, or 0.75 fraction of Tween 80 in the mixture of surfactants (Poloxamer 188 and Tween 80; total concentration 1% w/v). The results are depicted as mean±SD (n=3).
Optimized IN-SLN formulation
The optimized IN-SLN formulation was achieved using indomethacin (0.1% w/v), Compritol 888 ATO (2% w/v), Tween 80 (0.75% w/v), Poloxamer 188 (0.25% w/v), and glycerin (2.25% w/v), pH 6.8 and homogenization at 15,000 psi for 6 cycles. pH 6.8 was selected because Indocollyre, a commercial formulation in Europe, is marketed at this pH. At this optimized level, the particle size, percentage EE, PI, and zeta-potential of IN-SLNs were determined to be 140±5 nm, 72.0%±1.5%, 0.16±0.01, and −21±1.8 mV, respectively. This optimized formulation was used for further studies.
Effect of sterilization and storage
Three batches of the optimized IN-SLN formulation were sterilized by autoclaving (110°C for 30 min) and were subjected to storage stability studies at 40°C, 25°C, and 4°C for a period of 1 month (last time point tested). Table 1 represents the effect of sterilization on the physical parameters of the IN-SLNs. These parameters were evaluated 1 day after sterilization. Post-sterilization, the mean particle size, PI, zeta-potential, pH, and the percentage EE of the IN-SLNs were observed to be 149±5.0 nm, 0.17±0.03, −22±0.8 mV, 6.65±0.1, and 71.0%±0.2%, respectively. The significant difference in all the parameters tested after sterilization was not observed.
Results are depicted as mean±SD (n=3).
Figure 5 represents the effect of sterilization and storage on indomethacin drug content in the IN-SLN, IN-HPβCD, and IN-SOL formulations. In the case of the IN-SLN formulation, a significant decrease in the drug content was not observed poststerilization and on storage under the test conditions for a period of 1 month (last timepoint tested) (Fig. 5A). However, post-sterilization, the indomethacin content in the IN-HPβCD and IN-SOL formulations decreased from 100% to 84.0%±0.3% and 87.7%±0.25%, respectively (Fig. 5B, C). Additionally, further decrease in the drug content was observed in the IN-HPβCD and IN-SOL formulation on storage. At 40°C, 25°C, and 4°C, the drug content in the IN-HPβCD formulation decreased (from 84.0%±0.3%) to 67.0%±1.0%, 72.0%±0.5%, and 76.0%±0.3%, respectively, at the end of 1 month (Fig. 5B). In the case of IN-SOL formulation, at the end of 1 month, the drug content decreased (from 87.7%±0.25%) to 73.0%±0.9%, 79.0%±0.5%, and 81.0%±0.3% at 40°C, 25°C, and 4°C, respectively (Fig. 5C). Figure 6 represents the effect of storage of IN-SLNs at 40°C, 25°C, and 4°C on the mean particle size, zeta-potential, EE, and pH of IN-SLNs. A significant change was not observed in any of the parameters on storage for a period of 1 month (last time point tested).
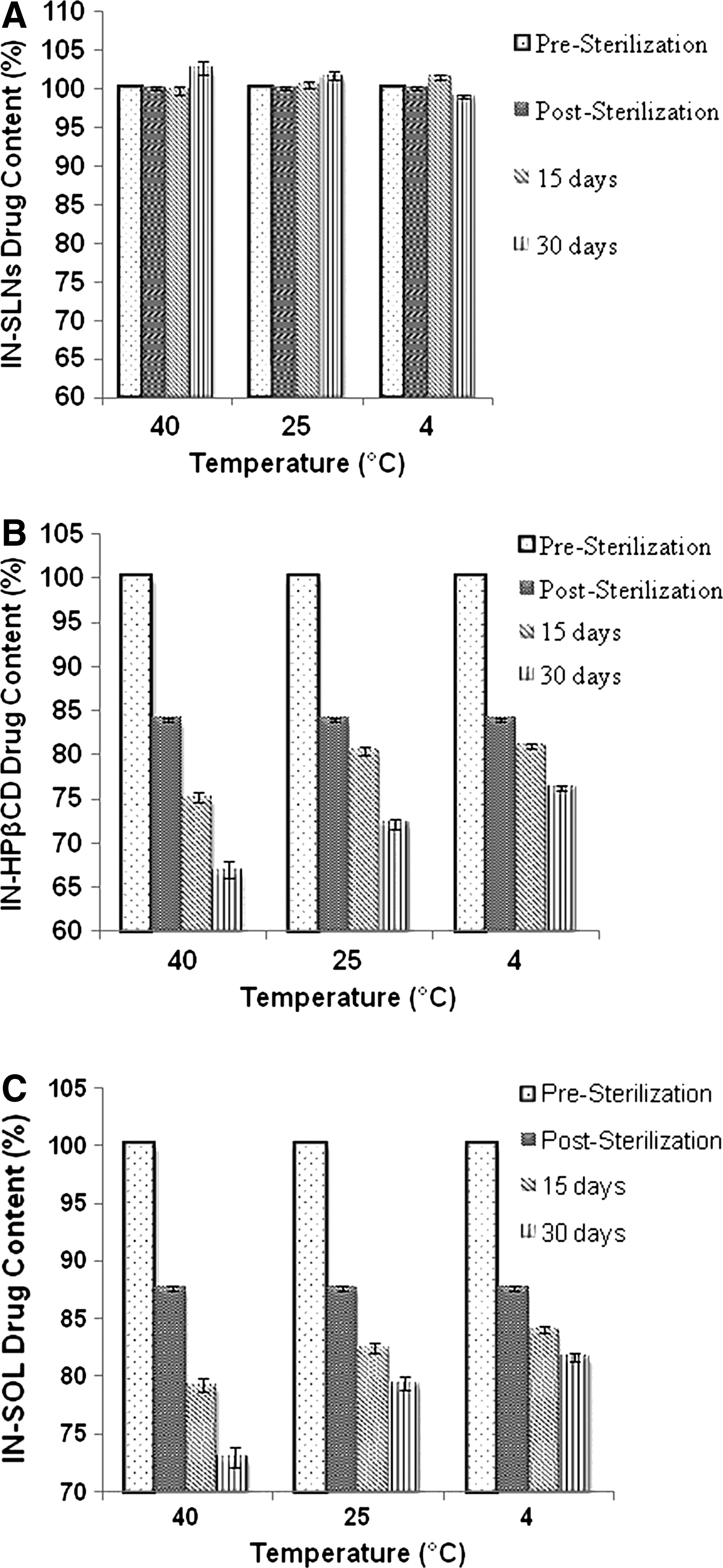
Effect of sterilization and 1-month storage under the test conditions on drug content in indomethacin-loaded solid lipid nanoparticle (IN-SLN)
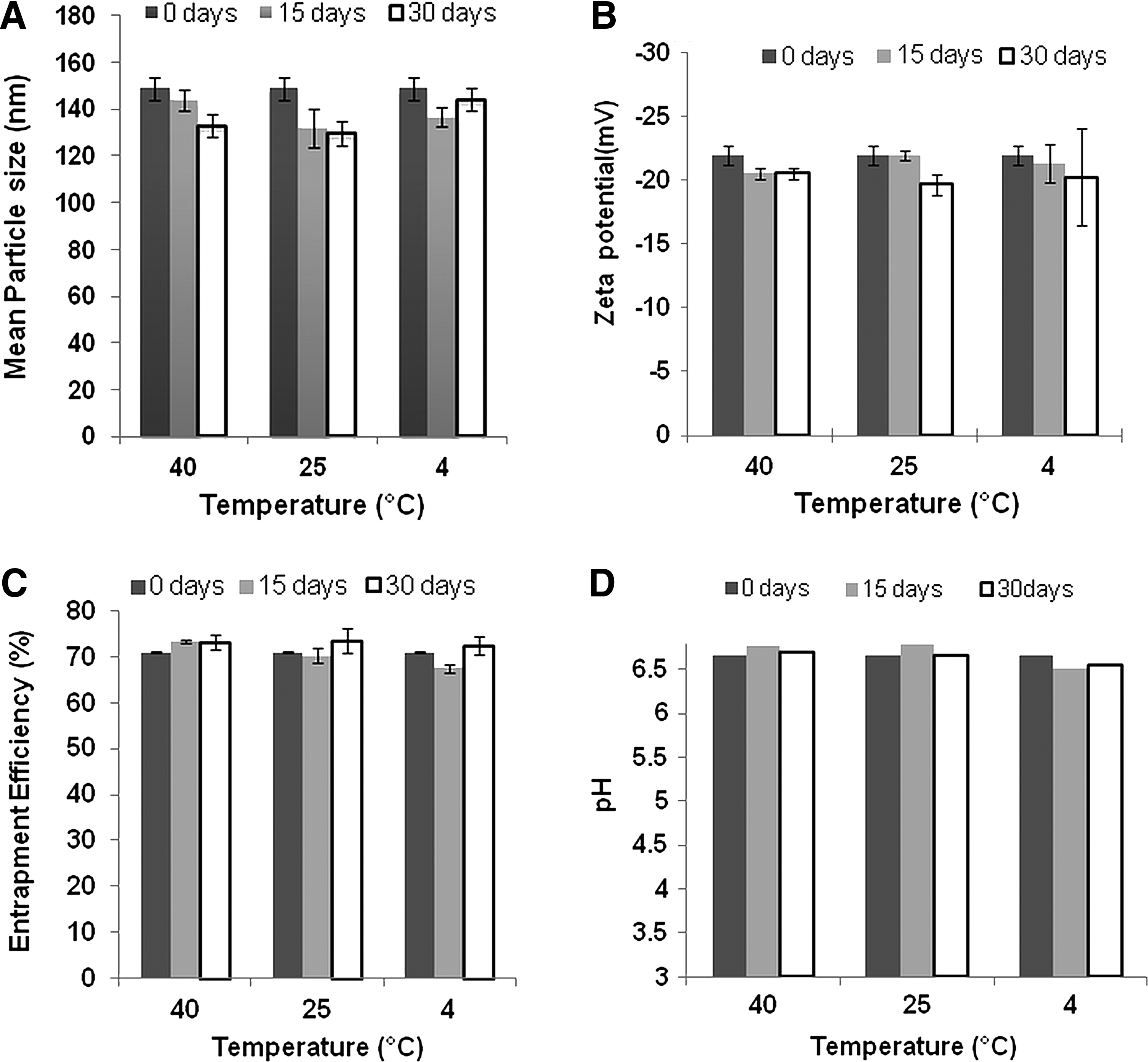
Effect of storage at 40°C, 25°C, and 4°C on the mean particle size
Differential scanning calorimetry
Perkin-Elmer Diamond DSC was used to investigate the melting and recrystallization behavior of the SLNs. DSC thermograms of indomethacin, Compritol 888 ATO, physical mixture (indomethacin and Compritol 888 ATO), lyophilized blank SLNs, and lyophilized IN-SLN formulation are presented in Fig. 7. Indomethacin exhibited an endotherm corresponding to its MP at ∼159°C. The thermal curve of the bulk Compritol 888 ATO and physical mixture (indomethacin and Compritol 888 ATO) exhibited an endothermic peak at ∼71°C. The melting endotherm of Compritol 888 ATO in lyophilized blank SLNs and IN-SLN formulation was observed at 69.03°C and 67.06°C, respectively. Additionally, an endotherm at 50°C–55°C corresponding to the MP of Poloxamer 188 was also observed in blank SLNs and IN-SLNs. Hyper-DSC thermograms (20°C–200°C at a heating rate of 200°C/min) of a physical mixture of indomethacin and bulk lipid exhibited a melting endotherm corresponding to melting of indomethacin at ∼158°C, which was absent in IN-SLNs (data not provided).
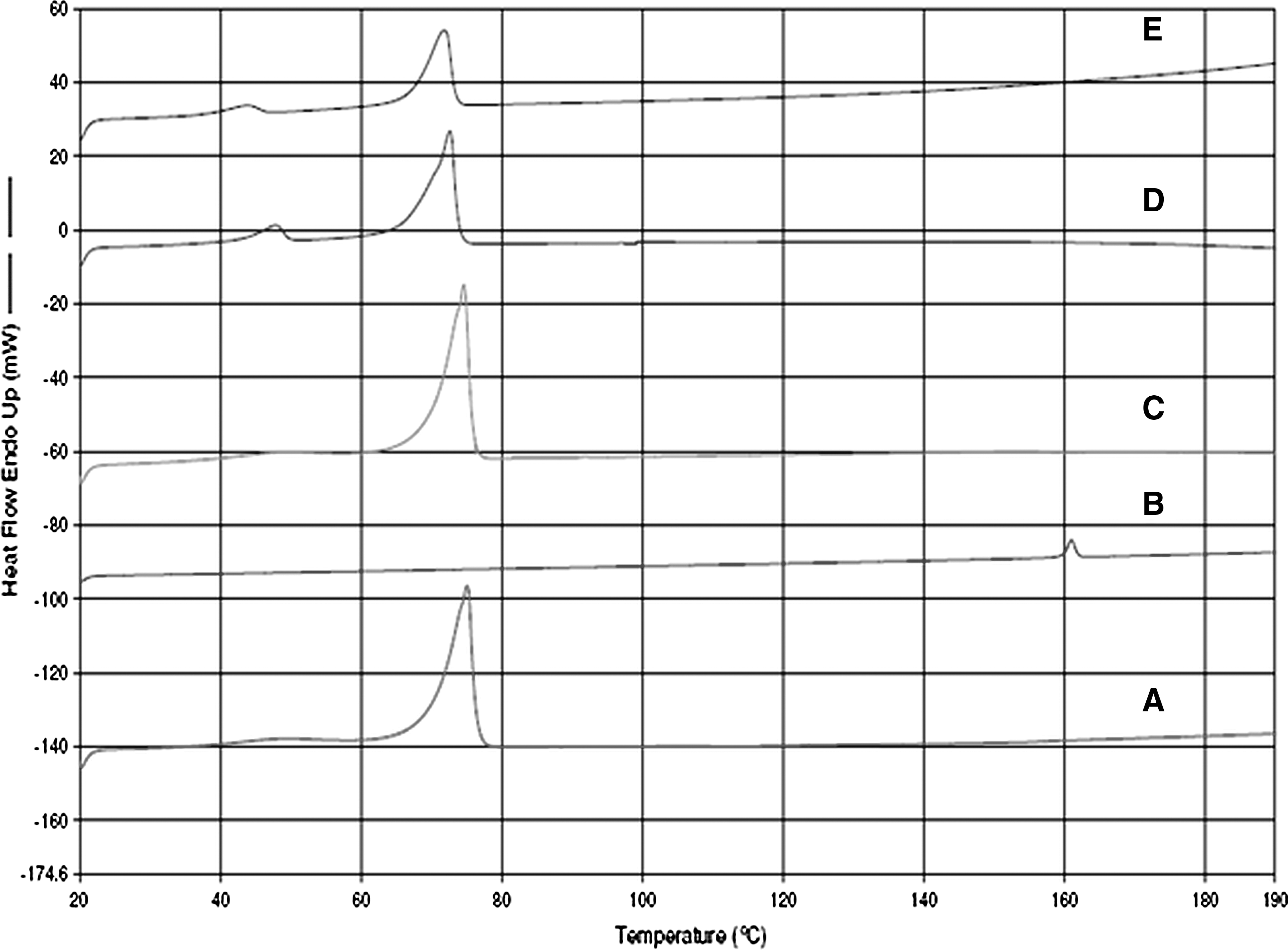
Differential scanning calorimetry thermograms of A: Compritol 888 ATO; B: Indomethacin; C: physical mixture (indomethacin and Compritol 888 ATO); D: lyophilized blank SLNs; and E: lyophilized IN-SLN formulation.
In vitro corneal permeation studies
In these studies, the donor solution consisted of 2 mL of the optimized IN-SLN formulation (0.1% w/v indomethacin content) (pre- and post-sterilization) or IN-SOL (0.1% w/v indomethacin content) or IN-HPβCD (0.1% w/v indomethacin content) diluted with 1 mL of 3 mM ACV solution (in DPBS, pH 7.4). The pH of the solution, immediately after dilution, was adjusted to 6.8, and the transport experiments were conducted. The receiver chamber solution contained 3.2 mL of 2.5% w/v HPβCD in DPBS (pH 7.4) in all cases. The transcorneal permeability coefficients of indomethacin, from all formulations tested, are depicted in Fig. 8. The in vitro transcorneal permeability of indomethacin from the IN-SOL and IN-HPβCD formulations was 2.7±0.48×10−6 and 4.0±0.9×10−6 cm/s, respectively. The IN-SLN formulation demonstrated a 4.5-fold and a 3-fold increase in the transcorneal permeability of indomethacin (12.2±1.85×10−6 cm/s). The transcorneal permeability of indomethacin from the IN-SLN formulation post-sterilization was observed to be 13.2±0.8×10−6 cm/s (Fig. 8). Figure 9 represents the permeation of ACV through the cornea, alone (control), or in the presence of IN-SOL, IN-HPβCD, and IN-SLNs (pre- and post-sterilization). One milliliter of ACV (3 mM in DPBS, pH 7.4) was added to 2 mL of, pH 6.8, DPBS (control) or to 2 mL of the formulations. The final pH of all formulations was adjusted to 6.8 before conducting transcorneal permeation. ACV was added to monitor/compare the integrity/tightness of the corneal tissues in the presence of the formulations and during the course of the experiments. The transcorneal permeability of ACV in the presence of IN-SOL (2.0±0.7×10−6 cm/s), IN-HPβCD (2.6±0.4×10−6 cm/s), pre-sterilized IN-SLNs (2.4±0.5×10−6 cm/s), and post-sterilized IN-SLNs (2.4±0.67×10−6 cm/s) formulations was not statistically different from that of ACV alone (control; 2.2±0.2×10−6 cm/s). The mean particle size, zeta-potential, pH, PI, and osmolality of the IN-SLN formulation before and after dilution with ACV were similar (Table 2). Additionally, on dilution with ACV, a significant difference in the osmolality of IN-HPβCD (predilution: 285±6 mOsm/kg H2O; postdilution 285±5 mOsm/kg H2O) or sterilized IN-SLNs (predilution: 280±3 mOsm/kg H2O; predilution: 280±5 mOsm/kg H2O) was not observed. However, on dilution with ACV, at the end of 3 h, a 36% decrease in the EE (from 72.0%±1.5% to 46%±4.0%) with the IN-SLN formulation was observed (Table 2). Figure 8 also represents transcorneal permeability of indomethacin from IN-HPβCD in the absence or in the presence of surfactants (0.75% Tween 80 and 0.25% Poloxamer). Transcorneal permeation of indomethacin from IN-HPβCD in the absence of and in the presence of surfactants was determined to be 4.02±0.84×10−6 and 4.47±0.33×10−6 cm/s, respectively.

Transcorneal permeation of indomethacin from the IN-SOL, IN-HPβCD, IN-HPβCD formulations containing 0.75% w/v Tween 80 and 0.25% w/v Poloxamer 188, and IN-SLN (pre- and poststerilization) formulations. Two milliliters of the formulations was diluted with 1 mL of acyclovir (3 mM in the Dulbecco's phosphate buffer saline, pH 7.4) solution. The indomethacin content in all the formulations was 0.1% w/v. The pH of all the final solutions was adjusted to 6.8 before conducting the transcorneal permeation studies. The results are depicted as mean±SD (n=6).
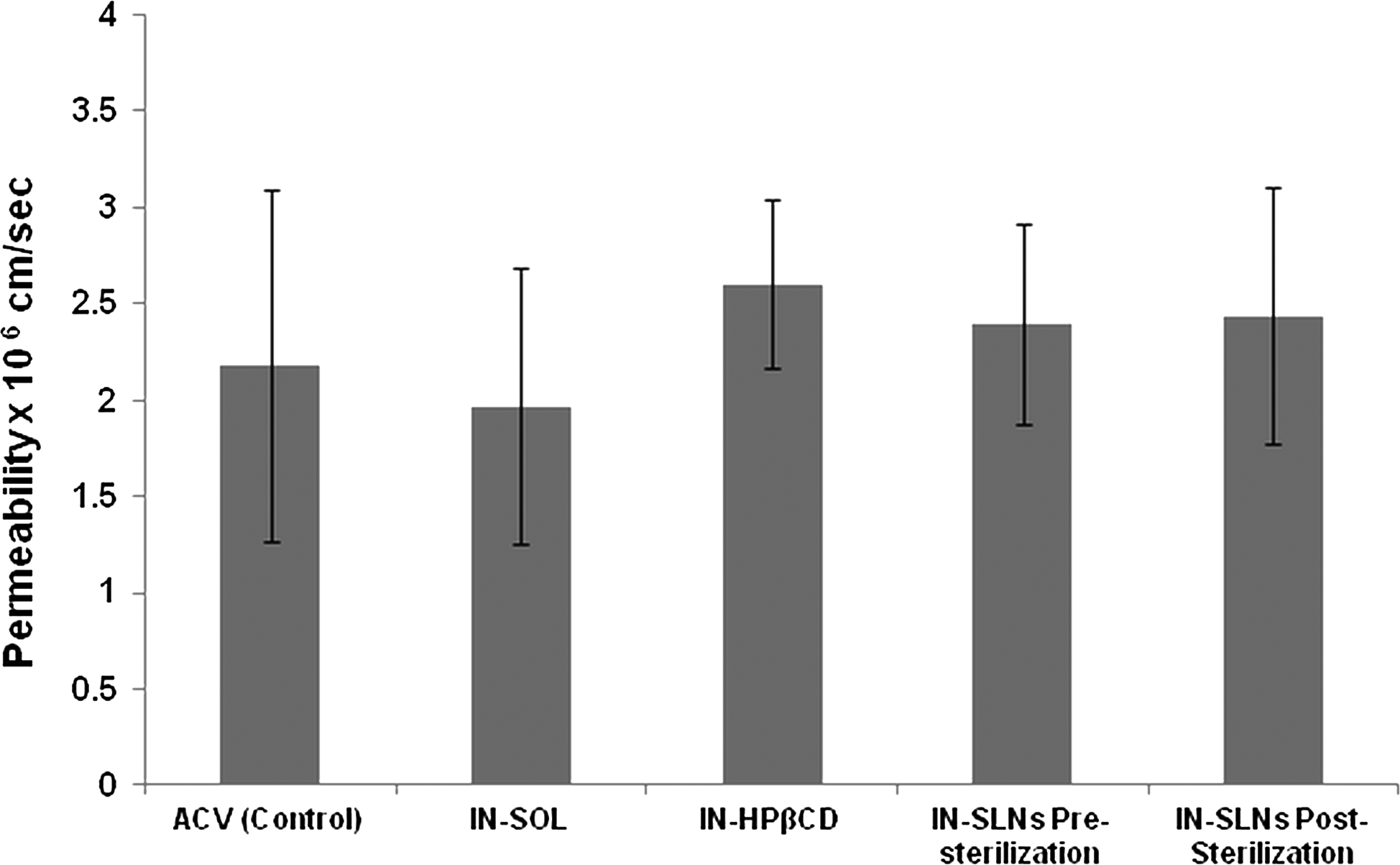
Transcorneal permeation of acyclovir (ACV), alone (control) or in the presence of the IN-SOL, IN-HPβCD, and IN-SLN (before and after sterilization) formulations. One milliliter of ACV [3 mM in the Dulbecco's phosphate buffer
Results are depicted as mean±SD (n=3).
IN-SLNs, indomethacin-loaded solid lipid nanoparticles.
Histology studies
The epithelial layer structure of the cornea exposed to the IN-SLNs did not show a significant difference from that of the control (Fig. 10), although there does seem to be some extracellular swelling in the corneal epithelium and separation of collagen lamellae in the anterior stroma.

Hematoxylin–eosin-stained corneal cross-sections exposed to
Discussion
The goal of this study was to develop and characterize IN-SLNs (0.1% w/v) and to compare in vitro corneal permeation of indomethacin from the IN-SLN, IN-SOL (0.1% w/v), and IN-HPβCD (0.1% w/v) formulations. The final indomethacin content in all the formulations was maintained at 0.1% w/v, because Indocollyre, a topical extemporaneously prepared hydro-PEG 400 solution of indomethacin, a commercial indomethacin formulation, is available in Europe at this concentration. Five factors, that is, the type of lipid, homogenization pressure, number of homogenization cycles, fraction of Tween 80 in the mixture of surfactants (Poloxamer 188 and Tween 80), while the keeping total surfactant concentration at 1% w/v, and pH were investigated for the preparation of the IN-SLNs. Efforts were directed toward minimizing the particle size, maximizing the EE, and maximizing the zeta-potential.
Solubility and EE of the drug, the determinants of the loading capacity of the drug in the lipids, are the 2 critical factors that drive the selection of the lipid phase for the preparation of the SLNs. Therefore, solubility of the drug in various lipids as well as its distribution between lipids and phosphate buffer (pH 6.8) were investigated. Indomethacin exhibited the highest distribution coefficient (10.1±0.8) in Compritol 888 ATO (Fig. 1), when compared to other lipids, indicating a better entrapment/loading efficiency of drug in Compritol 888 ATO. Additionally, in contrast to all the other lipids tested, indomethacin exhibited good solubility (clear yellow lipid melt) in Compritol 888 ATO (2 and 5 g), and the drug crystals were not observed under light microscopy 24 h after cooling to room temperature. Higher EE and drug solubility in Compritol 888 ATO could be attributed to the differences in the lipid crystalline structure related to the chemical nature of the lipid and arrangement of the drug molecules in the lattice. Compritol 888 ATO is a mixture of mono-, di-, and triglycerides and produces less-ordered lipid crystals with many lattice defects that help in accommodating the drug molecules compared to the other triglycerides tested (Dynasan 114, Dynasan 118, and Softisan 154). Although, Precirol ATO 5 (glyceryl palmitostearate) is also a mixture of mono-, di-, and triglycerides, higher solubility and entrapment of the drug in Compritol 888 ATO (glyceryl behenate) could be attributed to the differences in the chemical composition of the lipids. Therefore, Compritol 888 ATO was selected as the lipid phase for the preparation of the IN-SLNs. The final lipid concentration in all further formulations was maintained as 2% w/v, because an increase in the lipid content has been reported to result in a larger particle size with a broader size distribution. 21
Cavitational forces in the homogenization gap are responsible for the reduction in the particle size of the lipid nanoparticles. 22 To select the optimum pressure to prepare IN-SLNs, the pre-emulsion was passed through the high-pressure homogenizer at 3 different homogenization pressures. Increase in the homogenization pressure from 7,500 to 15,000 psi resulted in a decrease in the mean particle size of the IN-SLNs. Further increase in the homogenization pressure did not have any effect on the mean particle size of the IN-SLNs. Therefore, 15,000 psi was considered as the optimum homogenization pressure for the preparation of the IN-SLNs. For the selection of the optimum number of homogenization cycles at 15,000 psi, IN-SLNs stabilized with 1% w/v surfactant (0.75% w/v Tween 80 and 0.25% w/v Poloxamer 188) was passed through homogenizer from 1 to 10 cycles. The mean particle size and PI of IN-SLNs significantly decreased from single cycles to a plateau after 6 cycles, and further processing did not have a significant effect on both the parameters tested (Fig. 2). Thus, homogenization operating parameters of 15,000 psi and 6 cycles were selected for testing all further formulations.
The choice of the emulsifier and its ratio has an important impact on the quality of SLN dispersion.15,21 At optimized homogenization pressure and cycles, IN-SLNs (pH 6.8) stabilized with only Tween 80, as the emulsifier demonstrated a highest particle size and PI. As the fraction of Tween 80 in the formulation decreased, particle size and PI of the IN-SLNs was observed to decrease (Fig. 3). The observed differences in the particle size of the IN-SLNs stabilized using different combinations of surfactants could be explained by the different HLB values of Tween 80 (HLB 15), Poloxamer 188 (HLB 29), and the combination of Tween 80 and Poloxamer, which could lead to different surface absorption, and difference in the velocity of coverage of the new lipid surfaces and packing properties of the surfactants.17,23,24 However, a significant difference in the zeta-potential values of IN-SLNs with different fractions of Tween 80 was not observed, indicating that zeta-potential was not dependent on the fraction of Tween 80 in the formulation. In this set of studies, the pH of all the IN-SLN formulations was adjusted to pH 6.8, because Indocollyre (commercial indomethacin formulation in Europe) is marketed at this pH. However, interestingly, the EE of the formulations stabilized with Tween 80 or Poloxamer 188 or these mixtures was different, indicating that the fractions of Tween 80 in the formulation and the formulation pH had a significant effect on the EE. Therefore, to get further insight, studies were carried out to by preparing the IN-SLN formulation with different fractions of Tween 80 and adjusted to different pH values.
Indeed, both the fractions of Tween 80 in the formulation and the formulation pH had a significant effect on the percentage of indomethacin incorporated within the IN-SLNs (Fig. 4). Indomethacin (pKa of 4.5) demonstrated a pH-dependent EE, consistent with the pH-dependent solubility [section Results: Indomethacin-loaded solid lipid nanoparticles], which was expected, because the drug is known to be a weak acid and exists predominately in the ionized form above pH 4.5, which will promote localization in the aqueous phase. However, at all pH values, IN-SLNs stabilized with only Tween 80 (no Poloxamer 188) demonstrated a higher EE. As the fraction of Tween 80 in the formulation decreased, a significant decrease in the entrapment of indomethacin in the SLNs was observed at all pH values. Decrease in the entrapment with an increase in the concentration of Poloxamer 188 in the formulation could be attributed to the higher solubilization of the drug by Poloxamer 188 in the aqueous phase. The results are in agreement with the observation regarding the incorporation of diazepam and prednisolone in the SLNs, where the solubility of the drug in the aqueous–emulsifier phase was a determining factor for the EE.25,26 Based on the aforementioned discussion, optimization of the IN-SLN formulation was achieved with 15,000 psi, 6 cycles, indomethacin (0.1% w/v), Compritol 888 ATO (2% w/v), Tween 80 (0.75% w/v), Poloxamer 188 (0.25% w/v), glycerin (2.25% w/v), and pH 6.8. Although a higher EE could be obtained by adjusting the pH to lower values, the targeted pH of the optimized IN-SLN formulation was selected as 6.8, because Indocollyre is marketed at this pH. At these optimized levels, the particle size, percentage EE, PI, and zeta-potential of IN-SLNs were determined to be 140±5 nm, 72.0%±1.5%, 0.16±0.01, and −21±1.8 mV, respectively. This optimized formulation was used for further studies.
Recently, Castelli et al. prepared IN-SLNs by ultrasonication using Compritol as the lipid phase and Poloxamer 188 alone as the stabilizer. 27 The concentration of indomethacin and poloxamer was reported to be 2% w/w with respect to lipid and 1.35%, respectively. However, the formulation reported in this study was significantly different from that reported by Castelli et al. 27
In the present study, the IN-SLNs are prepared using high-pressure homogenization, and the drug loading is 5% w/w with respect to Compritol. Moreover, the optimized formulation contains a mixture of Tween 80 (0.75% w/v) and Poloxamer 188 (0.25% w/v). Additionally, in sharp contrast to Castelli et al., 27 in the present study, the formulation, process parameters, effect of sterilization, and stability of the IN-SLNs have been systematically evaluated. While Castelli et al. 27 reported IN-SLNs with polydispersed particle size distribution (particle population with diameter of 215.6 nm and a distinct particle population of 102.3 nm), in the present study, the optimized IN-SLN particle size was monodispersed with a mean particle size of 140±5 nm. The use of ultrasonication, nonoptimized formulation, and process parameters could be attributed to the observed polydispersity in the study reported by Castelli et al. 27 Moreover, the EE of the formulation reported by Castelli et al. 27 was 76%, and the pH of the formulation is not reported/considered. As demonstrated in the present study, the type and concentration of surfactant, their ratio, and formulation pH have a significant effect on the entrapment of the weakly acidic drug indomethacin in the SLNs. Further, the primary aim of the present study was to develop IN-SLNs for ocular delivery, whereas the aim of Castelli et al. 27 was to study organization and distribution of the different components in the IN-SLNs and nanostructured lipid carriers.
The pH and indomethacin content of the IN-HPβCD formulation was targeted to 6.8 and 1 mg/mL, respectively. Several reports indicate that maximum ocular permeation and bioavailability are achieved only when the cyclodextrin concentration is just sufficient to solubilize the available drug (saturation solubility). The presence of excess amounts of cyclodextrins decreases the ocular bioavailability due to retention of the drug molecule in the lipophilic central cavity of the cyclodextrins.28–31 The saturation solubility of indomethacin in 2.5% w/v HPβCD at pH 6.8 was determined to be 1.1 mg/mL. Thus, to avoid excess cyclodextrins in the formulation, IN-HPβCD was formulated using 2.5% w/v HPβCD.
All the ophthalmic products should be sterile, and physically and chemically stable on storage. 32 Indomethacin has been reported to undergo pH-dependent hydrolysis to 5-methoxy-2-methyl-indol-3-acetic acid and p-cholorobenzoic acid.1,33 The ability of SLNs to reduce hydrolysis, oxidation, and photodegradation of drugs as a result of incorporation into solid lipid matrices is well documented. 11 In this study, incorporation of indomethacin within the SLNs dramatically improved the chemical stability of indomethacin. A significant decrease in the drug content was not observed with the IN-SLN formulations on sterilization (110°C, 30 min) and on storage for up to a period of 1 month (last point tested) under the conditions tested (40°C, 25°C, and 4°C) (Fig. 5A). Additionally, the mean droplet size, zeta-potential, EE, and pH of the IN-SLNs remained unaltered post-sterilization and on storage (Fig. 6). However, a dramatic loss of indomethacin content from the IN-HPβCD and IN-SOL formulations was observed post-sterilization and on storage under the conditions tested (Fig. 5B, C).
The IN-SLN formulation was further characterized using DSC. The melting endotherm of indomethacin was not observed in the physical mixture of indomethacin and Compritol 888 ATO, because enough time was given for the drug to get solubilized in the bulk lipid that melts at ∼71°C (Fig. 7). However, in contrast to lyophilized IN-SLNs, when a physical mixture of indomethacin and Compritol 888 ATO was subjected to hyper-DSC (20°C–200°C at a heating rate of 200°C/min), a melting endotherm corresponding to melting of indomethacin at ∼158°C was observed (data not provided). This clearly indicates the presence of indomethacin in an amorphous state after entrapment within the SLNs. Additionally, the melting endotherm of bulk Compritol 888 ATO in blank SLNs shifted to lower temperatures (from ∼71°C to ∼69°C). The decrease in MP of the bulk lipid core in SLNs has been attributed to the small size of the SLNs, the dispersed state of the lipid, and the presence of surfactants.25,34–37 Nanoparticles have a large surface-to-volume ratio than the bulk materials that drastically alter the thermodynamic and thermal properties resulting in change in the MP. 38 The depression in the MP of the bulk lipid in the IN-SNLs (67.06°C) compared to that of blank SLNs (69.03°C) indicates increased lattice defects, resulting from the incorporation of indomethacin, which in turn reduces the degree of crystallinity and hence the MP of bulk lipid (Fig. 7). A similar decrease in the MP of the bulk lipid due to incorporation of the drug was previously reported. 39
Cornea is the major pathway for intraocular penetration of topically instilled medications.40–42 In vitro corneal permeability data suggest that incorporation of indomethacin in the SLNs led to a significant increase in the transcorneal diffusion of the drug. A 4.5-fold (from 2.7±0.48×10−6 to 12.2±1.85×10−6 cm/s) and a 3-fold (from 4.0±0.9×10−6 to 12.2±1.85×10−6 cm/s) increase in the corneal permeability of indomethacin from the IN-SLN formulations was observed compared to that from the IN-SOL and IN-HPβCD formulations, respectively (Fig. 8). Higher transcorneal permeation of IN-SLNs when compared to other formulations may be attributed to the corneal uptake of the nanoparticles by an endocytotic mechanism and due to release of the drug by the corneal enzymes. Using a confocal laser scanning microscopy (CLSM) analysis, Gokce et al. demonstrated cellular internalization (uptake) of Rhodamin B-loaded SLNs in the excised pig cornea. Additionally, intracellular release of Rhodamin B from SLNs was also observed probably due to an endosomal enzymatic activity. 16 Recently, Sandri et al. reported that, using CLSM, SLNs were localized, in particular, inside the corneal epithelium of excised pig cornea close to the cell nuclei due to an internalization/uptake mechanism for fluorescein isothiocyanate-chitosan-Compritol SLNs. 43 In another study, Yuan et al. evaluated the cellular uptake of SLNs with different lipid materials in A549 cancer cells and reported that the cellular uptake of glycerol tristearate SLNs was fastest when compared to SLNs of other lipids due to a small particle size (159.8 nm). 44
The transcorneal transport of indomethacin from the pre- and poststerilized IN-SLN formulations was comparable, which was expected since the physiochemical parameters of indomethacin remained unaltered on sterilization (Table 1). In contrast to the IN-HPβCD formulations that did not contain any surfactants, the IN-SLN formulations were stabilized with 0.75% Tween 80 and 0.25% Poloxamer 188, and these surfactants could be responsible for the observed increase in corneal permeation of indomethacin. To test this hypothesis, indomethacin from the IN-HPβCD formulation was permeated into the cornea in the presence of surfactants. The results demonstrate that permeation of indomethacin through the cornea was not modified in the presence of surfactants (Fig. 8). The transcorneal permeability of ACV (a positive control) in the presence of the formulations was not statistically different from that of the control, indicating that the integrity of the corneal epithelium was not affected by the formulation components (Fig. 9). The histology studies also did not suggest any major structural damage to the corneal epithelium (Fig. 10). However, in view of the observed extracellular swelling in the corneal epithelium, further investigations evaluating epithelial endocytosis of the SLNs and possible water-drag, and the effect of preservation of the excised cornea and exposure to the SLNs on endothelial cell function, as well as epithelial tight-junction protein expression, are needed.
Additionally, the mean particle size, zeta-potential, pH, PI, and osmolality of the IN-SLN formulation before and after dilution were similar, indicating that ACV did not affect the physical characteristics of the IN-SLNs during the transport experiments (Tables 1 and 2). A significant decrease in the EE of the drug in the IN-SLNs was not observed on storage at all the temperatures tested for a period of 1 month (last timepoint tested) (Fig. 6). However, on dilution with a 1 mM ACV solution, a 36% decrease in the EE of the drug was observed at the end of 3 h (Table 2), indicating that the release of indomethacin from the IN-SLNs was affected by partitioning of the drug between the lipid and the external aqueous phase. These results are consistent with the report by Calvo et al., wherein a rapid release of the encapsulated indomethacin (85% in 2 h), due to partitioning effect, from various colloidal formulations on dilution in a phosphate-buffered medium (pH 7.4) was observed. 7
Permeation studies were not undertaken with Indocollyre due to unavailability of the formulation in the United States. However, Calvo et al. compared the transcorneal permeability of indomethacin, in vitro, from various colloidal systems and Indocollyre. The transcorneal permeability of indomethacin from Indocollyre, emulsions, nanocapsules, and nanoparticles was reported to be 0.75±0.04×10−6, 2.74±0.49×10−6, 3.57±0.73×10−6, and 3.80±1.81×10−6 cm/s, respectively. In comparison to these results, in the present study, indomethacin permeability from the IN-SLNs (12.2±1.85×10−6 cm/s) was 16.2-fold higher compared to that of Indocollyre and 3.0-fold higher compared to that of the colloidal systems. 7
In conclusion, the results from this study demonstrate that IN-SLN formulation could dramatically improve the chemical stability and in vitro corneal permeability of indomethacin. Thus, IN-SLNs could significantly enhance the ocular bioavailability, including back of the eye ocular tissues, of the drug. Future experiments are aimed at evaluating the in vivo efficacy of these IN-SLNs.
Footnotes
Acknowledgments
This project was partially supported by the National Eye Institute, National Institutes of Health (Grant EY018426-02), National Institute of General Medical Sciences, National Institutes of Health (Grant P20 GM104932), and Health Resources and Services Administration (HRSA) (Grant DIBT16663).
Author Disclosure Statement
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or Health Resources and Services Administration.