
Abstract
Abstract
Purpose:
To compare the effect of nonpreserved oxybuprocaine and preserved artificial tears on central corneal thickness (CCT) obtained by 2 pachymeters.
Methods:
In this prospective, placebo-controlled study, involving a random sample of 100 eyes of 50 subjects, aged 24±2.3 years, CCT readings were obtained in 2 separate sessions with the Topcon SP-3000P and ultrasound pachymetry (USP), respectively, before, 5 and 10 min after instillation of a drop each of either oxybuprocaine hydrochloride (oxybuprocaine HCl) (group 1) or carboxymethylcellulose sodium, thera tears (group 2), and placebo.
Results:
The baseline mean CCT for SP-3000P was 509±38 μm and 542±36 μm for USP. No statistical significant differences between baseline CCTs (P>0.05 for both devices) in both groups. In both group experimental eyes, neither SP-3000P nor USP-measured CCTs varied significantly from the control eyes at 5 (P>0.05) and 10 (P>0.05) mins postinstillation of drops in both sessions. In group one, the 95% confidence intervals (CIs) for the SP-3000P CCTs were similar at 5 (−16 to 17 μm) and 10 min (−16 to 17 μm), but in the USP-measured CCTs, it was wider at 10 min (−41 to 46 μm) than at 5 min (−30 to 41 μm) postinstillation. In group two, the 95% CIs at 5 and 10 mins postinstillation, respectively, ranged between −20 and 47 μm, −21 and 43 μm (SP-3000P) and −29 and 23 μm, −26 and 23 μm (USP). Within groups and between groups, variations in CCT were similar at both times intervals in all comparisons.
Conclusion:
Although oxybuprocaine HCl and thera tears consistently did not affect the mean CCT obtained by both devices at both time intervals, variation in SP-3000P measured CCT was more consistent in both sessions and narrower in relation to USP-measured CCT. It may be reasonable to suggest that measurements of CCT in normal patients be taken before examinations requiring instillation of anesthetics or such measurements when obtained postinstillation of either oxybuprocaine or preserved artificial tears be interpreted with caution.
Introduction
Measurement of CCT can be performed by an optical method or with ultrasound, the latter being more reliable.18,19 Although ultrasound pachymetry (USP) is portable, simple to use, and repeatable, its reliability can be limited by variable factors, such as the need for use of topical anesthesia and operator skill, since the USP probe needs to be placed manually as perpendicularly as possible to the center of the cornea. 20 Therefore, even though the use of ultrasound is preferred to measure CCT, noncontact devices have become increasingly important in screening centers, especially in patients who may be at risk of developing glaucoma. Advantages of these noncontact devices stem from the fact, that they do not make contact with the cornea, and as such, no topical anesthesia is required. This has enabled easier and quicker measurement of CCT in routine optometry examinations, even more so in children with whom reliable fixation during contact tonometry or pachymetry measurements is rarely achieved. What is more, the risk of epithelial abrasion and cross infection between patients is virtually obliterated.
Some controversy has trailed the reported influence of the various topical anesthetics on corneal thickness measurements made with several pachymetry devices focused on the central cornea. Some work has reported a temporary increase,21–24 while others did not find significant variations.14,25–29 However, the studies that have reported significant variations in CCT have also differed in their explanations why the variations occur. Some have attributed the changes to structural/functional damage to both the corneal epithelium and endothelium, caused by preservatives in anesthetics,27,30,31 whereas others have reported that diffusion of topical anesthetic into the deep stroma layers causes an inhibition of endothelial cell metabolism, which results in corneal edema and a subsequent increase in corneal thickness.14,21 However, most of these studies were either poorly controlled, employed too few subjects, and/or measurements of CCT were carried out using 1 device.
This study was designed in line with the common clinical practice of using topical anesthetic, where 1 drop is usually sufficient, in determination of CCT and measurements often taken 5 min after instillation. Secondly, to verify if precise CCT measurements by SP-3000P can be obtained in clinics subsequent to performing other examinations requiring the instillation of anesthesia, the current study used a nonpreserved formulation of topical anesthetic [oxybuprocaine hydrochloride (oxybuprocaine HCl)] and a new form of preserved artificial tear (thera tears lubricant) in which the patented preservative is capable of disappearing on contact with the eye surface for maximum comfort. Therefore, the purpose of the study was to compare the effects, if any, that nonpreserved topical anesthetics and preserved artificial tears might cause in determination of CCT by 2 devices. It also sorts and evaluates the consistency and magnitude of this effect, if any.
Subjects and Methods
Study population
The study adhered to the principles of the 1967 Helsinki declaration (as modified in Edinburgh, United Kingdom, 2000). Approval was obtained from the Ethics Committee of College of Applied Medical Sciences. Informed consent was obtained from all participants—100 eyes of 50 subjects, including 27 (54%) males and 23 (46%) females aged between 20 and 29 years [24±2.2 years, mean±standard deviation (SD)] were randomly recruited into this placebo-controlled study, from March 2012 and July 2012. The population was composed of students from different departments of the University.
Subjects with a history or evidence of one of the following were excluded: contact lens wear; participation in any of the previous studies by our research group; primary or secondary anterior segment disease or surgery; astigmatism greater than 3D. 10 Subjects were required to ensure that a minimum of 2 h had elapsed between waking up and commencement of the measurement session to allow time for the dissipation of overnight corneal edema. 32
Measurement protocol
Before measurements of CCT, a comprehensive optometric examination was carried out for each subject, including objective and subjective refraction, keratometry, and slit lamp examination of the anterior segment. At each subject's visit, measurements of CCT were obtained on both eyes consecutively using first the noncontact specular microscope SP-3000P (Topcon Corporation; 3 readings), followed by the handheld USP (Pachette DHG 550; Depew; 3 readings).
SP-3000P measurements were taken before (baseline), 5 and 10 min after instillation of 1 drop of preserved 0.25% carboxymethylcellulose (CMC) sodium (Thera tears lubricant; Akorn, Inc.) or 1 drop of preservative-free 0.4% oxybuprocaine HCl (Minims; Chauvin Pharmaceuticals Ltd.) or normal saline (placebo). For USP measurements, CCT measurements were only obtained 5 min (baseline) and 10 min after instillation of any eye drop since it was necessary to instill topical anesthetics. Also, because it was customary in clinic settings to take USP measurements after about 5 min of instilling topical anesthetic and since a current study 29 has shown that USP-CCT values did not vary significantly at this time point, we considered USP measurements obtained 5 min after instillation of oxybuprocaine HCl as baseline CCT values for this technique.
Each subject had 2 visits, separated by 1 day, to complete the study, so that both eyes were tested with the same eye drop to assess consistency of effects, if any, caused by instillation of either eye drop. The triplicate baseline CCT measurements were used for statistical analysis of instrument repeatability, while averages of the 3 measurements of CCT within each session were used for analysis of the effect of each eye drop. All measurements were carried out between 12:00 and 14:00 h to avoid influence of diurnal variation in CCT. 33
In the first session only, eyes were randomly assigned to 1 of 2 groups by a postgraduate student. Randomization was carried out using a series of random numbers generated on a Microsoft Excel spreadsheet by the same student so that neither the examiners nor the subjects were aware of the selection made: Group one received 1 drop of 0.4% oxybuprocaine HCl (nonpreserved topical anesthetic) in 1 eye and normal saline (placebo) in the other eye; Group two received 1 drop of 0.25% thera tears (preserved artificial tear) in 1 eye and normal saline in the other eye. This was done to eliminate observer and patient bias. Corneal thickness was then measured by SP-3000P (examiner F.H.A.) and USP (examiner U.L.O.) in a masked fashion. During the second visit, no randomization was performed; rather, the protocol was rotated between eyes.
The SP-3000P was used in the automatic image capture, low-intensity mode of the specular microscope. For USP measurements, the cornea was anesthetized with 1 drop of 1% oxybuprocaine HCl (group one), while the probe was always disinfected with an alcohol swab before each subject. The pupil center was used as a reference for probe placement, and the probe was lightly placed perpendicularly to the central corneal surface taking care to avoid excessive compression of the probe tip against the cornea. The ultrasound velocity was set to 1,640 m/s for all measurements in accordance with the manufacturer's calibration recommendation. In both techniques, subjects were required to fixate on a central target.
Data analysis
Statistical analysis was performed using Graphpad Instat version 3.00 (Graphpad Software, Inc.). To achieve a statistical power of 80% at a significance level of α=0.05, 23 subjects were required for each group. This sample size calculation was determined from an initial sample of 15 subjects using the statistical freeware G*Power (version 3.0.5).
All data were entered into a Microsoft Excel spreadsheet. The mean, SD, minimum and maximum values were calculated and presented descriptively. To compare the baseline measurements within sessions and to assess within-session repeatability of each technique, a repeated measures analysis of variance (ANOVA) was conducted on the triplicate baseline CCT measurements in each session.
Further analysis of CCT measurements was performed by subtracting each of the average CCT measurements obtained 5 and 10 min after instillation (of oxybuprocaine or normal saline) from the baseline CCT measurements. For both the control eyes and experimental eyes, the resulting CCT changes in all subjects were averaged at 5- and 10-min intervals and used in all comparative analysis.
To study the variation in corneal thickness at both time points in each group (following instillation of both eye drops), Bland and Altman 34 recommended that the experimental eye and the control eye be compared directly and the size of differences reported. A repeated measures ANOVA was conducted twice for each group, for each technique to compare the variations in mean CCTs in treated eyes at 5 and 10 min intervals with the variations in thickness values of control eyes. We also calculated the 95% limits of agreement (mean±1.96×SDmean difference between treatment) in corneal thickness between experimental eyes and placebo in each group for each technique. For both techniques, similar comparisons were also made to assess between-group (oxybuprocaine and thera tears) differences at 5- and 10-min postinstillation using repeated measures ANOVA. The columns compared were columns of averages [(oxybuprocaine HCl and thera tears, 5 min) vs. (oxybuprocaine HCl vs. thera tears, 10 min) in session one vs. (oxybuprocaine HCl vs. thera tears 5 min) vs. (oxybuprocaine HCl vs. thera tears 10 min) in session two]. A Bland-Altman plot was then plotted to graphically show the 95% limits of agreement between oxybuprocaine and thera tears.
Results
The mean age of group one subjects (oxybuprocaine HCl-treated) was 23±2.4 years (range: 20–29 years) and 24±2.1 years (range: 21–29 years) for thera tear-treated subjects. In all eyes (group one and two, n=100), the mean CCT at baseline for SP-3000P was 509±38 μm (range: 431–571 μm) and 542±36 μm (range: 469–611 μm) for USP (group one only, when topical anesthesia was used, n=50). The triplicate baseline CCT measurements did not vary significantly with repeated measures ANOVA [F(2, 99)=1.88, P=0.16; F(2, 49)=1.05, P=0.36, SP-3000P and USP, respectively].
Within-group changes in mean CCT values obtained by SP-3000P and USP after treatment
The mean CCT obtained at 5 min and at 10 min after instillation of eye drops in both sessions using SP-3000P and USP is shown in Table 1
Oxy eyes, eyes treated with 1 drop of oxybuprocaine hydrochloride (group one); thera tears eyes, eyes treated with 1 drop of preserved artificial tears (group two).
Group One (oxybuprocaine HCl-treated eyes vs. placebo eyes)
Repeated measures ANOVA showed that in SP-3000P measured CCTs, no statistically significant differences were observed between averages of experimental eyes and control eyes in both sessions at baseline [F(3, 24)=20.7, P>0.05], at 5 min postinstillation [F(3, 24)=25.1, P>0.05] and at 10 min postinstillation [F(3, 24)=70.9, P>0.05]. The 95% confidence intervals (CIs) were the same (−16 and 17 μm) at 5 min and at 10 min postinstillation of oxybuprocaine. Differences between the variations at both time intervals in both sessions were also not statistically significant [F(7, 24)=1.9, P>0.05].
In both sessions of USP, between experimental eyes and control eyes, neither the mean CCT at 5 min [F(3, 24)=31.8, P>0.05] and 10 min [F(3, 24)=104.9, P>0.05] postinstillation of drops, nor the variations at 5 and 10 min [F(7, 24)=2.8, P>0.05] postinstillation of drops were statistically significantly different within and between sessions. The 95% limits of agreement between oxybuprocaine and placebo were wider at 10 min (−41 to 46 μm) than at 5 min (−30 to 41 μm) postinstillation.
Group two (thera tear-treated eyes)
In SP-3000P measured eyes, differences in mean CCT between experimental eyes and placebo eyes in session one [F(3, 24)=108.0, P=0.50] and session two [F(3, 24)=163.9, P=0.18] were not statistically significant at 5 (P>0.05) and 10 min (P>0.05) postinstillation. The 95% limits of CIs, 5 min postinstillation, ranged from −37 to 47 μm (session one) and −21 to 17 μm (session two); 10 min postinstillation, it ranged from −20 to 20 μm (session one) and −41 to 43 μm (session two). Variations in CCT were also similar (P>0.05) in both sessions between treatments at all-time intervals postinstillation of drops [F(3, 24)=0.73, P=0.51].
Measuring the CCT by the USP did not result in any statistically significant difference in mean CCT between experimental eyes and placebo eyes in session one [F(3, 24)=82.4, P=0.61] and two [F(3, 24)=163.9, P=0.18]. Differences in CCT variations between treatments in both sessions [F(3, 24)=0.95, P=0.87] was also not statistically significant at both time intervals after instillation (P>0.05 for all comparisons). In sessions one and two, respectively, the 95% limits of agreement between thera tears and placebo, at 5 min postinstillation, ranged from −29 to 24 μm and −18 to 14 μm. At 10 min after drops, it ranged from −26 to 23 μm and −21 to 20 μm.
Between-group comparisons of mean CCT measurements (oxybuprocaine HCl vs. thera tears)
Figures 1–4 are Bland-Altman plots of difference between oxybuprocaine HCl and thera tears as a function of their averages in sessions one and two, at 5 min for SP-3000P (Fig. 1) and USP-measured CCTs (Fig. 2), and at 10 min for SP-3000P (Fig. 3) and USP- measured CCTs (Fig. 4). Results of the analysis show that, although, almost at both times, oxybuprocaine HCl consistently underestimated CCT values obtained by both pachymetry devices with respect to thera tears, these differences were not at anytime statistically significant in SP-3000P-measured CCTs [F(7, 24)=5.4, P=0.98] and in USP-measured CCTs [F(7, 24)=2.6, P=0.95]. The between-group mean differences and 95% limits of agreement were −2 μm (−111 to 106 μm), −5 μm (−111 to 102 μm); −5 μm (−110 to 99 μm), and −5 μm (−104 to 93 μm) for SP-3000P session one 5, 10 min; session two, at 5 and 10 min, respectively. The corresponding values for USP-measured between-group mean CCT differences were −3 (−128 to 123 μm), 3 (−123 to 130 μm); −5 (−101 to 92 μm), and −7 (−104 to 90 μm).
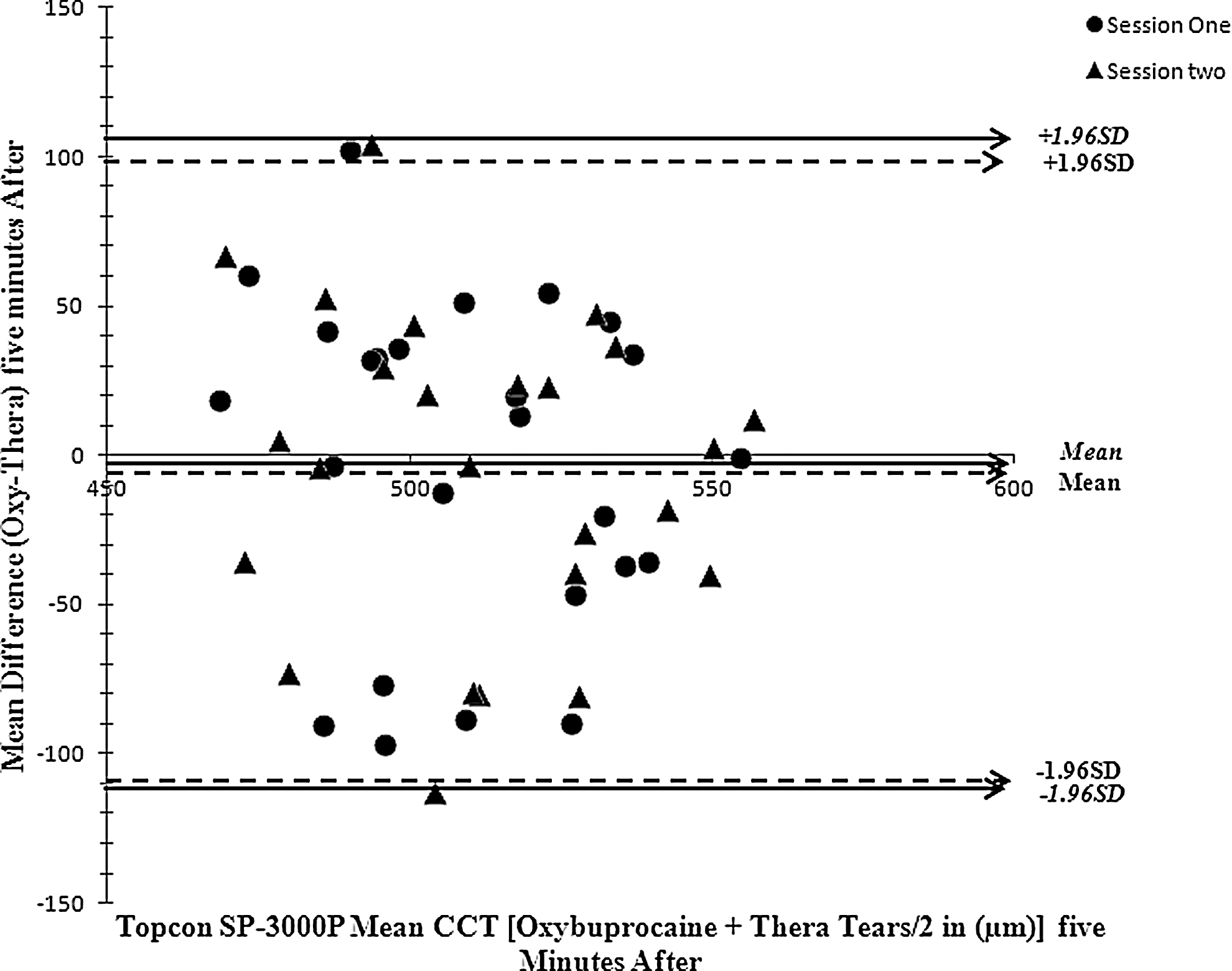
Bland-Altman plot of between-group mean difference [oxybuprocaine hydrochloride (oxybuprocaine HCl) minus thera tears] in the Topcon SP-3000P-measured central corneal thickness (CCTs) as a function of their averages, 5 min after instillation in sessions one and two. Solid lines are 95% limits of agreement in session one and dotted lines for session two.
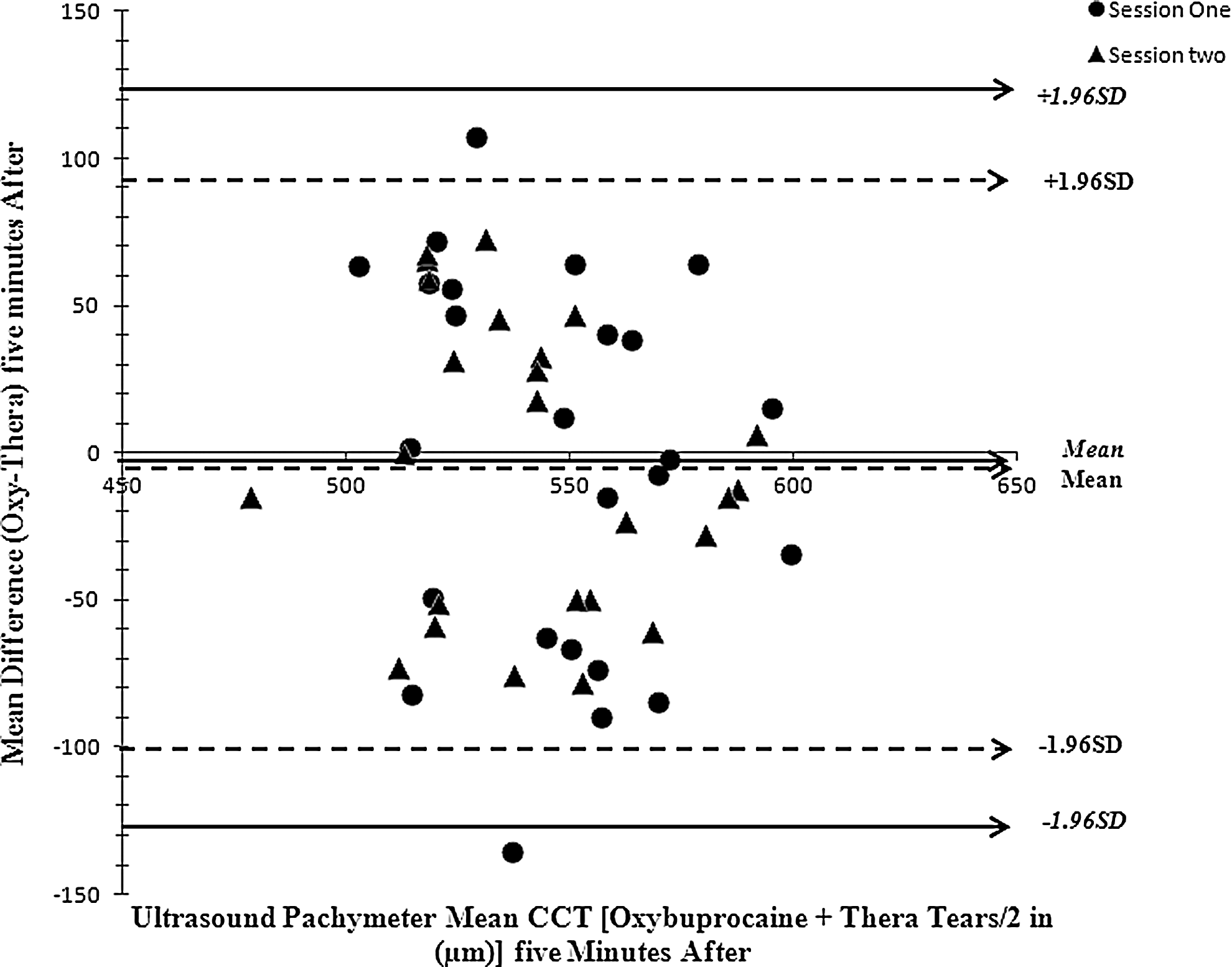
Bland-Altman plot of between-group mean difference (oxybuprocaine HCl minus thera tears) in the ultrasound pachymeter-measured CCTs as a function of their averages, 5 min after instillation in sessions one and two. Solid lines are 95% limits of agreement in session one and dotted lines for session two.
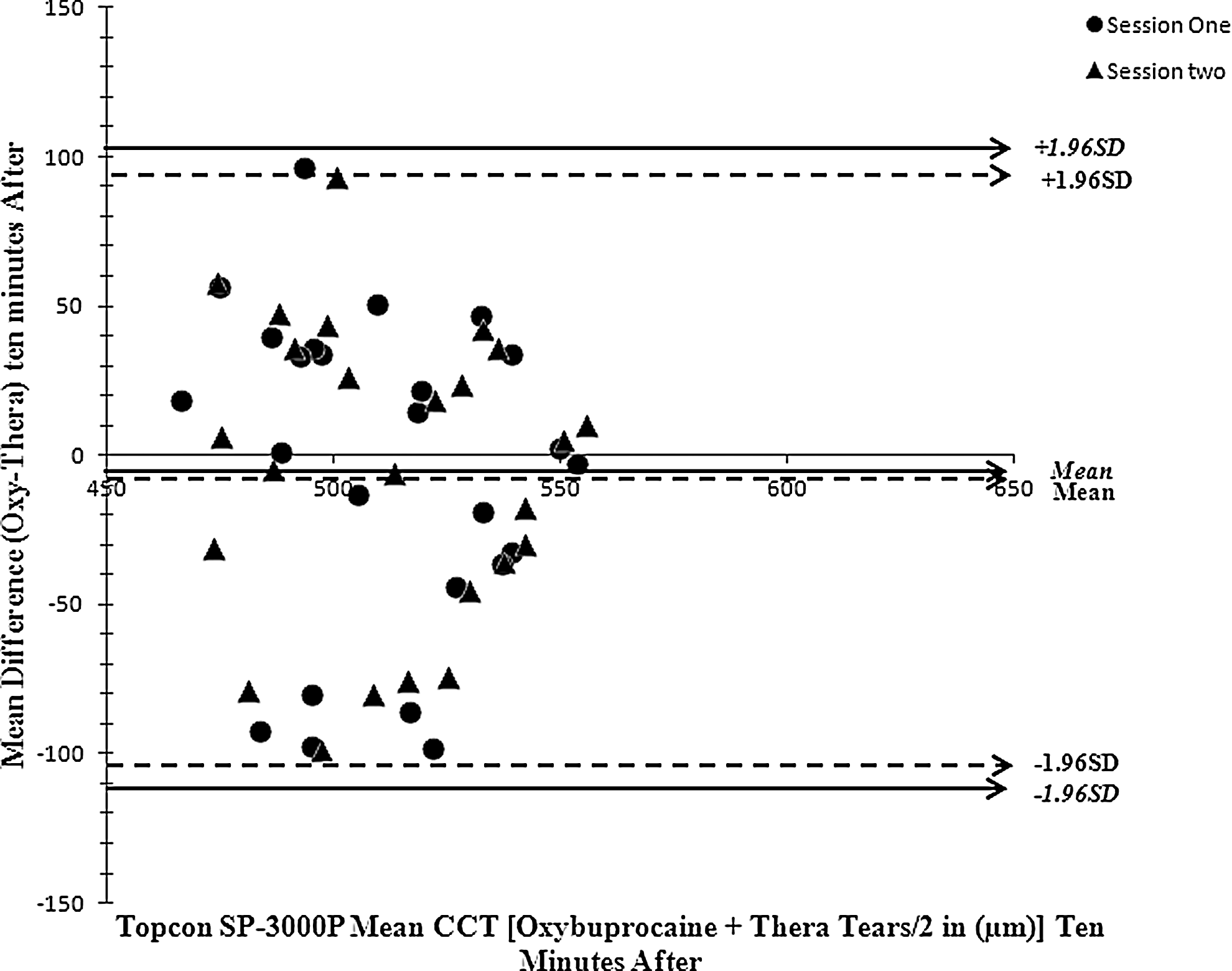
Bland-Altman plot of between-group mean difference (oxybuprocaine HCl minus thera tears) in the Topcon SP-3000P-measured CCTs as a function of their averages, 10 min after instillation in sessions one and two. Solid lines are 95% limits of agreement in session one and dotted lines for session two.
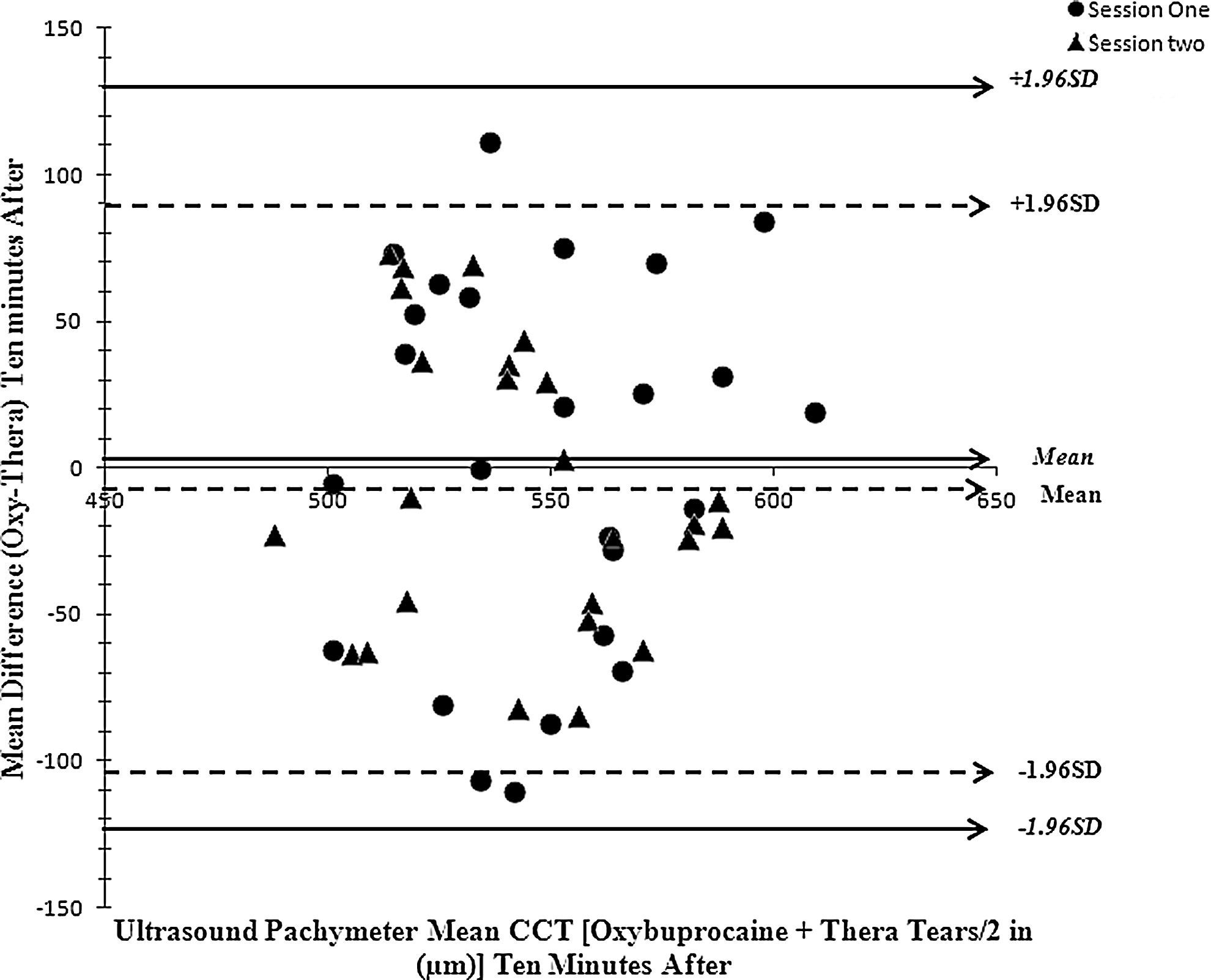
Bland-Altman plot of between-group mean difference (oxybuprocaine HCl minus thera tears) in the ultrasound pachymeter-measured CCTs as a function of their averages, 10 min after instillation in sessions one and two. Solid lines are 95% limits of agreement in session one and dotted lines for session two.
Discussion
The SP-3000P and USP have good repeatabilities18,20,25,35–38 and have been reliably used in monitoring changes in CCT after instillation of topical anesthetics in the past.14,23,25 In this study, the baseline CCT measurements were similar within sessions and between sessions of both instruments. The effect (no significant change) of instilling either 1 drop of oxybuprocaine HCL or thera tears was similar when measurements were obtained 5 and 10 min after instillation, with either instrument. It was also more consistent between sessions of SP-3000P CCT measurements than between sessions of USP-CCT measurements, at both time intervals. Variations in CCT measurements after drop instillation although not significant (Figs. 1–4) reveals that a maximal difference between oxybuprocaine HCl and thera tears occurred in USP-measured CCTs with limits of agreement between groups ranging up to 130 μm and below −128 μm (Figs. 2 and 4) in relation to a maximum of 108 μm and a minimum of 111 μm in SP-3000P-measured CCTs (Figs. 1 and 3). It can therefore be deduced that although both instruments were consistent in not causing any significant change in measured CCTs, the SP-3000P due to its automated operational principle (automated device) had better consistency in relation to the USP, which is more dependent on the accuracy of manual probe placement.
The thera tears used in this study is a lubricant in a bottle composed of the CMC sodium preserved by sodium perborate. The manufacturers state that this preservative turns into water and oxygen on contact with the eye surface, thereby enhancing maximum comfort. In comparison to oxybuprocaine and placebo, and with respect to baseline corneal thickness, instillation of a drop of thera tears lubricant caused no significant change in mean CCT as measured by both pachymeters or in the variation in CCT at any time. This could be due to the disappearance of the preservative when the drop is in contact with the ocular surface as claimed by the manufacturers.
Again, although instillation of both oxybuprocaine HCl and thera tears caused no significant change or variation in CCT, between both treatments, the latter had a propensity to return higher CCT values at both time intervals, which was consistent in both sessions and in both techniques. This could be explained from the fact that, the latter is an artificial tear drop with superior hypotonicity, mucoadhesive properties, and increased ocular residence time, as compared to the former. Previous studies have reported a significant increase in measured corneal thickness after instillation of various artificial tear drops in dry eye patients, but not in the control normal subjects.15,36,37
With the increase in the use of noncontact devices in obtaining CCT measurements, it's not uncommon to observe that CCT measurements in the majority of patients may be obtained subsequent to other examinations requiring instillation of topical anesthetics, such as Goldmann applanation tonometry. Thus, some of these patients may show variations in CCT values with application of artificial tears or variations in SP-3000P-measured CCTs postapplication of topical anesthetics, which should be taken into consideration when preoperative corneal thickness measurements are performed before and after refractive surgery. Caution should therefore be taken when interpreting CCT measurements obtained in such patients, since a combination of both drop effects may likely show very wide variations (up to −111 to 106 μm) in the measurements returned. Mukhopadhyay et al. 24 and Asensio et al. 14 reported a similar degree of variability in CCT (−10 to 30 μm, >10 μm, respectively). Similarly, with such variations, we run the risk of misclassification for primary open-angle glaucoma or ocular hypertension due to falsely interpreted cornea thickness increases. 38 Further study will be required to determine if this wide individual CCT variation is sustained, and if so, for how long.
One of the major strengths of this study is the placebo-controlled randomized design. The key advantages being that it often has high efficiency relative to the cohort method and that it is self-controlled: time-invariant confounders, such as sex, location, genetics, and underlying state of health are controlled for implicitly. 39 The limitations of this study include: (1) the recruitment of only healthy subjects and (2) the narrow age range, both of which may limit the applications of the results of this study. The authors therefore recommend the inclusion of subjects with dry eyes, diabetes, and glaucoma subjects of various age groups in future studies.
In summary, the instillation of 1 drop of thera tears lubricant (CMC sodium) and nonpreserved oxybuprocaine HCl consistently caused no significant change in CCT values obtained by SP-3000P and USP. There was wide variability in measured CCT between oxybuprocaine and thera tears (although not statistically significant), but more consistent in both sessions of SP-3000P-measured eyes than in the USP-measured eyes. This should be considered by clinicians when precise CCT measurements are needed, such as before refractive surgeries and in normal patients on regular use of artificial tears. More importantly, SP-3000P CCT measurements could be more reliable if performed post-other ophthalmic examinations requiring instillation of topical anesthetics.
Footnotes
Acknowledgments
The authors extend their appreciation to the Research Centre, College of Applied Medical Sciences and the Deanship of Scientific Research at the King Saud University for funding this research.
Author Disclosure Statement
No competing financial interest exists.