
Abstract
Abstract
Purpose:
To evaluate the impact of macular serous retinal detachment (SRD) and its relationship to treatment outcome after primary intravitreal bevacizumab (IVB) injection in patients with branch retinal vein occlusion (BRVO) and macular edema (ME).
Methods:
Seventy-three patients with ME secondary to BRVO who received primary IVB (2.5 mg/0.1 mL) were included in this study. The specific ME patterns were investigated using optical coherence tomography (OCT) examination. Visual acuity (VA), central macular thickness (CMT), and macular volume at baseline; at 1, 3, and 6 months; and at final visit after primary IVB were retrospectively analyzed and compared between patients with and without SRD.
Results:
SRD was found in 25 patients (34.2%). The baseline CMT was significantly thicker in patients with SRD than in those without it (648.4±200.5 μm vs. 440.3±119.6 μm, P<0.001). Six months after primary IVB injection, a greater reduction in CMT change from baseline was observed in the SRD group (412.5±227.2 μm) than in the group without SRD (118.5±175.2 μm) (P<0.001). The improvement of logarithm of the minimum angle of resolution VA was also greater in the SRD group than in the group without SRD (−0.64±0.52 and −0.28±0.62 respectively, P=0.015). Logistic regression analysis showed that the presence of SRD was an independent factor for visual improvement in BRVO (P=0.027).
Conclusion:
Patients with SRD had greater functional and morphological improvements at 6 months after primary IVB therapy. The results of this study suggest that the presence of SRD observed on OCT may be an indicator of favorable clinical response after IVB injections and that in BRVO patients with SRD, bevacizumab may be a good alternative for treatment.
Introduction
In recent years, anti-vascular endothelial growth factor (VEGF) agent bevacizumab has been increasingly used for BRVO patients. Numerous studies have reported that it efficiently reduced ME in BRVO.4–7 However, since not all eyes follow an optimal course after bevacizumab treatments, efforts were made to identify relevant prognostic indicators.8–11 A large retrospective study conducted by the Retinal Vein Occlusion Study Group identified baseline visual acuity (VA), age, and duration of BRVO to be of prognostic relevance for visual improvement after bevacizumab therapy. 9 Hoeh et al. reported that BRVO patients with CME and larger cystic spaces, greater than 600 μm on OCT, were associated with poor functional response after treatment. 10 Preoperative presence of macular ischemia has also been reported as a predictor of treatment outcome. 11
In diabetic ME, a positive correlation between OCT ME patterns and clinical response after bevacizumab therapy was recently reported. 12 However, the issue of whether the presence of macular SRD on OCT is predictive of treatment outcome after intravitreal bevacizumab (IVB) treatment in BRVO patients with ME has not been previously addressed. Therefore, the aim of this study is to evaluate the impact and relationship of SRD to treatment outcome after primary IVB treatment in BRVO patients.
Methods
Seventy-three patients (37 women, 36 men; 73 eyes) with ME secondary to BRVO who received IVB treatment at the retina service of a single tertiary referral center in Kaohsiung, Taiwan, between January 2008 and December 2010 were enrolled in this study. The medical records of the patients were retrospectively analyzed. This study was carried out in adherence to the tenets of the Declaration of Helsinki, and was approved by the institutional review board of the Kaohsiung Chang Gung Memorial Hospital.
Main inclusion criteria for this study were the presence of SRD and/or CME documented by OCT with ME involving the center of the fovea with a minimum of central macular thickness (CMT) at a baseline of≥250 μm. All patients were naïve to treatment. The exclusion criteria were as follows: (1) a previous intravitreal injection of triamcinolone acetonide or anti-VEGF agents; (2) previous macular laser photocoagulation treatment; (3) previous ocular surgery within 6 months; and (4) severe intraretinal hemorrhage that preclude accurate acquisition and interpretation of OCT images.
At baseline, all patients underwent a comprehensive ophthalmologic examination, including measurement of best-corrected VA on Landolt C ring chart, intraocular pressure (IOP) measurement, slit-lamp biomicroscopy, dilated fundus examination with indirect ophthalmoscopy, and OCT examination, with or without fluorescein angiography (FA).
OCT images were obtained using the third-generation OCT (OCT-3; Model 3000; Carl-Zeiss Meditec). The fundi were scanned with a measurement beam on the 6 radial planes crossing the central fovea. A scan length of 6 mm was used for all eyes. CMT and macular volume were measured and obtained using the Fast Macular Thickness Map analysis protocol on OCT. CMT represents the average retinal thickness of the central 1 mm of the macula. Macular volume represents the sum of the volumes of the retina in the central 6 mm of the macula. The classification of CME or SRD was based on the definitions by Spaide and coworkers. 2 CME was defined by the presence of hyporeflective intraretinal cavities on the cross-sectional scans (Fig. 1A). SRD was defined by an elevation of the posterior surface of the retina above the retinal pigment epithelium on OCT (Fig. 1B). Patients were separated into 2 groups according to the presence or absence of SRD on OCT.
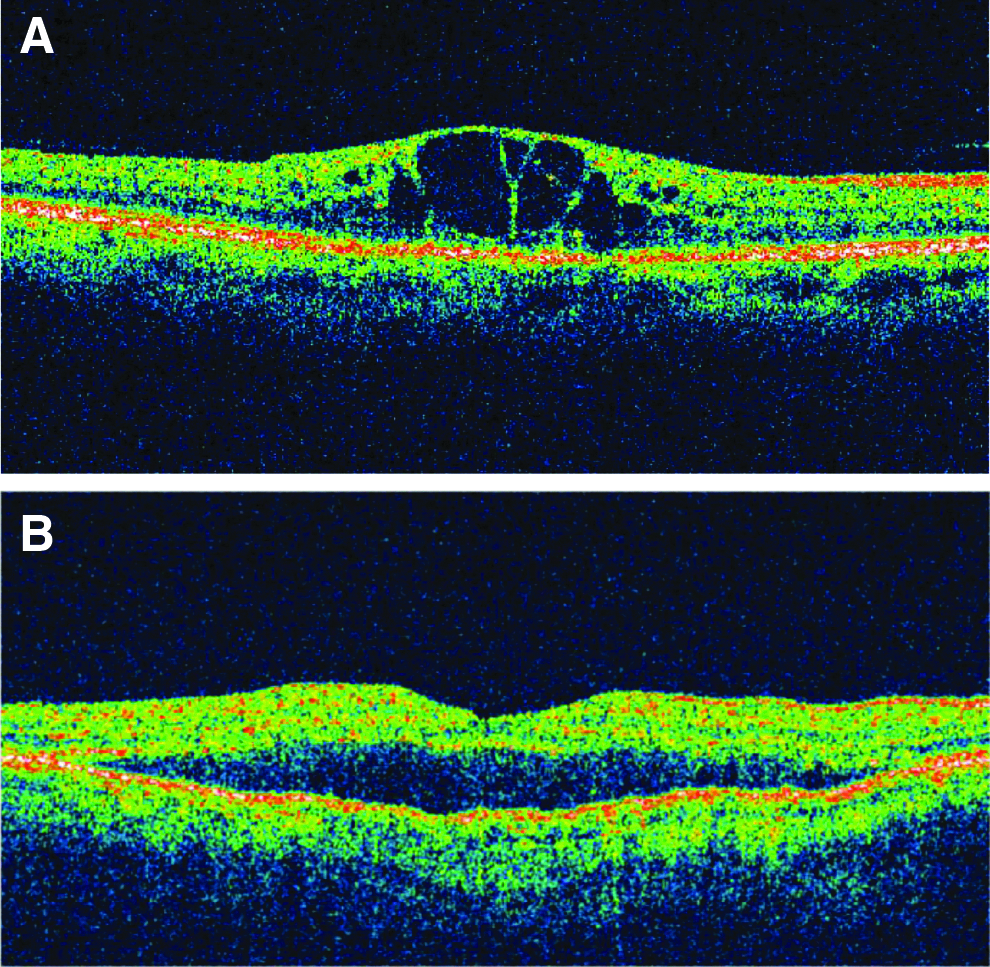
Optical coherence tomography cross-sectional scans demonstrating
Written informed consent was obtained before treatment, and patients were informed regarding the off-label use of bevacizumab and its potential side-effects. Intravitreal injections were administered under sterile conditions. Patients received 2.5 mg/0.1 mL of bevacizumab (Avastin; Genetech, Inc.) using the standard protocol of the Kaoshiung Chang Gung Memorial Hospital. In the surgery room, topical anesthesia was applied; povidone–iodine 5% eye drops were applied several times; and a sterile lid speculum was placed over the eye. After anterior paracentesis had been performed to avoid drug reflex during injection and to prevent elevation of IOP, bevacizumab was injected into the vitreous cavity using a 27-gauge needle at 3.5 and 4.0 mm posterior to the limbus in pseudophakic and phakic eyes, respectively. After IVB, vision was checked immediately to confirm retinal perfusion; this required VA that was sufficient to detect at least hand movements. Immediately after this, tobramycin–dexamethasone ointment (Tobradex™; Alcon, Inc.) was applied.
Reinjections were performed on an “as-needed” basis. Criteria for the reinjection of bevacizumab included morphologically evident intraretinal edema or subretinal fluid on OCT, persistent edema with a CMT of ≥250 μm, recurrent ME with an increase of CMT≥50 μm to the values obtained from the previous examination period, or a subjective decrease in VA from the previous follow-up visit.
Focal pattern macular grid laser treatments were used as an adjunctive therapy for ME unresponsive to at least 2 to 3 bevacizumab injections. Scatter laser photocoagulation was performed in the retinal quadrant involved by BRVO if neovascularization was noted, or when evidence of ischemia was observed on FA.
Main outcome measures were changes in VA, CMT, and macular volume from baseline to the final visit. Patient data were examined at baseline; at 1, 3, and 6 months; and at the final visit after primary IVB. Recurrent ME after primary treatment was defined as an increase in CMT greater than 50 μm than the values obtained from the previous examination period. VA data were converted to the logarithm of minimum angle of resolution (logMAR) scale for statistical comparison.
Statistical analyses were performed using SPSS software v. 17.0 (SPSS, Inc.). Continuous variables were analyzed with the student's t-test, and categorical variables were analyzed with the chi-square test. A comparison of treatment response before and after bevacizumab injection was analyzed with the paired t-test. Independent variables relevant to prognosis were identified using a multivariate analysis by stepwise logistic regression. The level of statistical significance was set at P<0.05.
Results
The mean age of the 73 patients enrolled in this study was 63.01±10.36 years, (range, 42 to 86 years) and the mean follow-up time was 19.85±11.54 months (range, 6 to 48 months). The mean duration of symptoms before receiving treatment was 6.74±8.45 weeks (range, 3 to 48 weeks). At baseline, 25 patients (34.2%) had SRD, and 48 patients (65.8%) had CME alone without SRD. In this study population, the baseline mean logMAR VA was 1.29±0.59, baseline CMT was 551.53±180.64 μm, and macular volume was 10.90±2.86 mm3.
The clinical characteristics of the patients in the 2 comparison groups are summarized in Table 1. The mean age, gender, presence of hypertension, diabetes mellitus (DM), duration of symptoms, and baseline VA were not significantly different between the 2 groups. However, the SRD group presented with a significantly greater mean CMT (648.4±200.5 μm, P<0.001) and macular volume (13.00±3.42 mm3, P<0.001) than the group without SRD (440.3±119.6 μm and 9.82±1.73 mm3, respectively) at baseline.
SRD, serous retinal detachment; SD, standard deviation; logMAR VA, logarithm of minimum angle of resolution visual acuity; CMT, central macular thickness. (Bold values indicate statistically significant p-value).
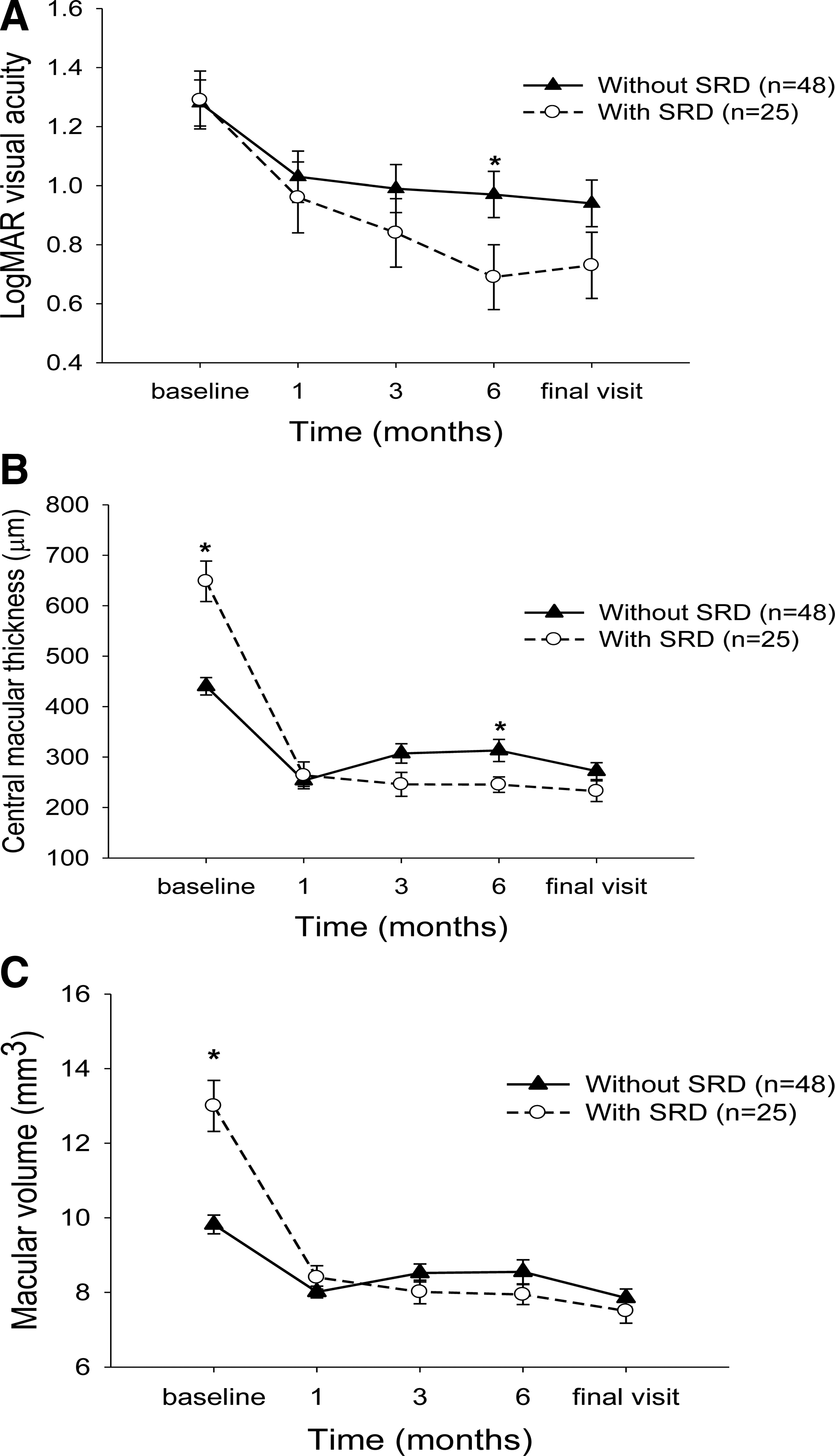
When analyzing the treatment outcomes of the individual groups, both groups had significant improvements in VA and in the OCT parameters at all time points compared with baseline (P<0.01) (Table 2). However, when comparing between the groups, at 6 months after treatment, the SRD group had significantly better VA (P=0.043) (Fig. 2A), a greater amplitude of VA improvement (P=0.033) (Table 3), and lesser CMT (P=0.013) (Fig. 2B). At the final follow-up, there were no statistical differences in all 3 outcome measures between the 2 groups (logMAR VA: P=0.129; CMT: P=0.151; macular volume: P=0.392).
MV, macular volume.
The amount of improvement in VA when compared with baseline in the group with SRD was significantly greater than in the group without SRD at 6 months. (Bold value indicates statistically significant p value).
Reinjections of bevacizumab were administered if ME persisted or recurred. Recurrent ME after primary IVB was more common in the group without SRD than in the group with SRD at 3 months (66.7% and 40.0%, P=0.029, respectively) (Table 4). However, there was no difference in the number of bevacizumab reinjections between the group with SRD (2.36±1.29, mean±SD) and the group without SRD (2.13±0.84, mean±SD) (P=0.415). Four patients (8.3%) in the group without SRD and 2 patients (8.0%) in the group with SRD (P=0.961) received additional intravitreal triamcinolone acetonide injections. Laser treatment was performed for 12 patients (25%) in the group without SRD, and for 11 patients (44%) in the group with SRD (P=0.097). In patients in the SRD group who received laser treatment, 6 out of 11 patients (54.5%) received laser treatment for more than 6 months after primary IVB; while in the group without SRD, 4 out of 12 patients (33.3%) received laser treatment at 6 months after primary IVB (P=0.414).
Bold value indicates statistically significant p value.
Multivariate analysis revealed that the presence of SRD at baseline (odds ratio, 3.33; 95% confidence interval 1.14–9.72, P=0.027) and the baseline logMAR VA (odds ratio, 4.043; 95% confidence interval 1.43–11.41, P=0.008) were independent factors for visual improvement by at least 0.4 logMAR (median value of improvement in VA of our study) from baseline to the last visit. Other variables, including age, sex, hypertension, DM, baseline CMT, and baseline macular volume, were not independent factors associated with visual improvement at the final visit (Table 5).
CI, confidence interval. (Bold values indicate statistically significant p value).
Discussion
In ME secondary to BRVO, CME is its most common presentation. SRD was previously thought to occur infrequently. 13 However, using OCT, recent studies have shown that SRD is a more common presentation in BRVO than has been previously recognized.2,3,14
Our study results showed that after primary bevacizumab treatment, both patients with and without SRD had significant improvements in VA compared with baseline (Table 2). However, a greater amount of VA improvement was observed in the patients with SRD than in the patients without SRD, especially at 6 months after treatment. Similarly, although an improvement of CMT was observed in both groups, the amount of reduction in macular thickness was greater in the SRD group, and this difference reached statistical significance at 6 months. In other words, our results suggest that in patients with ME caused by BRVO, both CME and SRD respond favorably to bevacizumab therapy; however, the amount of improvement is greater in patients with SRD.
Untreated SRD in BRVO has previously been associated with a poor visual prognosis.3,15 However, Noma et al. 16 used microperimetry to show that SRD itself does not influence macular sensitivity, and that SRD does not necessarily lead to a poor visual prognosis in BRVO patients. 17 The initial visual impairment may be related to the mechanical photoreceptor cell damage caused by the retinal detachment, and may be reversible after SRD resolves. 17 Our study results support the findings that after resolution of SRD, the visual prognosis of these patients is better than what was previously thought. Our findings suggest that once normal retinal architecture is promptly restored after bevacizumab therapy, visual potential may be retained in these patients.
In retinal vein occlusion, venous stasis leads to capillary nonperfusion and tissue ischemia, and can result in disruption of the blood-retinal barrier (BRB) function. 18 The development of SRD in hypoxic retina had been associated with an increased production of inflammatory mediators in response to hypoxia and ischemia,17,18 which then leads to increased vascular permeability and leakage across the outer BRB formed by the retinal pigment epithelial (RPE) layer. Extracellular fluid then accumulates in the subretinal space as a result of the transudation of plasma proteins and osmolytes leaked from blood vessels crossing the outer BRB. 19 VEGF is an important angiogenic factor that causes an increase in vascular permeability and is up-regulated in the hypoxic retina. 18 Noma et al. had previously shown that the level of VEGF and other inflammatory mediators, such as intercellular adhesion molecule-1, were significantly higher in BRVO patients with SRD than in those with CME, and suggested that this markedly higher level of vitreous inflammatory factors contributed to the formation of SRD. 17 Although the exact mechanism by which VEGF increases vascular permeability is currently unknown, 18 it appears that after stimulation by excessive VEGF, fluid transportation across the RPE layer may be altered, which can be counteracted by the administration of an anti-VEGF agent.
A VEGF antagonism for the treatment of ME secondary to BRVO has been widely studied, demonstrating effective post-treatment reduction of VEGF below detectable levels, 20 reduced ME, and improved VA.4–7,21,22 However, a few studies have addressed the differences in treatment outcome in response to bevacizumab between the 2 morphological patterns, CME and SRD, both of which can occur in BRVO. The use of macular grid laser and intravitreal triamcinolone acetonide for the management of BRVO with SRD has been previously reported.15,23 Recently, a study by Cinal et al. investigated the treatment outcome of SRD in central retinal vein occlusion after IVB therapy; a significant improvement in the vision and resolution of ME was observed after treatment. 24 However, the results of their study are limited by the absence of a comparison group. Our study is the first that specifically investigates and compares the treatment outcomes of bevacizumab between BRVO patients with SRD and those without SRD.
Since the inner BRB is more prone to hypoxic injuries than the outer BRB, 18 we speculate that this may be the cause of the differential response between SRD and non-SRD patients who were observed in this study. Under hypoxic conditions, the tight junctions between endothelial cells, which constitute the inner BRB, open up and become separated; while at the outer BRB, the intercellular spaces between the RPE cells widen, but the tight junctions remain intact. 18 Therefore, we speculate that the integrity and preservation of the RPE tight junctions in the outer BRB during hypoxia may play a role in the more favorable clinical response that were observed in SRD patients.
In previous OCT studies, distinct morphological patterns of ME were appreciated2,3; however, the mechanism by which a diversity of ME morphological patterns occurs after retinal vein occlusion is still not well understood. In a recent study, Murakami and coworkers showed that intraretinal cystic edema in BRVO patients was associated with macular ischemia or fusiform/aneurysmal dilation of the perifoveal capillaries. 25 BRVO patients with SRD, on the other hand, more often had perfused macula and fine perifoveal capillary plexus. 25 However, since FA was not performed in all patients in this study, we are unable to confirm this finding in our patients with SRD.
The extent of ischemia may also have an impact on the therapeutic outcome.9,11 As shown by Chung et al., the presence of macular ischemia may be a poor prognostic factor for visual improvement. 11 However, in contrast to this report, in a more recent study, the Retinal Vein Occlusion Study Group demonstrated that even with the presence of macular ischemia, it can still be associated with a favorable visual outcome after bevacizumab therapy. 9 Since FA was not performed in all of our patients in this study, we were unable to evaluate the influence of ischemia status on treatment outcome.
The Branch Vein Occlusion study previously demonstrated that grid pattern laser treatments effectively reduced ME secondary to BRVO. 26 In BRVO patients with SRD, macular grid laser treatments were also shown to be effective in reducing macular thickness and preventing VA deterioration. 15 Ohashi and coworkers previously showed that the presence of SRD delays the absorption of ME and the recovery of VA after grid laser in patients with BRVO. 27 However, in contrast to the slower recovery course after macular grid laser in BRVO patients with SRD, in this study, we found that after IVB, the recovery course may be better in SRD patients, because the amount of improvement was greater in patients with SRD than in those without SRD, especially at 6 months after primary IVB. Although the number of patients who ultimately received laser treatment was slightly higher in the SRD group (44%) than in the group without SRD (25%), however, the proportion of patients who received laser treatment was not statistically different between the 2 groups (P=0.097). Furthermore, since in the SRD group, more than half of the laser cases (54.4%) were performed at least 6 months after primary IVB, we believe that it probably would not affect our results. However, even though in our study, we showed that a greater amount of morphological and functional improvement after IVB was achieved in the SRD group, it is possible that laser treatment may still be needed for long-term stabilization in cases of BRVO with SRD.
Major limitations of this study include its retrospective design, small sample size of the subgroups, and inconsistent criteria for reinjection of bevacizumab and laser treatments among patients. The inclusion of DM cases in this study may also potentially confound our results, because DM can cause retinal microangiopathy and result in abnormal vascular permeability, 19 which may also affect treatment outcomes. However, patients with severe nonproliferative diabetic retinopathy, proliferative diabetic retinopathy, and diabetic maculopathy were not included in this study; thus, the influence of diabetic microangiopathy on our results should be less significant in our patients. Further prospective studies with a larger sample size, a standardized reinjection, and laser protocols will be needed to clarify the role of SRD in BRVO and the individual morphological ME patterns and their effects on long-term prognosis and treatment outcomes.
In conclusion, our study shows that IVB injections can rapidly and effectively reduce ME in BRVO. However, both morphological and functional improvements were significantly greater in patients presenting with SRD, especially at 6 months after primary bevacizumab treatment. Therefore, in BRVO patients with SRD, bevacizumab may be considered a good alternative for treatment.
Footnotes
Author Disclosure Statement
The authors have no financial interest or conflict in the material discussed in this article.