
Abstract
Abstract
Objective:
To evaluate the efficacy and tolerability of the fixed-combination brimonidine 0.2%/timolol 0.5% (FCBT) compared with the fixed-combination dorzolamide 2%/timolol 0.5% (FCDT) in the treatment of patients with elevated intraocular pressure (IOP).
Methods:
Pertinent randomized controlled trials comparing FCBT with FCDT in patients with elevated IOP were identified through systematic searches of the Cochrane Library, PubMed, and EMBASE. The main efficacy measures were the IOP reduction (IOPR), including diurnal mean IOPR, and peak IOPR. The main tolerability measure was the individual adverse events. The pooled estimates and 95% confidence intervals (CIs) were carried out in RevMan version 5.0 software.
Results:
Seven studies involving 582 patients were included in the meta-analysis. With a weighted mean difference (WMD) of IOPR in diurnal mean of 0.44 mmHg (95% CI, 0.00–0.88), the FCBT was as effective as FCDT in lowering IOP in patients with elevated IOP (P=0.05). The WMD of IOPR at peak was 0.65 mmHg (95% CI, −0.06 to 1.35) (P=0.76), and there was no significant difference between FCBT and FCDT. FCBT caused burning/stinging in less patients than FCDT [pooled relative risk: 0.45 (95% CI, 0.29–0.70)].
Conclusions:
Both FCBT and FCDT can effectively lower IOP in patients with elevated IOP, and the IOP-lowering efficacy of FCBT is noninferior to that of FCDT. Additionally, FCBT affords an ocular comfort advantage compared with FCDT.
Introduction
The modern goals of glaucoma management are to avoid glaucomatous nerve damage and preserve visual field and total quality of life for patients with minimal side effects.2,3 The elevated intraocular pressure (IOP) is one of the major risk factors for glaucoma and lowering it via various pharmaceuticals and/or surgical techniques is currently the mainstay of glaucoma treatment. The Early Manifest Glaucoma Trial showed that IOP-lowering treatment decreased the risk of glaucoma progression by half. Moreover, progression risk decreased about 10% with each millimeter of mercury (mmHg) of IOP reduction from baseline. 4
Topical medical therapy is the most common first-line treatment and many topical medications are available for lowering IOP. 5 However, many patients need multiple medications to lower their IOP to target levels. 5 The more medications used, the more complicated the treatment regimen becomes and patient compliance becomes a concern.6,7 When multiple medications are required, the use of a fixed combination of two IOP-lowering medications offer several advantages over the concomitant use of the individual components. 8 Fixed combinations allow the simplification of a multi-drug regimen by reducing the total number of drops instilled per day and may improve adherence to chronic therapy in glaucoma patients. Fixed combinations of IOP-lowering medications have been developed by combining different pharmacologic classes of ocular hypotensive drugs commonly prescribed. 9
Fixed combinations of brimonidine 0.2%/timolol 0.5% (FCBT) and dorzolamide 2%/timolol 0.5% (FCDT) are frequently used products in primary open-angle glaucoma (POAG). 9 Many previous studies compared the efficacy of FCBT with FCDT. Some reported that FCBT treatment was more effective in reducing IOP than FCDT,10,11 whereas others concluded that both drugs had similar efficacy.12–15 Furthermore, a recent study reported that FCDT provides better efficacy. 16 These conflicting results make it difficult to draw conclusions that could be applied in clinical practice.
To determine whether FCBT offers any advantages over FCDT for IOP control, in terms of enhanced efficacy and fewer adverse events, we undertook a meta-analysis of relevant randomized controlled trials.
Methods
We attempted to identify, all randomized controlled trials (RCTs) carried out to assess the effects and tolerability associated with the use of FCBT when comparing to FCDT in patients with elevated IOP.
Outcome measures
The outcome measure of efficacy was the reduction from baseline to end of treatment in IOP [IOP reduction (IOPR)] at peak and diurnal mean. Baseline was defined as the time point after a washout period for patients using anti-glaucoma medications or at time of diagnosis for newly diagnosed patients. Peak refers to the moment as 2 h after morning administration of FCBT and FCDT (with a range of ±1 h). Diurnal mean IOP was defined as the average mean outcomes measured throughout the assessed day. We also assessed tolerability of the drugs by considering the proportions of patients with individual adverse events.
Search strategy
RCTs that compared the effects of FCBT and FCDT were identified using a systematic search of MEDLINE, EMBASE, and CENTRAL databases.
The search combined terms related to brimonidine (including MeSH search using exp “receptors, adrenergic, alpha-2” and exp “brimonidine”), terms related to dorzolamide (including MeSH search using exp “carbonic anhydrase inhibitors” and exp “dorzolamide”) and terms related to timolol (including MeSH search using exp “adrenergic beta antagonists” and exp “timolol”). The limit for the search was clinical trial.
Trials selection
Published studies fulfilling the following criteria were included in this meta-analysis: (1) study design: randomized clinical trials; (2) population: patients with elevated IOP; (3) intervention: FCBT versus FCDT after a wash out period; (4) outcome variables: IOPR. Only trials meeting these criteria were assessed for methodological quality.
Data extraction
A customized form for data extraction, which was described in the Cochrane Handbook for Systematic Reviews of Intervention, 17 was used to record the authors of the study, the year of publication, information on study design (whether randomization, allocation concealment, intention to treat analysis, double blind or single blind, parallel or crossover), interventions, length of study, number of subjects, patients age, sex, type of glaucoma, and IOP measurements. In addition, we recorded the proportion of withdrawals and number of patients reporting adverse events.
Qualitative assessment
We used standard criteria [allocation concealment, blinding, intention-to-treat (ITT) analysis, lost- to-follow-up] for appraising the quality of each study, and also quantified the quality assessment by using the scoring system developed by Jadad et al. 18
The quality scoring system was as follows: (1) allocation concealment, coded as adequate (score 1), inadequate or unclear (score 0); (2) blinding, coded as double blind (score 2), single blind (score 1), and open label (score 0); (3) ITT analysis, coded as used (score 1), not used or unable to assess (score 0); and (4) lost to follow-up, coded as data given (score 1), and data not given (score 0). A Jadad score <3: poor quality.
Statistical analysis
Statistical analysis was performed using RevMan version 5.0 (Cochrane Collaboration, Oxford, United Kingdom). Outcome measure was assessed on an ITT basis, with the ITT population comprising all randomized patients who received study medications and had valid baseline data available. Relative risk (RR) was estimated for dichotomous outcomes. Weighted mean difference (WMD) was calculated for continuous outcomes. When mean and standard deviation (SD) of IOPR were reported, we used them directly. When these data were not available, they were computed as follows, according to the methods described in the Cochrane Handbook for Systematic Reviews of Interventions 17 : IOPR=IOPbaseline−IOPendpoint and SDIOPR=(SD2baseline+SD2endpoint−SDbaseline×SDendpoint)1/2. When standard error (SE) was reported, SD=SE×N1/2. We used the Q statistic for all comparisons so as to evaluate heterogeneity of treatment effects between studies. Heterogeneity was checked by P-value. 19 If no heterogeneity was detected (P>0.1), we combined the results in a meta-analysis using the Mantel–Haenszel fixed effects model. 20 Results were presented with 95% confidence intervals (95% CIs). P<0.05 was considered statistically significant. To detect publication biases, asymmetry in funnel plots was visually examined.
Results
Overall, 7 RCTs that met our inclusion criteria were included in the meta-analysis, involving 582 patients with elevated IOP.10–16 The flow of the studies included in our analysis is shown in Fig. 1. Four studies were conducted at multiple sites. Three trials had a prospective, parallel design, and others had a prospective, crossover design. The duration of the studies ranged from 4 weeks to 6 months. The mean age of patients in the studies ranged from 56 to 72 years. Among the 512 patients for whom data on sex were available 213 (41.6%) were male and 299 (58.4%) were female.
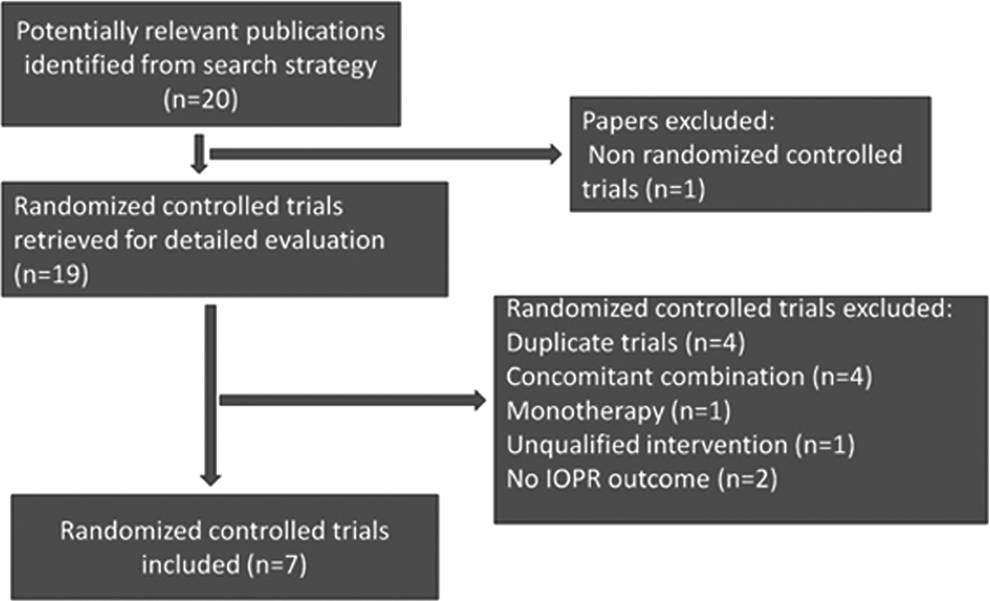
Flowchart of the trials included in the meta-analysis.
The baseline characteristics of the included studies are summarized in Table 1. Four trials scored 4, two scored 3, three scored 3, and one scored 2. Allocation concealment was adequate in 6 studies, and unclear in 1 study. Treatment was assigned in a randomized fashion. Participants were blinded in 1 study, investigators in 5 studies, and examiners in 6. Finally, patients were analyzed by the ITT principle in 5 of the studies (Table 2).
POAG, primary open angle glaucoma; OH, ocular hypertension; IOPR, intraocular pressure reduction; PG, parallel group; CR, crossover; DB, double blind; SB, single blind; OL, open label; FCBT, fixed-combination brimonidine 0.2%/timolol 0.5%; FCDT, fixed-combination dorzolamide 2%/timolol 0.5%; PGA, prostaglandin analogue; NR, not reported; PXG, pseudoexfoliative glaucoma; ITT, intention-to-treat; PP, per protocol; SD, standard deviation.
Funnel plots for the studies comparing FCBT with FCDT on the reduction in IOP at peak and diurnal mean are qualitatively symmetrical, which indicated the absence of publication bias (Fig. 2).
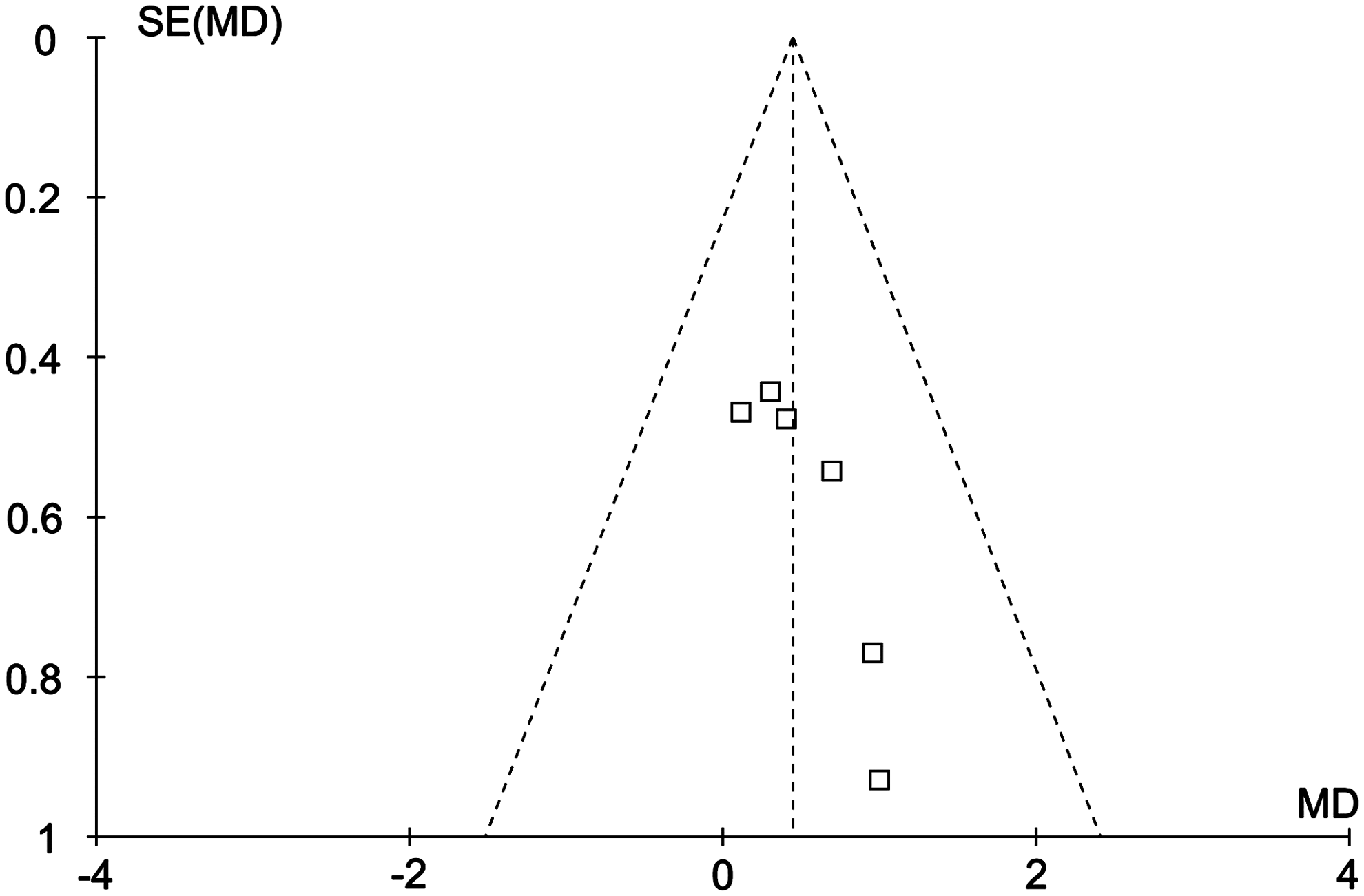
Funnel plot of the intraocular pressure reduction comparing the fixed combination brimonidine/timolol with the fixed combination dorzolamide/timolol.
Efficacy
Diurnal mean IOP
In all studies, FCBT (287 patients) and FCDT (268 patients) were administrated twice daily. Six trials involving 517 patients reported diurnal mean IOPR.
The point estimates of all 6 trials were distributed across the 1.0 odds ratio. There was no significant heterogeneity (P=0.88, I 2 =0%). FCBT was associated with numerically lower IOPRs relative to FCDT in diurnal mean.
The WMD of IOPR in diurnal mean was 0.44 mmHg (95% CI, 0.00–0.88) (Fig. 3), and there was no significant difference between FCBT and FCDT (P=0.05, test of overall effect).
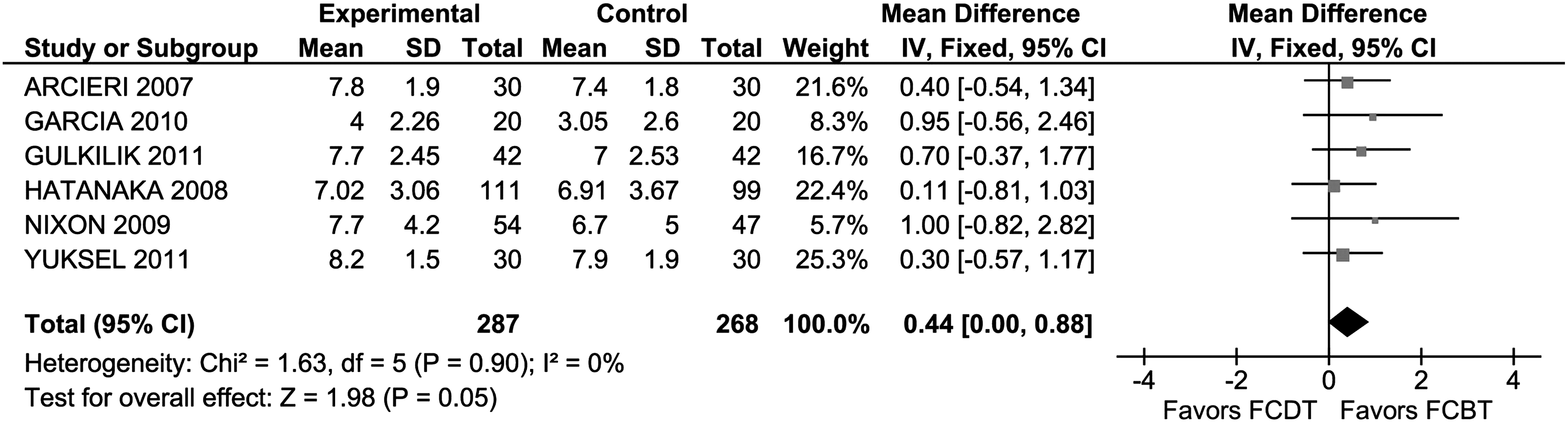
Forest plot of intraocular pressure reduction in diurnal mean.
Peak IOP
The reductions from baseline in peak IOP comparing FCBT with FCDT are shown in Fig. 4. All 6 trials had 95% CIs crossing 1.0.
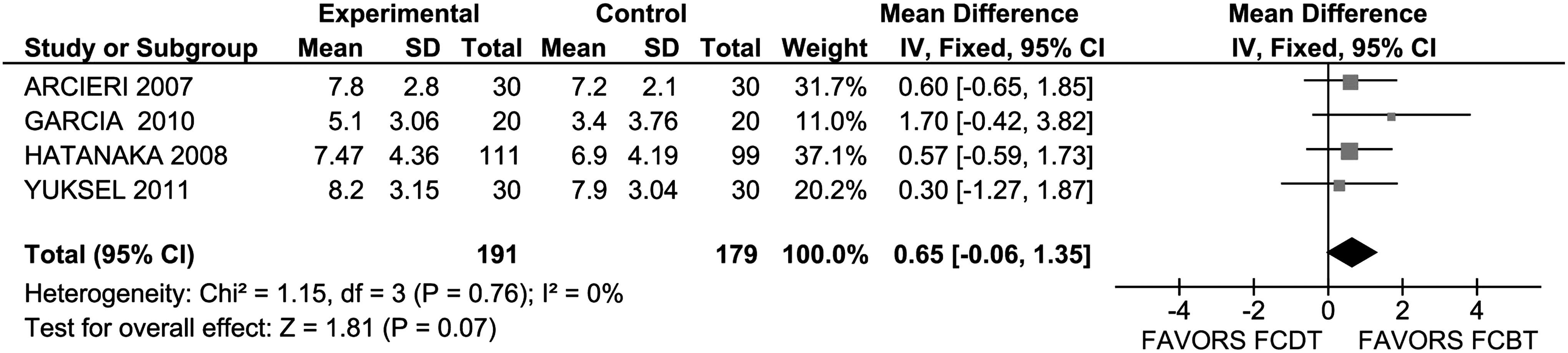
Forest plot of intraocular pressure reduction at peak moment.
There was no significant heterogeneity across studies (P=0.76, I2=0%). The WMD of IOPR was 0.65 mmHg (95% CI, −0.06 to 1.35). Although FCBT showed numerically lower IOPRs at peak when compared with FCDT, there was no significant difference between them (P=0.07, test of overall effect).
Tolerability
Across all studies, the adverse events reported were usually mild to moderate and resolved without treatment.
FCDT caused burning/stinging in more patients than the FCBT [pooled RR: 0.45 (95% CI, 0.29–0.70)] (Table 3). There were no significant differences between FCBT and FCDT in the incidence of any other reported adverse events such as allergy/pruritus, dry eye, conjunctival hyperemia, blurred vision, and tearing/secretion.
RR, relative risk; CI, confidence interval.
Discussion
Lowering IOP is beneficial in both POAG and ocular hypertension. A previous meta-analysis of RCTs revealed that an IOP-lowering strategy delays the progression of visual field deterioration. 21 Depending on the glaucomatous damage and the presence of other risk factors, the target IOP often has to be chosen such that IOP lowering beyond 30% or even 40% is necessary. 22 Medical therapy remains the cornerstone of glaucoma treatment. Hence, it is important to select the simplest treatment regimen that achieves the most effective IOP reduction. 9
In this present meta-analysis, we reviewed 7 RCTs comparing the FCBT with the FCDT in patients with elevated IOP, and found no significant difference regarding efficacy in lowering IOP at peak and diurnal mean. Both drugs contain timolol, a beta blocker, combined with either an alpha2 adrenergic agonist (brimonidine) or a carbonic anhydrase inhibitor (dorzolamide). A study comparing brimonidine 0.2% versus dorzolamide 2% found similar efficacy and safety between monotherapy treatment with brimonidine or dorzolamide when each was given 3 times daily to patients with ocular hypertension or POAG. 23 This suggests that brimonidine 0.2% and dorzolamide 2% behave similarly when used as monotherapy and as combined to timolol. Ventura et al. 24 stated that there are no marked differences in efficacy and safety of the 2 fixed combination medication and therefore proposed that cost should be considered in deciding which medication to prescribe since the most important factors influencing the choice of an initial agent are efficacy, tolerability, contraindications, safety, convenience of administration, and cost. 25
The tolerability was evaluated by calculating the proportion of subjects randomized to each class of medication who experienced each category of adverse event. Both FCBT and FCDT were well tolerated. There was only one specific category of adverse events in which significant difference in the frequencies of occurrence among the classes of therapies was observed: burning/stinging. These data are noted in the manufacturer's product labeling, which includes results from their original clinical studies and has also been reproduced in other large comparative trials where the incidences of drug-related ocular burning or stinging sensation with dorzolamide–timolol were higher than those with other ocular hypotensive medications. 26
Strengths and limitations of the meta-analysis
To demonstrate that the statistical analysis is robust, we scored the methodological quality of included randomized clinical trials. Only one study was of poor quality (Jadad score=2). When excluding this study, the results were similar. In an attempt to reduce publication bias, an extensive literature search in multiple databases and websites was conducted to retrieve all relevant eligible trials, and any language publications were included. In addition, we explored funnel plots to detect potential publication biases, and any evidence for such a bias was found.
However, the present study has limitations that stem from the designs of the individual trials and the methods of meta-analysis itself. One limitation of our systematic review is that our analyses were based on data pooled from trials of different durations. Some caution is therefore needed in their interpretation. Further, the short duration of included studies also limits the conclusion one may draw concerning the effects of FCBT and FCDT in the long-term treatment required in chronic glaucoma. A second limitation of this meta-analysis is that only published studies were included. Although multiple databases and websites were searched, unfortunately, it is possible that we may have failed to include some articles, especially those published in other languages. A third limitation of this meta-analysis is that our analysis did not evaluate the success rate and the response rate.
Recommendations for future research to inform clinical practice
Our systematic review data from 7 RCTs, which were undertaken in various countries, showed that there was large evidence to help deal with clinical importance regarding efficacy and tolerability of FCBT compared with FCDT in the treatment of elevated IOP. However, the lack of key comparative data such as the success rate and the response rate leaves doctors, commissioners, and the public confused about how to use such a new drug in relation to standard practice.
Further long-term studies are needed to evaluate the relative efficacy and tolerability of FCBT and FCDT in lowering IOP in patients with elevated IOP. Outcome data should include IOP reduction, IOP control, IOP response, and adverse events. Increasing the number of patients and increasing the follow-up period may produce results closer to what is actually experienced in practice.
Conclusion
In conclusion, the results of this meta-analysis including 7 randomized clinical trials suggest that both FCBT and FCDT can effectively lower IOP in patients with elevated IOP, and the IOP-lowering efficacy of FCBT is noninferior to that of FCDT. Lesser occurrence of burning/stinging sensation may improve patients' compliance with FCBT. Further clinical trials will help identify differences between the 2 fixed combinations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.