
Abstract
Abstract
Purpose:
To investigate whether a self-reported history of allergy to sulfa-based drugs is a predictor for subsequent adverse reactions to topical carbonic anhydrase inhibitors (CAIs).
Methods:
A retrospective case-controlled cohort study via chart review was performed on 1,287 patients with a diagnosis of glaucoma. The outcome measure was the development of an adverse reaction (either ocular, systemic, or both) within at least 30 days after receipt of 1 of 4 classes of topical glaucoma medications: CAIs (dorzolamide and brinzolamide), prostaglandin analogues, beta-adrenergic blockers, and alpha2-adrenergic agonists.
Results:
Patients with a self-reported history of sulfa allergy had significantly more ocular adverse reactions after the initiation of any of the topical antiglaucoma medications when compared to those patients with no reported allergies. Patients with a self-reported sulfa allergy and patients who self-reported other, nonsulfa-related allergies had similar rates of adverse reactions to most of the topical medications. The patients reporting a sulfa allergy who used topical CAIs did not have more adverse reactions compared with patients who reported having other, nonsulfa-related allergies who used topical CAIs. Self-reported sulfa-allergic patients had similar rates of adverse reactions to topical CAIs compared with topical prostaglandin analogues.
Conclusion:
It may be safe to use a topical CAI in patients who report a history of a sulfa allergy. Patients with medication allergies of any kind may be more likely to develop allergic reactions to other, unrelated drug classes.
Introduction
Certain nonantibiotic, sulfa-containing medications have traditionally been avoided in patients who report a history of sulfa-based antibiotic allergies, even though the chemical composition of the antibiotic sulfonylarylamine sulfonamide and nonantibiotic, nonsulfonylarylamine compounds are quite different (Fig. 1). The nonsulfonamide medications, including dorzolamide, brinzolamide, and acetazolamide, are useful antiglaucoma agents, but traditional practice has been to avoid these medications in patients who report a sulfa allergy. Avoiding these glaucoma agents may contribute to the progression of glaucomatous vision loss, or hasten the decision for more risky options to control glaucoma, such as incisional surgery.
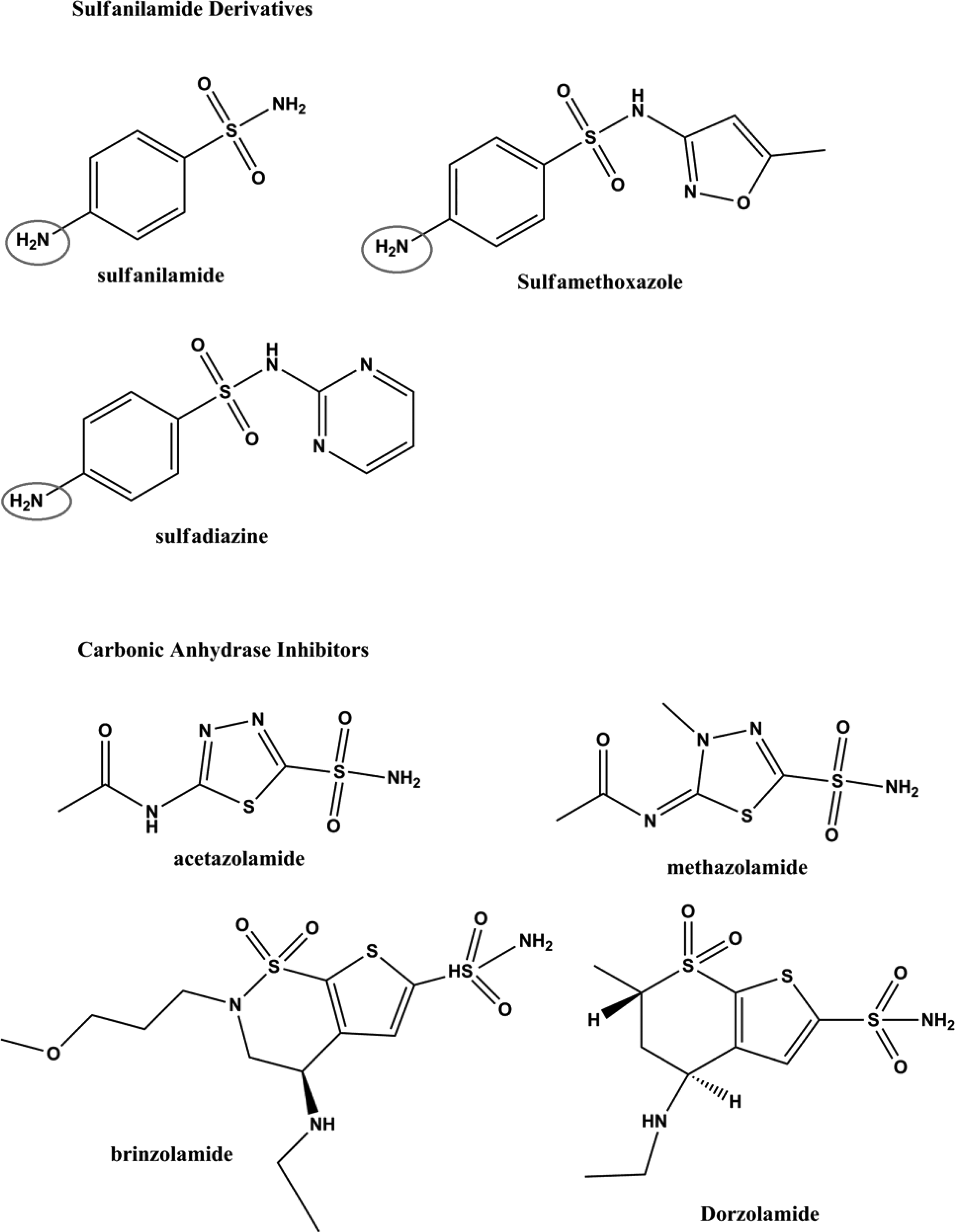
The sulfonamide antibiotics have an arylamine group (the R-NH2, which is circled, with the R group being an aromatic ring), while the carbonic anhydrase inhibitors (CAIs) (nonantibiotics) do not contain an aromatic amine.
At issue is whether a history of allergy to a sulfa-based antibiotic is a predictor for a subsequent allergic reaction to a structurally different compound containing a sulfa group, such as the nonsulfonylarylamines. To answer this question, we conducted a retrospective case-controlled cohort study to investigate adverse events in glaucoma patients with self-reported sulfa allergy who were using sulfa-containing or nonsulfa-containing antiglaucoma medications. As with the typical clinical experience, this retrospective study did not involve formal allergy testing to confirm self-reported medication allergies, nor were formal allergy tests used to confirm the allergic nature of patients' adverse reactions. 4 For this reason, this study measured adverse reactions, not necessarily true allergic reactions, to topical glaucoma medications in patients who self-reported a sulfa allergy. We also examined adverse events in glaucoma patients with unconfirmed, self-reported allergies to other nonsulfa-containing medications who were using topical antiglaucoma medications, such as carbonic anhydrase inhibitors (CAIs), prostaglandin analogues, alpha2-adrenergic agonists, and beta-adrenergic blockers.
Methods
A retrospective case-controlled cohort study via chart review was performed on 1,287 patients with a diagnosis of glaucoma who were seen by 2 of the authors (M.B.S. and H.R.M.) during the year of 2009. The study was approved by the Yale University School of Medicine Human Investigation Committee. All charts were collected and reviewed from the archives of the Yale Eye Center. Demographic information, prescription-drug information, indications for all new prescriptions, surgeries, clinical events, diagnoses, and physicians' notes were documented. Inclusion criteria for the source population were (1) a clinical diagnosis of primary open-angle, pigment dispersion, or exfoliation glaucoma, or ocular hypertension in at least 1 eye, (2) treatment with the topical CAIs dorzolamide or brinzolamide, or with prostaglandin analogues, beta-adrenergic blockers, or alpha2-adrenergic agonists, (3) at least 1 follow-up visit after 4 weeks of therapy.
Exclusion criteria included (1) patients who started more than 1 topical medication at the same time, (2) patients who underwent surgery less than 4 weeks after the initiation of topical medical therapy, (3) patients using oral sulfa-based medications such as acetazolamide or methazolamide.
The typical practice to elicit an allergy history in the authors' clinic was for a technician, resident, or attending physician to ask an open-ended question, “Do you have any allergies to medications?” The vast majority of patients simply reported having a sulfa allergy or allergy to some other medication. No efforts were made to interpret, characterize, or quantify the nature of a patient's self-reported allergies that were recorded in the chart. No confirmatory or formal allergy testing was performed to verify a patient's self-reported allergy history. Only a few patients identified a named medication, such as Bactrim or Aspirin. No efforts were made to identify or classify details regarding the class of sulfa medication patients reported. The typical clinical practice of M.B.S. and H.R.M. was to discuss the higher possible risk of allergic reactions to topical CAIs in patients who self-reported a sulfa allergy, when initiating therapy. The physician's decision to prescribe CAIs to these patients was based on the determination that the benefits outweighed the potential risks of other intraocular pressure-lowering alternatives.
The study group comprised of patients from the cohort who self-declared a sulfa allergy. The control groups were patients from the cohort who self-declared either no medication allergies, or allergies to nonsulfa medications. To randomize the controls, the control group patients were chosen if they had Yale medical record numbers that were one before or one after each study group patient's record number. This randomization was formed on the assumption that the order in which patients arrived at the clinic and were assigned medical record numbers followed a random pattern. Each topical glaucoma medication used by the patient was counted only once in the analysis. If a patient used more than 1 topical glaucoma medication, it was under the condition that there was a 1-month gap between start of the drug usage. The 4 study groups were divided by which 1 of the 4 medication classes a patient was using; the 4 control groups were decided on this criterion as well.
Because ascertaining true allergic events in the clinical setting is often difficult, and no formal allergy testing was performed in this retrospective study, the primary outcome measure was the development of an adverse reaction (either ocular, systemic, or both) within at least 30 days of initiation of a topical glaucoma medication. Adverse reactions were defined in this study as reactions significant enough to cause discontinuation of treatment. Adverse ocular reactions included itching, eyelid swelling, intolerable conjunctival hyperemia, chemosis, mucoid discharge, significant papillary or follicular reaction, or eyelid dermatitis. Adverse systemic reactions included urticaria, anaphylactic shock, erythema multiform, asthma, and eczema. Statistical analysis was carried out using 2-proportion chi square tests with a significance level of 0.05. Cross testing was conducted across classes of drugs and across allergy histories.
Results
The study group consisted of 94 self-reported sulfa-allergic patients from the study's source population. The control group consisted of 205 randomly selected patients from the study's source population with glaucoma who self-reported no medication allergies or nonsulfa medication allergies. The study and control groups were evenly matched by race, gender, and age (Table 1).
Patients with previous self-reported sulfa allergy had significantly more ocular adverse reactions after the initiation of any of the topical antiglaucoma medications when compared to those patients with no self-reported allergies (Table 2). Patients who reported a history of a sulfa allergy and patients who reported other, nonsulfa-related allergies had statistically similar rates of reactions to most of the topical medications.
This includes ocular and systemic adverse reactions.
CAI, carbonic anhydrase inhibitor.
The self-reported sulfa-allergic patients using topical CAIs did not have more adverse events than patients who reported other, nonsulfa-related allergies, and did not have a higher rate of adverse reactions than did self-reported sulfa-allergic patients using prostaglandin analogues (Table 3). Patients who reported a history of a sulfa allergy developed significantly more adverse reactions using topical alpha2-adrenergic agonists than self-reported sulfa-allergic patients using a topical CAI (P<0.05) (Table 4). Patients who reported a sulfa allergy had a significantly higher rate of ocular adverse reactions after starting topical alpha2-adrenergic agonists compared to both the group of patients who reported a history of nonsulfa-related medication allergies and the group who reported no history of medication allergies. The self-reported sulfa-allergic study group had a significantly lower number of adverse reactions to topical beta-adrenergic blockers when compared with self-reported sulfa-allergic patients using any other medication class (P<0.05).
Some patients have sulfa allergy as well as other allergies.
P-value=0.052.
The rates of systemic (nonocular) reactions to topical antiglaucoma medications were not significantly different between the medication classes. The only systemic reactions that patients experienced were rash, skin swelling, erythema multiform, and severe vomiting. No patients experienced anaphylaxis.
Discussion
There is little published biochemical or clinical evidence to support the assumption that prior allergic reactions to sulfonamide-based drugs increases susceptibility to allergic reactions from all sulfa-based drugs. 5 There are significant structural differences between sulfonamide antibiotics and other sulfonamide medications such as CAIs. While sulfonamide antibiotics contain an arylamine (R-NH2 where R is an aromatic ring), the chemical structure that has been proposed to be responsible for the sulfonamide hypersensitivity reactions, other sulfonamide-containing medications do not have this aromatic amine. 6 In addition, sulfonamide antibiotics contain a 5- or 6-member aromatic heterocyclic ring and one or more nitrogen groups at the sulfonamido-N1 position, chemical structures that are not present in CAIs.7,8
A previous study by Lee et al. that evaluated self-reported sulfa-allergic patients who were using oral nonbacteriostatic sulfonamides acetazolamide and/or furosemide found that 7% of patients developed urticaria and no patients developed a severe allergic reaction. 8 Similarly, a study by Strom et al. found that patients taking a nonantibiotic sulfonamide who had a self-reported sulfa allergy had equal rates of allergic-type reactions when compared to those patients who self-reported allergies to any type of medication. 3
Our retrospective study measured adverse events that were significant enough to necessitate discontinuation of topical medical therapy. No efforts were made to differentiate the features of patients' self-reported allergies, and no patients in our study had formal testing to determine if they had true allergies to sulfa or other medication, or true allergic reactions. In agreement with previous reports that evaluated oral medications (that also did not confirm true allergic reactions), our study, evaluating patients using topical glaucoma medications, found that patients who self-reported a sulfa allergy had more adverse events than patients with no self-reported allergies. In addition, the self-reported sulfa-allergic patients had equal amounts of adverse reactions to sulfa-based medications compared with patients who self-reported allergies to nonsulfa-based medications. Our study found that self-reported sulfa-allergic patients had the highest rate of local adverse reactions to alpha2-adrenergic agonists, and the lowest rate of local adverse reactions to topical beta-adrenergic blockers, similar to previous reports of adverse reactions to topical glaucoma medications in patients who report no medication allergies.
There is uncertainty regarding the underlying cause for the results seen in this study, primarily the finding that patients who reported a previous allergy to any medication were more likely to have an adverse event to topical medications compared with patients who reported no medication allergies. It is possible that some patients are less tolerant of the medication side effects, and more likely to voice discomfort or report adverse events. It is also possible that some patients may have an immunologic basis for hypersensitivity to various chemical compounds, including medication excipients, such as preservatives. It would be valuable to further investigate the nature and significance of cross-reactivity events for true and self-reported medication allergies.
This study has a number of limitations. The retrospective nature of the study makes it difficult to control for many variables; most notably, clinicians may have avoided prescribing topical CAIs in patients who reported a history of severe reactions to sulfa medications (e.g., Stevens Johnson's or anaphylaxis), only prescribing topical CAIs for sulfa-allergic patients who reported a remote or mild allergic reaction. There was a greater number of women than men in our study, and a preponderance of Caucasians, but these differences were consistent between the various groups. We attempted to identify a large case-controlled cohort in an effort to reduce random sampling errors and bias. It is possible that an allergic or adverse reaction could develop later than a month after the initiation of therapy. The 30-day window was selected because most hypersensitivity reactions to drugs occur within several weeks of administration and a shorter study period may better control confounders. 5 It is possible that patients developed a reaction to the cumulative exposure to multiple or chronic medications, but this cumulative exposure experience should have been similar across all the study groups. The self-reported nature of patients' allergies is an inherent limitation, but it represents the limits of a typical personal medical history taken in a daily clinical practice. It is likely that this cohort includes many patients who do not have a true sulfa allergy because confirmatory or formal allergy testing was not done to ascertain the verity of the self-declared sulfa allergy history. It is difficult to distinguish between a true allergic reaction, chemical sensitivity, and individual medication intolerance, which is why we elected to record adverse events that were significant enough to warrant cessation of therapy. Utilizing adverse events may result in an over-estimation of the actual incidence of true allergic events.
In conclusion, we found no significant difference in the rate of adverse events in self-reported sulfa-allergic patients who were using topical sulfa-containing CAIs compared with self-reported sulfa-allergic patients who were using topical prostaglandin analogues or beta-adrenergic blockers. Patients who reported allergies to any kind of medication, sulfa and nonsulfa containing, were more likely to develop an adverse reaction to topical antiglaucoma medications than patients who reported no allergies to medications. Finally, self-reported sulfa-allergic patients were most likely to have an adverse reaction to topical alpha2-adrenergic agonists, and were most tolerant of topical beta-adrenergic blockers, compared with the other classes of medications.
The results of this study suggest that it may be reasonable to initiate therapy with a sulfa-containing topical antiglaucoma CAI in a patient who reports a sulfa allergy. It would be prudent, however, for clinicians to investigate the nature and severity of prior adverse reactions to sulfa medications. Clinicians should exercise caution before recommending the use of sulfa-containing CAIs in patients with sulfa allergies or any allergy history, inform patients of the low, but potentially significant possibility of adverse reactions, and follow patients carefully for the development of adverse reactions.
Footnotes
Disclosure of Funding
Unrestricted departmental grant from Research to Prevent Blindness.
Author Disclosure Statement
No competing financial interests exist.