
Abstract
Abstract
Purpose:
Demonstrate that the blockade of angiotensin II AT-1 receptors, through the systemic administration of olmesartan, can reduce the MCP-1 expression and the resulting macrophage accumulation in the choroid and sclera of hypercholesterolemic rabbits.
Methods:
Thirty-two New Zealand rabbits were divided into 3 groups: group I (GI) was fed a standard rabbit diet; group II (GII) was fed a hypercholesterolemic diet; and group III (GIII) was fed a hypercholesterolemic diet plus olmesartan. Serum levels of total cholesterol, triglyceride, HDL cholesterol, and blood glucose were determined in fasting rabbits at the beginning of the experiment and on the day of euthanasia. The choroid and sclera were submitted to morphometric analysis as well as immunohistochemical analysis with MCP-1 and RAM-11 (macrophage marker) antibodies.
Results:
No abnormality was detected in GI. Group II and III had significant increases in choroid–sclera complex thicknesses when compared with group I (P<0.001). GII showed a significant increase in immunoreactivity for MCP-1 in relation to GI (P=0.001) and GIII (P=0.004). GII showed a significant increase in immunoreactivity for RAM-11 of the choroid–sclera complex in relation to GI (P<0.001) and GIII (P=0.034). A significant increase in immunoreactivity for RAM-11 was observed in GIII in relation to GI (P=0.008).
Conclusion:
Olmesartan reduced the MCP-1 expression and the resultant macrophage accumulation in the choroid–sclera complex of hypercholesterolemic rabbits.
Introduction
The objective of this study is to determine whether the blockade of angiotensin II AT-1 receptors, induced by olmesartan, can decrease the leukocyte recruitment in the choroid–sclera complex of hypercholesterolemic rabbits.
Methods
Experimentation environment
The procedures described in this study were performed at the Surgical Technique Laboratory at PUC-PR and the Study Center of the Angelina Caron Hospital. The animals were kept in an animal facility (macroenvironment) on 12-h dark/12-h light cycles, with air changes and room temperature controlled between 19°C to 23°C. During the experiment, they were fed water and standard Nuvital® rabbit chow (Nuvital) ad libitum.
Animals used and experiment design
Thirty-two white adult male rabbits (New Zealand), with a mean age of 3.7 months, were selected for this study. Animals were handled in compliance with the principles established by the Association for Research in Vision and Ophthalmology (ARVO), and the protocol was approved by the Pontifical Catholic University Animal Research Committee. The animals were divided into 3 groups: group I (GI), the normal group, 8 rabbits; group II (GII), the hypercholesterolemic group, 13 rabbits; group III (GIII), the olmesartan-treated hypercholesterolemic group, 11 rabbits. During the 56-day study, the animals in GII and GIII were fed a specific diet: Nuvital Lab (Nuvital) plus 1% cholesterol (Sigma-Aldrich®). The daily amount of food per animal was 600 g. 15 The diet, Nuvital Lab (Nuvital), does not alter lipid metabolism in the animals. In GIII diet, 1 mg/kg/day of olmesartan (commercially available from Sankio) was administered by oral gavage from day 1 through day 56. On day 56, the animals from GII and GIII were euthanized. Animals from GI were fed only Nuvital Lab chow and were euthanized on day 28. Serum levels of total cholesterol, triglycerides, HDL cholesterol, and glucose were determined in fasting rabbits at the beginning of the experiment and the time of euthanasia. Euthanasia was carried out by endovenous anesthesia with 5 mL of pentobarbital, and the rabbit eyes were immediately placed in 4% paraformaldehyde (Merck), in 0.1 M phosphate, pH 7.4, for 4 h, for the choroid–sclera complex morphometry and immunohistochemical analysis.
Tissue preparation
After fixation, the samples were evaluated macroscopically. A coronal section at the level of the optic nerve was performed, and the ocular globe was divided into 2 equal halves. The lower half was stored for future study; the upper half underwent dehydration, diaphanization, and was embedded in paraffin using a Leica® TP 1020–Automatic Tissue Processor (Leica). A Leica EG1160 paraffin-embedding device was used to produce the paraffin blocks. The Leica RM2145 Microtome was used to obtain 5-micron-thick sections for histology. The sections were placed on glass slides smeared with albumin, stained with hematoxylin–eosin and mounted with 24×900-mm coverslips, using Entellan Mounting Media (Merck).
Choroid–sclera complex morphometry
For the quantitative analysis, the evaluated sections were stained with hematoxylin–eosin. With the aid of a 4×objective lens and a blue overhead projector marker, the hemisectioned ocular globe was divided manually into 10 equal segments (from the pars plana to the contralateral pars plana). Segment images were obtained (10 images of each eye) using an Olympus BX50 microscope (Olympus) connected to a Sony camera BX50 (Sony Corporation). In each captured image, 4 linear morphometric measurements were performed, using the Image-Pro plus® software BX50 (Media Cybernetics, Inc.) that obtained 40 measurements in each eye to evaluate the choroidal and scleral thicknesses. Finally, the mean of the 4 measurements of each of the 10 segments was obtained. The result is expressed in micrometers.
Tissue preparation and immunohistochemical analysis
The histological slices were submitted to blockage of endogenous peroxidase. They were then washed in deionized water and incubated in a moist chamber at 95°C for 20 min for antigen retrieval. Afterward, endogenous peroxidase was again blocked. The slices were incubated with the primary polyclonal antibody anti-MCP-1 at a 1/400 dilution (Imuny Biotechnology) and with the primary monoclonal antibody RAM-11 (a macrophage tissue marker) at a 1/400 dilution (DakoCytomation). Next, the slices were incubated with a secondary antibody, Envision® System labeled polymer-HRP anti-mouse (DakoCytomation) at room temperature for 30 min. They were then stained by dripping a freshly prepared DAB substrate (DakoCytomation) and once more incubated for 3 to 5 min. The slides were counterstained with Mayer hematoxylin and mounted.
Positive and negative controls were used in all evaluations, and the slides were initially analyzed by a masked observer. In this analysis, positive and negative results for the markers detected by anti-MCP-1 and RAM-11 were recorded. The positive areas acquired a brownish color and were studied utilizing color morphometry. This procedure was performed by capturing images of 3 consecutive fields, close to the optic nerve head, with a B×50 Olympus microscope coupled to a Sony camera, Model DXC-107A, using a 40×objective. The computer program Image-Pro Plus used enabled the observer to select and color the positive areas and automatically determined the immunoreactive area in square micrometers. The data obtained were compiled in a Microsoft Excel spreadsheet for statistical analysis. The variable immunoreactive area represents the sum of all positive areas in each of the 3 fields studied. This color morphometry method has already been used in other studies.16,17
Statistical analysis
To compare the defined groups for treatment in relation to the quantitative variables, a single factor analysis of variances was selected. Multiple comparisons were made with the least significant difference test. The baseline and euthanasia time evaluations within each group were analyzed using the Student's t-test for paired samples. Normality was assessed with the Shapiro–Wilk test. Logarithmic transformation was performed for variables showing skewed data. Values of P<0.05 indicated statistical significance. Statistica v. 8.0 was used for data processing.
Results
Blood sample analyses
At baseline, there was no significant difference in the laboratory variables of the animals, within the same group and between groups. The rabbits did not show significant alterations in the glycemic and HDL values at the time of euthanasia. Conversely, total cholesterol, which at baseline was about 47 mg/dL, reached at the time of euthanasia 2200.00 mg/dL in groups II and III, revealing thus, a significant increase in relation to GI (P<0.001). The baseline value for triglyceride was 60 mg/dL and increased at the end of the experiment to 203 mg/dL in GII and GIII, revealing thus, a significant increase in relation to GI (P<0.001).
Choroid–sclera complex morphometry
Group II and III had a significant increase in the choroid–sclera complex thickness if compared to Group I (P<0.001) (Table 1).
ANOVA, P<0.05
GI versus GII: P<0.001; GI versus GIII: P<0.001; GII versus GIII: P=0.293.
GI, normal diet group; GII, cholesterol-enriched diet group; GIII, cholesterol- and olmesartan-enriched diet group.
Immunoreactivity for MCP-1
The hypercholesterolemic group (GII) showed a significant increase in MCP-1 immunoreactivity in relation to the GI (P=0.001) and GIII (P=0.004) groups. There was no statistical difference between GIII and GI (P=0.307) (Table 2).
ANOVA, P<0.05.
GI versus GII: P=0.001; GI versus GIII: P=0.307; GII versus GIII: P=0.004.
The choroid–sclera complex of GI exhibited a bluish color, revealing low MCP-1 immunoreactivity (Fig. 1.1). Figure 1.2 shows that the GII choroid–sclera complex exhibited marked immunoreactivity, identified by the orange coloration. Figure 1.3 shows that the choroid–sclera complex in GIII had a higher MCP-1 immunoreactivity than in GI and lower than in GII. Figure 1 also demonstrates the difference in thickness of the choroid–sclera complex among the groups. GII and GIII showed a significant increase in choroid and sclera thickness in relation to GI.
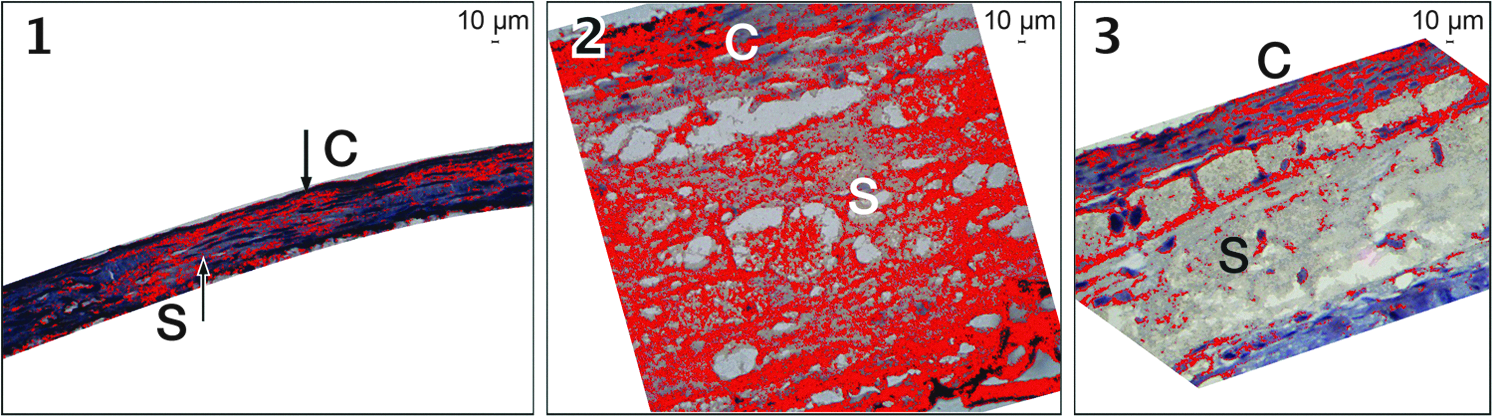
Immunohistochemistry with the MCP-1 antibody.
Immunoreactivity for RAM-11 (macrophage marker)
The hypercholesterolemic group (GII) exhibited a significant increase in RAM-11 immunoreactivity of the choroid and sclera in relation to GI (P<0.001) and to GIII (P=0.034). Conversely, GIII showed a significantly higher immunoreactivity in relation to GI (P=0.008) (Table 3).
ANOVA, P<0.05.
GI versus GII: P<0.001; GI versus GIII: P=0.008; GII versus GIII: P=0.034
The choroid–sclera complex of GI animals stained predominantly blue, revealing a low level of MCP-1 immunoreactivity (Fig. 2.1). Conversely, Fig. 2.2 shows that the choroid–sclera complex of GII animals is predominantly orange in color, revealing a high level of immunoreactivity. Figure 2.3, representing the GIII choroid–sclera complex, shows an immunoreactivity level for MCP-1 higher than in GI (Fig. 2.1) and lower than in GII (Fig. 2.2).
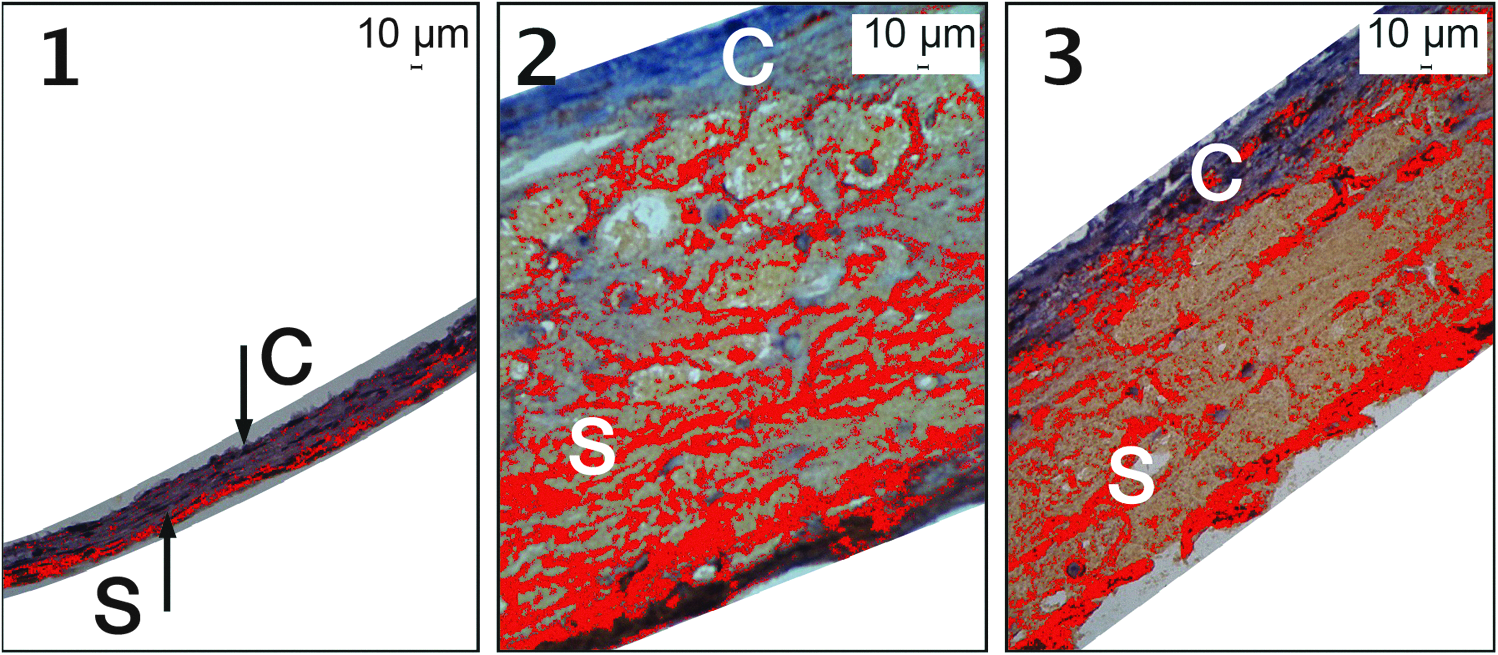
Immunohistochemistry with the RAM-11 antibody.
Discussion
In the present study, rabbits were fed a cholesterol-enriched diet with the objective of determining the effect of olmesartan on MCP-1 expression and the resulting macrophage accumulation in the choroid–sclera complex. As occurs in the great vessels,10,18,19 dyslipidemia induced a significant increase in MCP-1 expression in the choroid–sclera complex of the animals on the cholesterol-enriched diet (Table 2). MCP-1 is a chemotactic cytokine of low molecular weight (8–10 kDa), which is involved in monocyte recruitment to the inflammation site.20–22 Although MCP-1 is not expressed in normal vessels, several stimuli, particularly in response to lipid oxidation, may induce the release of inflammatory cytokines. These cytokines promote secretion of MCP-1 by cells of the endothelium, vascular smooth muscle and retinal pigment epithelium (RPE), which in turn promotes leukocyte recruitment and perpetuation of the inflammatory responses.21–25 Considering that hypercholesterolemia is a contributing factor of ARMD 26 and that cytokines, enzymes, and growth factors responsible for the atheromatous plaque may also affect the genesis of the degenerative macular disease,4–7 it is expected that MCP-1 has a similar action in the choroidal vessels.
In this study, when inducing hypercholesterolemia, we attempted to create a physiopathologic condition similar to ARMD, that is, the accumulation of lipids in the Bruch's membrane, which attract macrophages with the objective to absorb oxidized LDL. It is important to stress that, independent of the increase in serum cholesterol, RPE is a continuous production source of lipid and cholesterol esters and oxidized lipids are found in the initial phase of ARMD.27,28 The oxidized lipids stimulate the expression of chemotactic factors, such as IL-8 and MCP-1, by the RPE cells, which promote macrophage recruitment. 29 Hence, the increase in the MCP-1 expression in the choroid and sclera of hypercholesterolemic animals may have contributed for the increase in the macrophage concentration significantly (Table 3), accounting for the thickness of the choroid–sclera complex observed in this (Table 1) and in other studies.8,9
As ARMD and atherosclerosis display similar physiopathologic mechanisms,2–7,10–12 it is expected that the drugs used to treat these diseases present equivalent effects and characteristics. The addition of olmesartan to the hypercholesterolemic diet aimed to evaluate the effect of angiotensin II AT-1 receptors blockade on MCP-1 and the resulting macrophage accumulation in the choroid–sclera complex. Olmesartan medoxomil is a potent and a highly selective angiotensin II AT1 receptor antagonist, with proven effectiveness in blood pressure reduction. 30 It has been experimentally demonstrated that olmesartan induces a decrease in macrophages, monocytes, and T lymphocytes in the atheromatous plaque. 31 In the present study, the blockade of the angiotensin II AT1 receptor with an olmesartan-supplemented cholesterol-enriched diet, significantly reduced MCP-1 expression in the choroid and sclera, compared to the hypercholesterolemic diet only (P=0.004) (Table 2). It has already been demonstrated that the blockade of the AT1 receptor inhibits the inflammatory markers and maintains endothelial integrity preventing monocytes from migrating into the arterial wall intima. 32 This finding, confirmed by the immunohistochemical analysis of RAM-11, has been reproduced in our study. The reduction in the MCP-1 expression, induced by olmesartan, resulted in a significant decrease in the macrophage density in the choroid–sclera complex of the olmesartan-supplemented diet group (GIII) in relation to the only hypercholesterolemic diet (GII) group (P=0.034) (Table 3).
Due to its important role in the pathologic processes that involve angiogenesis and inflammation,13,33–35 the angiotensin II receptor type 1 may become an attractive target for the treatment of ARMD. Experimental studies have demonstrated that the blockade of the angiotensin II AT1 receptor lowered the expression of macrophages and inflammatory markers in the RPE and choroid, significantly reducing the development of the subretinal neovascular membrane.13,14,36
Finally, a therapeutic approach to ARMD that aims to interfere with macrophage actions should be carefully considered. It is likely that, in the early phase of ARMD, macrophage neutralization may aggravate the disease condition, as there will be increased accumulation of debris, immunoglobulins, and complements. 37 In the late phase, the suppression of macrophages may be useful as it neutralizes the inflammatory cytokines, such as interleukins and TNF-alpha, enzymes, such as MMP-9 that degrade the basement membrane, and growth factors, such as VEGF that promote angiogenesis.4–7,12–14,36,37 Consequently, there is a need for further experiments to evaluate the effectiveness and safety of olmesartan in the treatment and/or prevention of ARMD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.