
Abstract
Abstract
Purpose:
To evaluate structural alterations of iris and pupil diameters (PDs) in patients using systemic α-1-adrenergic receptor antagonists (α-1ARAs), which are associated with intraoperative floppy iris syndrome (IFIS).
Methods:
Eighty-eight eyes of 49 male were evaluated prospectively. Patients were assigned to 2 different groups. Study group included 23 patients taking any systemic α-1ARAs treatment, and control group included 26 patients not taking any systemic α-1ARAs treatment. All patients underwent anterior segment optical coherence tomography to evaluate iris thickness at the dilator muscle region (DMR) and at the sphincter muscle region (SMR). The PD was measured using a computerized infrared pupillometer under scotopic and photopic illumination.
Results:
The study group included 46 eyes of 23 patients and the control group included 42 eyes of 26 patients. Most treated patients were on tamsulosin (16/23). Mean age was similar in the study and control groups (61.9±7.1 vs. 60.3±8, 2 years, nonsignificant). DMR (506.5±89.4 vs. 503.6±83.5 μm), SMR (507.8±78.1 vs. 522.1±96.4 μm) and the DMR/SMR ratio (1.0±0.15 vs. 0.99±0.23 μm) was similar in the study and control groups and these differences were nonsignificant. Scotopic PDs were also similar in both groups (3.99±1.11 vs. 3.74±1.35, nonsignificant). A significantly reduced photopic PD (2.89±0.55 vs. 3.62±0.64, P<0.001) and an increased scotopic/photopic PD (1.42±0.44 vs. 1.02±0.30, P<0.001) were found in the study group.
Conclusions:
Evaluating PD alterations might be more useful than evaluating iris structural alterations in predicting IFIS. There is still a need for a reliable method that will determine the possibility of IFIS.
Introduction
It has also been revealed that there is a strong association between IFIS and sympathetic α-1 adrenergic receptor antagonists (α-1ARAs) used in the treatment of benign prostatic hyperplasia.1,7–10 Although the exact distribution of α-1A receptor subtypes in the human iris smooth dilator muscle is not obvious, animal studies showed that α-1A is the dominant iris adrenoreceptor. 11 It has been hypothesized that α-1ARAs affect these receptors in the iris dilator muscle leading to irreversible atrophy. 12
There is no current method to predict in which patients using α-1ARAs will develop IFIS. Evaluation of iris structural alterations and pupil size behavior might be used in predicting IFIS predisposition in patients using systemic α-1ARAs.
We assessed the influence of various α1-ARAs on the iris structure by using anterior segment optical coherence tomography (OCT) and pupil diameters (PD) by using computerized infrared pupillometer.
Methods
Patients
We prospectively enrolled 49 male patients with current use of any systemic α-1ARAs and untreated controls. Age, type and time of using the systemic α-1ARAs, ocular history, and systemic diseases recorded. Exclusion criteria included, previous ocular surgery, history of ocular trauma, glaucoma, exfoliation syndrome, pigment dispersion syndrome, ocular signs or a history of uveitis, previous laser iridoplasty, use of eyedrops other than artificial tears and any other condition that could alter iris morphology (e.g., tumors, congenital anterior segment abnormalities, rubeosis). The study was performed with informed patient consent and conducted under a protocol approved by the local ethics committee and in accordance with the ethical standards stated in the 1964 Declaration of Helsinki.
Iris measurement
All patients underwent anterior segment imaging using cornea lens adapted OCT (Spectral OCT/SLO™ system, OTI Ophthalmic Technologies, Inc.). Cornea lens provides high-resolution spectral OCT imaging of the cornea and angle. This affordable add-on lens transforms the spectral OCT/SLO™ into a system capable of imaging both posterior and anterior segments. These systems can acquire more than 25,000 A-scans per second with a resolution of approximately 5 μm. A total of 5 high-quality images were taken horizontally through the center of the pupil under standardized lighting conditions (300 lux) for each eye by using AS-OCT. Iris thickness measurements were obtained from one of these images which was well-centered and showed the anatomical structures best. The iris thickness was measured from 2 main points adjusted to iris anatomy. The first measurement was at the midpoint between the scleral spur and pupil margin representing the dilator muscle region (DMR). The second point was 0.75 mm from the pupillary margin representing the sphincter muscle region (SMR) (Fig. 1).
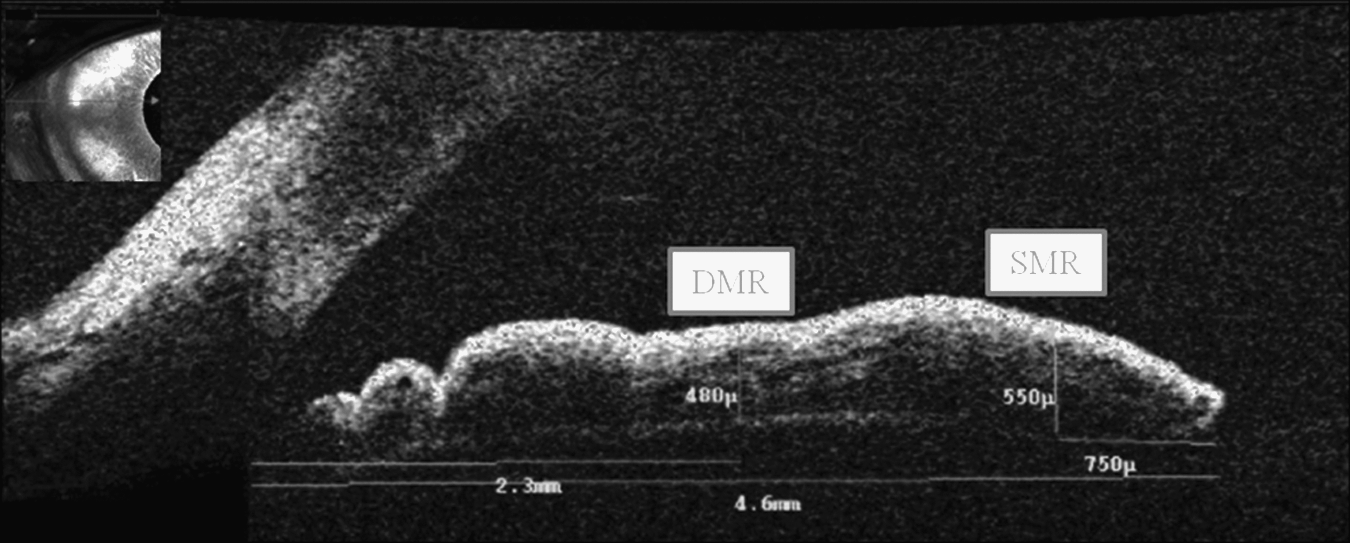
AS-OCT image demonstrating the standardized positions where iris thickness was measured. DMR, dilator muscle region (1/2 of total iris length); SMR, sphincter muscle region (750 μm away from pupiller margin); OCT, optical coherence tomography.
Pupil measurements
Pupil measurements were taken using a computerized infrared pupillometer (Sirius, Costruzione Strumenti Oftalmici) under scotopic (0.04 lux) and photopic illumination (40 lux). The ratio between the PD measured in the photopic/scotopic illumination was also calculated to compensate for possible intersubject variability.
Statistical analysis
Numerical variables between study and control groups were compared by using the Student's t test (or the Mann–Whitney U tests when variables are not distributed normally). A P-value of≤0.05 is considered significant.
Results
The study group included 46 eyes of 23 patients and the control group included 42 eyes of 26 patients. Most treated patients were on tamsulosin (16/23). Also, 4 patients were taking alfuzosin, 2 patients were taking terazosin, and 1 patient was taking doxazosin in the study group. There was no statistically significant difference in mean age between the study and control groups (61.9±7.1 vs. 60.3±8, 2 years). Both groups were similar according to the history of systemic diseases, such as congestive heart failure, diabetes, and hypertension. Patients in the study group had been treated with a systemic α-1ARAs between 6 and 120 months (median 36 months).
Table 1 shows the patients' characteristics, mean±SD values of iris and pupil measurements of both groups. There was no statistical difference in iris thickness in the DMR, SMR, and DMR/SMR ratio between groups. These values were 506.5±89.4 and 503.6±83.5 μm for DMR, 507.8±78.1 and 522.1±96.4 μm for SMR, and 1.0±0.15 and 0.99±0.23 μm for the DMR/SMR ratio in the study and the control group, respectively. None of these values was similar in the study and the control group and these differences were nonsignificant.
Univariate analysis of variance.
DMRT, dilator muscle region thickness; SMRT, sphincter muscle region thickness; PS, pupil size; NS, not significant.
Although there was no difference in scotopic PD, significantly reduced photopic PD values (2.89±0.55 vs. 3.62±0.64, P<0.001) and increased scotopic/photopic PD values (1.42±0.44 vs. 1.02±0.30, P<0.001) were found in the study group.
Discussion
Adequate pupil dilation and subsequent stability of the iris during surgery are the key factors for an uncomplicated cataract surgery. 13 Predicting IFIS before phacoemulsification becomes important as it can increase the risk for intraoperative and postoperative complications if not identified and managed early.2,8
Three recent studies investigated the effect of α-1ARAs on iris morphology. Prata et al. reported that patients using systemic α-1ARAs have significantly lower values of DMR thickness and the DMR/SMR ratio when compared to age-matched controls. However, it was impossible to make an inference about the effect of α-1ARAs on iris morphology as their study consisted of patients with glaucoma. 14 Reichenberger et al. had also measured the cross-sectional iris thickness by OCT in patients taking tamsulosin before cataract surgery and found reduced total iris thickness when compared with that in 41 controls. 15 There is only one study that evaluated iris pathology in patients taking tamsulosin histologically, showing that the thickness of the iris dilator muscle was normal in 16 cadaver eyes from study patients when compared with that in controls. 16 In contrast to these OCT studies, we showed that there is no difference in iris thickness in the DMR and SMR, which represents alterations in iris morphology. However, our results correlated with that cadaver study.
Our review of the literature revealed only 4 publications evaluating PD in patients taking α-1ARAs. The first study evaluated PD in patients treated with tamsulosin and alfuzosin over 6 months. They observed that PD decreased under mesopic and scotopic light after treatment with tamsulosin, but only scotopic PD decreased after treatment with alfuzosin. 17 However, Issa et al. reported that there was no significant difference in the mesopic and dilated PD between the 2 groups (tamsulosin and other α-1ARAs groups). 18 The third study assessed the pupil dynamics quantitatively (with digital pupillometer) in relation to the use of 1ARAs. 19 Their results showed a significant decrease in maximum PD in patients using α-1ARAs when compared with the control group. They also found a significant decrease in constriction velocity in these patients. Prata et al. also reported a smaller photopic PD in their patients when compared with controls. 14 In agreement with these studies, we showed a significant decrease in the photopic PD. However, we did not find a difference in the scotopic PD between the study and control groups. Finally, we found an increase in the scotopic/photopic PD ratio in the study group. We believe that the function of the pupil dilator and constrictor muscle could be evaluated by measuring the PD. Our finding might be important for the surgeon, who can consider it within the context of cataract surgery.
Chang and Campbell were the first who postulated that systemic tamsulosin blocked contraction of the iris dilator smooth muscle and that led to muscle tone deficiency. 1 Although multiple factors affect pupil functionality, we postulate that our results may be associated with the iris dilatator smooth muscle tone deficiency. We do not have an explanation why the pupil sizes are similar in both groups under scotopic condition in contrast to previous studies. This may be due to the complexity of the iris biology. For instance, advanced age and systemic diseases associated with endothelial dysregulation (e.g., congestive heart failure, diabetes, and hypertension) may affect the iris morphology and pupil size. 20
This study is prospective and has an acceptable sample size compared with other similar studies. Although there is no reported literature regarding how iris measurements with anterior segment OCT would represent the real iris thickness, we presumably eliminate this limitation by using the same device at the same position.
In conclusion, this study demostrated that α-1ARAs, in particular, tamsulosin, do not change the iris structure on anterior segment OCT. We also observed a significant decrease in the photopic PD and an increase in the scotopic/photopic PD ratio. If IFIS could be predicted and recognized before surgery, proper management strategies would be used, the outcome would be better and the complication rate would be low. Evaluating PD alterations might be more useful than evaluating iris structural alterations in predicting IFIS predisposition in patients who are treated with systemic α-1ARAs. There is still a need for a reliable method that will determine the possibility of IFIS.
Footnotes
Author Disclosure Statement
No financial support was received for this submission. None of the authors had a conflict of interest with the submission.