
Abstract
Abstract
Purpose:
In this study, we investigated the efficacy of systemic and intravitreal (IV) infliximab treatments and compared these 2 different treatment modalities in an experimental model of endotoxin-induced uveitis (EIU).
Methods:
Twenty-four white New Zealand rabbits were equally divided into 4 groups. Group 1 received IV injection of lipopolysaccharide (LPS), group 2 received IV injections of LPS and saline, group 3 received IV LPS and IV 2 mg/0.1 cc infliximab, and group 4 received IV LPS and 5 mg/kg intravenous infliximab. Inflammation was determined with objective and subjective tests. The subjective test was clinical determination of uveitis, the objective tests were determination of protein concentrations and tumor necrosis factor alpha (TNF-α) levels and histopathology.
Results:
Clinical examination score was lower in group 3 and group 4 (4±0.6 and 3.5±1.6, respectively) when compared with group 1 (P=0.02; P=0.04, respectively) and group 2. In group 3 and 4, the aqueous and vitreous protein and TNF-α concentration measured significantly lower than group 1 and 2. In histopathologic examination, there was no statistically significant difference between group 1, 2, and 3 (3.5±0.5, 3.6±0.5, 3.6±0.5, respectively). However, the lowest histopathologic inflammation was determined in group 4 (2.5±0.5) (compared with group 1 and group 3, respectively; P=0.03; P=0.014).
Conclusion:
In a rabbit model of experimental EIU, intravenous administration of infliximab was more effective than IV route in an acute period.
Introduction
U
In this study, we aimed to investigate the efficacy of systemic and IV infliximab and compare these 2 treatment modalities. To our knowledge, this is the first report on the comparison and efficacy of different treatment modalities in an experimental model of uveitis.
Methods
Experimental protocol
Twenty-four New Zealand white rabbits (2.0–3.0 kg; 14–16 weeks of age) were selected for this study. All rabbits were treated in accordance with the Association for Research in Vision and Ophthalmology Statement for the use of Animals in Ophthalmic and Vision Research and our experiment was approved by the local ethics committee of Gazi University Animal Research Center (No. G.Ü.ET-09.071).
The animals were kept under standard laboratory conditions, at 21°C and 50% humidity and fed with water and rabbit food in a 12-h light/12-h dark cycle. The animals were anesthetized with intramuscular injections of ketamine hydrochloride 10% (35 mg/kg, Alfamine; Alfasan) and xylazine hydrochloride (5 mg/kg, Alfazyne; Alfasan). Five minutes before any manipulation, 3 drops of propacaine hydrochloride 0.5% (Alcaine; Alcon) was used for topical anesthesia. Only 1 eye (right eye) of each animal was used for this experiment. The sterilization was provided by a povidone–iodine solution 5% before any manipulation. Injections were performed under sterile conditions 2.5 mm posterior to the limbus using a 1-mL insulin syringe with a 27-gauge needle. After the injections, a cotton-tipped swab was pressed against the injection site for 10–15 s to prevent extraocular reflux. Lomefloxacin drops and tobramycin ointment were applied to all eyes after the injections.
Treatment groups
The animals were divided into 4 groups. Group 1 (n=6) received IV lipopolysaccharide (LPS) endotoxin, group 2 (n=6) received IV LPS plus IV saline (0.1 mL of pyrogen-free 0.9%), group 3 (n=6) received IV LPS plus IV infliximab (2 mg/0.1 cc), and group 4 (n=6) received IV LPS plus intravenous infliximab (5 mg/kg).
Endotoxin-induced uveitis method
Endotoxin-induced uveitis (EIU) was achieved by IV injections of 2 μg/0.1 cc LPS from Salmonella typhimurium (Sigma Chemical Co.).
IV infliximab injection
Twenty-four hours after IV LPS injection, 2 mg/0.1 cc infliximab (Remicade; Shering-Plough) was injected intravitreally in group 3.
Systemic infliximab treatment
Twenty-four hours after IV LPS injection, infliximab, which was dissolved in sterile apyrogen saline at a dose of 5 mg/kg, was infused in 1 h through the marginal ear vein in group 4.
Collection of aqueous humor and vitreous samples
After animals were killed, aqueous and vitreous samples were collected immediately from the right eye of the animals. Approximately 0.2 mL of aqueous and 0.4 mL of vitreous samples were collected using a 1-mL insulin syringe with a 27-gauge needle, avoiding injury to the lens, iris, or retina. The globe was filled with 10% formaldehyde. All samples were centrifuged at 12,000 rpm for 3 min and then stored at −80°C until the biochemical assays were performed. The aqueous and vitreous samples were studied for TNF-α levels and protein concentrations.
Euthanasia and enucleation
Twenty-four hours after treatment (IV and intravenous infliximab), an overdose of xylazine hydrochloride (200 mg/kg, Alfazyne; Alfasan) was injected into the heart for euthanasia. After euthanasia, the eyes were enucleated. The enucleated material was stored at −80°C until histopathologic examination.
Determination of treatment groups
The animals were determined with objective and subjective tests. The subjective test was clinical determination of uveitis, the objective tests were determination of protein concentrations and TNF-α levels and histopathology.
Clinical determination
The degree of anterior uveitis was assessed clinically by 1 masked observer (N.Y.) 24 h after IV LPS injections and 24 h after systemic treatments. All eyes were evaluated and then scored clinically for vascular, pupillary and, exudative signs. The intensity of the signs of intraocular inflammation was graded by using the clinical scoring system. 10 Iris hyperemia was scored for absence (0), mild (1), or presence (2); flare, miosis, and hypopyon were scored for absence (0) or presence (2). The maximum possible uveitis score was 8.
Measurement of protein concentration in aqueous humor and vitreous
The total protein concentration was measured in the aqueous humor and vitreous by the Lowry method. 11 Values were expressed as mg protein/mL aqueous or vitreous.
Measurement of TNF-α levels in aqueous humor and vitreous
TNF-α levels were measured in the aqueous humor and vitreous by using the enzyme-linked immunosorbent assay (ELISA) method. The TNF-α kit was specific to recombinant rabbit TNF-α (No. E0133RB; USCN-LIFE Science, Inc.). Values were expressed as pg/mL.
Histopathologic determination
Enucleated eyes were fixed in 10% formaldehyde for 2 days and then embedded in paraffin. Four micrometer sections were obtained from the paraffin blocks and stained with standard hematoxylin–eosin staining. The histopathologic examination was performed under the light microscopy (Olympus) at ×200 magnification. The histopathologic evaluation of inflammation was graded by using the scoring system modified from Verma et al. 12 The iris-ciliary body inflammation intensity was scored as follows: grade 1, 1 to 10 cells per field; grade 2, 11 to 30 cells per field; grade 3, 31 to 100 cells per field; and grade 4, 101 to 300 cells per field.
Statistical analysis
Statistical analysis was performed using SPSS® v16.0 for Windows. The data obtained from the 4 groups were analyzed with the nonparametric Kruskal–Wallis test and Mann–Whitney U test. A value of P<0.05 was considered to be statistically significant. All data are expressed as the mean±standard deviation.
Results
Clinical score
Intense inflammation was observed in group 1 and group 2 (Fig. 1a, b). The mean clinical severity score was 6.6±0.5 and 5.5±1.9 in group 1 and 2, respectively (P>0.05). Ocular inflammation was significantly reduced in treatment groups when compared with the group 1 (P=0.02, P=0.04, respectively), the mean clinical severity score was 4±0.6 and 3.5±1.6 in group 3 and 4, respectively (Fig. 1c–f ). The comparison of clinical severity score between group 1 and 2 and between group 3 and 4 showed no significant difference (P>0.05) (Fig. 2).

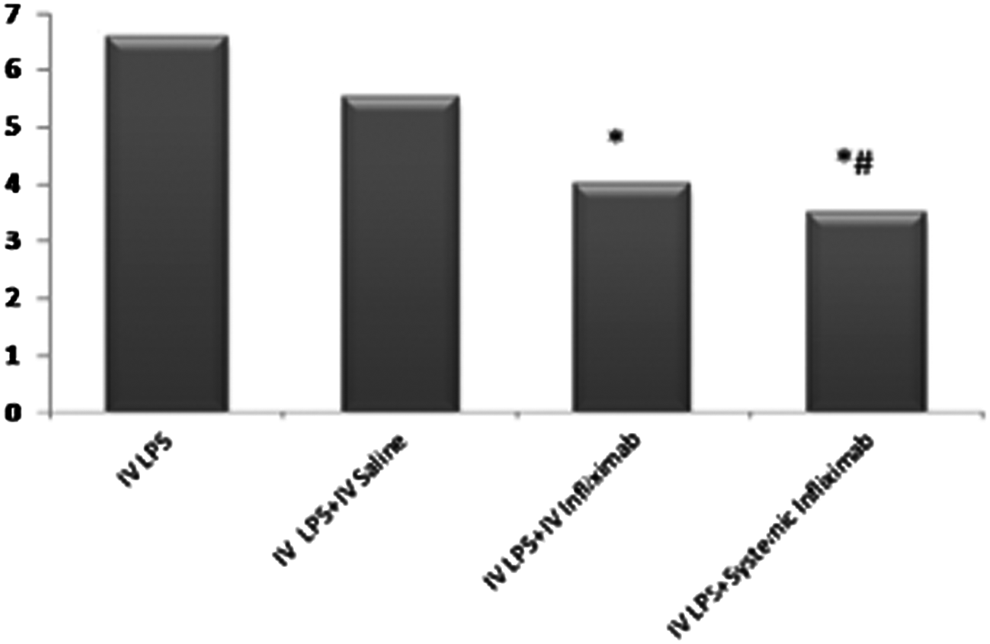
Clinical severity score. *P<0.05, when compared group 3 and 4 with the control group (group 1),
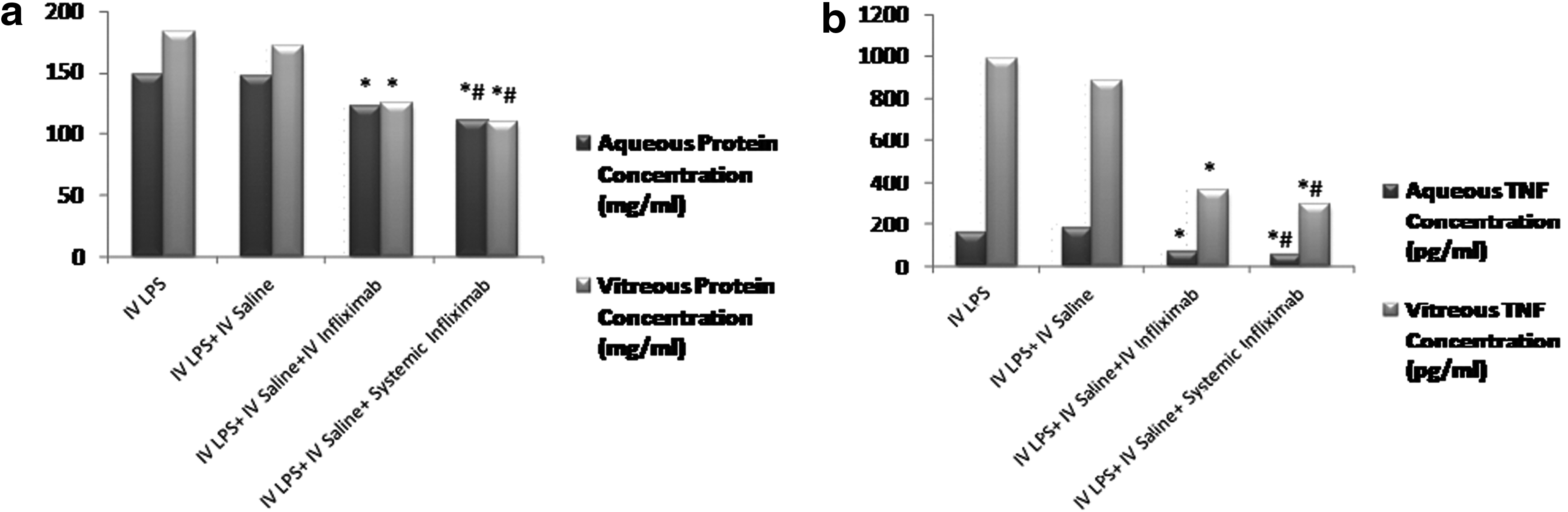
Protein concentration in aqueous humor and vitreous
The protein concentrations in the aqueous humor and vitreous are shown in Fig. 2. Severe inflammation was found in group 1 and 2 and a significant reduction was observed in group 3 (aqueous, P=0.004; vitreous, P=0.004) and 4 (aqueous, P=0.002; vitreous, P=0.002) when compared to group 1. In group 4, the protein concentration was lower than group 3, but this was not statistically significant (aqueous, P=0.065; vitreous, P=0.092) (Fig. 3a).
The effect of infliximab treatment on
TNF-α levels in aqueous humor and vitreous
The TNF- α levels in the aqueous humor and vitreous are shown in Fig. 3. IV injection of LPS induced high TNF-α levels in the aqueous humor and vitreous. After infliximab treatment, TNF-α levels in the aqueous humor and vitreous were reduced significantly in group 3 (aqueous, P=0.004; and vitreous, P=0.004) and group 4 (aqueous, P=0.002; vitreous, P=0.002). In group 4, the TNF-α levels were lower than group 3, but this was not statistically significant (aqueous, P=0.200; vitreous, P=0.109) (Fig. 3b).
Histopathology
The mean histopathologic inflammation intensity score in the iris-ciliary body is shown in Table 1. The inflammation was severe in group 1, 2, and 3 and there was no statistically significance between these groups. However, in group 4, inflammation was reduced significantly when compared with group 1 (P=0.03) and group 3 (P=0.014) (Fig. 4a–d).

P>0.05, when compared group 3 with group 1.
P<0.05, when compared group 4 with group 3 and 1.
LPS, lipopolysaccharide; IV; intravitreal.
Discussion
Uveitis is a complex disorder involving inflammation of the uveal tract, and the exact mechanism underlying uveitis remains unclear. EIU, a model of intraocular inflammation provided by LPS, is a useful experimental model for understanding acute uveitis in humans and it is used in studies in which the pathophysiology of this disease is examined. Following 24 h of sublethal injection of LPS intraperitoneally or intravitreally, maximal intraocular inflammation is characterized by miosis, iris hyperemia, protein leakage to the humor aqueous associated with the breakdown of blood–ocular barriers, as well as inflammatory cell infiltration of the anterior uveal tissue and vitreous.13,14 In the present study, LPS was injected intravitreally, as Howes et al. 14 described in rabbits, and severe inflammation was elicited similar to that reported by other studies in the literature.9,15,16
In the pathogenesis of EIO, TNF-α plays a critical, early, and very important role. More specifically, TNF-α, a pluripotent cytokine, is involved in a variety of inflammatory pathways. In the early phase of inflammation, TNF-α is released, and TNF-α receptors are expressed by ocular inflammatory cells (macrophages, neutrophils, T and B lymphocytes, natural killer). Subsequently, TNF-α increases the expression of high-affinity IL-2 receptors and induces the production of IL-1. Thus, this provides the synthesis of prostaglandins and induces vasodilatation, breakdown of blood–ocular barriers, rapid ocular inflammatory cells infiltration, and protein leakage into the aqueous humor, anterior uveal tissue, and vitreous.17,18 Further inflammatory cells induce further TNF-α, causing further inflammation.
This circle can be broken by the use of TNF-α antagonists such as etanercept, infliximab, and adalimumab. Thus, in ocular inflammation, TNF-α inhibitors are significant therapeutic agents, including infliximab, which binds to both membrane-bound TNF and soluble TNF. Clinical studies have shown the efficacy of systemic infliximab therapy for the treatment of ocular uveitis.2–7 Additionally, Markomichelakis et al. 8 reported the rapid effect of a single intravenous infliximab infusion for ocular inflammation. The effect of systemic infliximab has also been shown in an experimental model of uveitis. Additionally, Diaz-Llopis et al. 15 have demonstrated that prophylactic high-dose intravenous infliximab (20 mg/kg) reduced ocular inflammation significantly. Finally, Johnsen-Soriano et al. 19 assessed the acute effect (24-h effect) of intravenous infliximab and adalimumab in the EIU rat model, finding that protein levels in aqueous and histopathological inflammation were reduced effectively.
In the present study, 5 mg/kg infliximab infusion was effective for reducing the clinical score, protein, and TNF-α levels in aqueous-vitreous and histopathological inflammation when compared with the control group. However, in 3 different studies that administered different anti-TNF-α antibodies both systemically and locally, ocular inflammation was not reduced and inflammation was exacerbated.20–22 In these studies, the variable results may be associated with different anti-TNF-α therapies. Infliximab is more effective and specific to the TNF receptor p55, which underlies most of the inflammatory activities, than the previous anti-TNF-α antibodies.
The human and animal experimental studies demonstrated that systemic infliximab therapy shows promising results for treatment of noninfectious ocular inflammation.2–8 Despite the effectiveness of the systemic infliximab therapy, serious adverse effects have been described, including infections, malignancy, autoimmune disease, and autoantibody formation. This has led researchers more recently to study intraocular infliximab injection to reduce or eliminate the serious side effects of systemic infliximab. Additionally, researchers have considered whether a higher intraocular concentration could be achieved with IV infliximab. However, the inner and outer retinal–blood barrier and the molecular weight of the drug can prevent the effects of infliximab.
For IV drugs, retinal toxicity is an important problem. In 2 separate studies, the rabbit model was used to evaluate the ocular toxicity of IV infliximab at various doses.23,24 Giansanti et al. 23 described that IV infliximab was safe at a dose of up to 1.7 mg/0.1 cc. On the other hand, Theodossiadis et al. 24 showed that 2 mg/0.1 cc dose of IV infliximab could be used safely. Additionally, Melo et al. 25 demonstrated that IV infliximab at doses of 100 and 400 μm evidenced no toxicity to the retina in primates.
As a result, IV infliximab has recently begun to be used clinically. For example, Giganti et al. 26 reported that IV infliximab at a lower dose (0.05 mg) was associated with retinal toxicity in 4 patients with adult macular degeneration or choroidal neovascular membranes (electroretinography and microperimetry changing was detected). Additionally, Wu et al. 27 showed that IV infliximab at doses of 1 mg and 2 mg was associated with an intraocular inflammatory reaction. However, 6 different studies presented a single IV injection of 1 mg or 1.5 mg infliximab and concluded that the drug was safe in all 66 eyes with pathologic features28–33 included in the study.
In our study, a dose of 2 mg/0.1 cc IV infliximab was used in group 3. TNF-α and protein levels (in the aqueous humor and vitreous) and clinical scores were reduced significantly in group 3 twenty-four hours after injection of IV infliximab. However, there was no histopathologic difference between the IV infliximab (group 3) and the control group. Nevertheless, Hosseini et al. 9 showed that histopathological inflammation was reduced effectively on the seventh post-IV infliximab (1 mg/0.1 cc) injection day.
In group 4 (systemic infliximab), TNF-α, protein levels, and histopathologic inflammation were lower than group 3 (IV infliximab). As described previously, TNF-α is a proinflammatory mediator, and if TNF-α levels persists at a medium level, the inflammation becomes more severe. In group 3, TNF-α levels started to decrease; however, histopathologic inflammation did start to decrease. On the other hand, in group 4, histopathologic inflammation was reduced with decreasing TNF-α levels. The explanation of this result is probably that the TNF-α levels in group 4 were lower than group 3, and the group 4 TNF-α level reduction was enough for the decrease of histopathologic inflammation.
In our experimental study, enucleation was performed after 24 h of treatment (IV and intravenous infliximab). At 24 h of IV infliximab in group 3, we failed to find any histopathological changes, whereas the TNF-α levels decreased. Although Hosseini et al. 9 gave less IV infliximab doses (1 mg/0.1 cc) than our study, the results showed remission of inflammation on day 7. We think that, if we determined histopathologic inflammation during the late period as Hosseini et al. did, we could find less inflammation in the IV infliximab group (group 3). Several possible explanations for the late histopathologic effect of IV infliximab or the fast effect of systemic inflammation exist. First, the IV infliximab molecular weight could contribute. Studies suggest that larger antibodies such as bevacizumab could not penetrate the retina. Although bevacizumab's molecular weight is large, it is effective in treating preretinal, retinal, and choroidal neovascularization. Infliximab's molecular weight (149 kDa) is similar to bevacizumab (144.1 kDa). 34 This explains how IV infliximab could exert its effects (even if these effects are late). Additionally, in immunohistochemical experiments with an anti-idiotype antibody recognizing infliximab, inliximab was observed at least in the proximal retinal layers 5 days after IV injection (Liarakos et al., unpublished). Additionally, Melo et al. 25 demonstrated that IV infliximab penetrated deeply to all retina layers in primates 7 days after injection. Systemic infliximab was also found to reach uveal tissue directly and rapidly, lead to early reduction in TNF-α levels, and histopathologic inflammation.
In conclusion, our study suggests that intravenous infliximab infusion was more effective than IV infliximab in an acute period. However, further experimental studies are needed to compare both therapies (IV and systemic infliximab) over a longer period for the late effects.
Footnotes
Acknowledgment
The authors thank the Society of Turkish Ophthalmology for supporting this study.
Author Disclosure Statement
There is no financial interest or conflict of interest for all the authors.