
Abstract
Abstract
Purpose:
To investigate the rate of secondary glaucoma after intravitreal dexamethasone 0.7 mg (Ozurdex®) implantation over a clinical treatment period of 1 year.
Methods:
A prospective study of a series of 16 patients (9 males, 7 females; mean age 76 years) suffering from central- or branch retinal vein occlusion treated with dexamethasone 0.7 mg were followed up for 12 months. Main outcome measures were intraocular pressure (IOP) determined with Goldmann applanation tonometry (GAT) and Pascal dynamic contour tonometry (DCT), as well as best-corrected visual acuity (BCVA) and central retinal thickness measured with optical coherence tomography (OCT).
Results:
BCVA (logMAR) improved in treated patients from mean 0.81 at baseline to a peak of 0.47 after 2 months but declined irrespective of reinjections to 0.87 at 12 months. Central retinal thickness measured with OCT initially decreased but increased again with recurring macular edema. 69% of patients treated with dexamethasone 0.7 mg had an IOP increase of at least 5 mmHg. In total, 50% of patients had an increase of ≥10 mmHg during the studied period. The IOP increase in treated eyes was significant 1, 2, 3, and 8 months after dexamethasone 0.7 mg implantation.
Conclusion:
Secondary glaucoma after intravitreal injection of dexamethasone 0.7 mg might be underestimated in the GENEVA studies. The clinical safety profile reported here calls for thorough identification of suitable patients and frequent IOP control if dexamethasone 0.7 mg (Ozurdex) is applied as a long-term treatment.
Introduction
The sustained-release dexamethasone implant (Ozurdex®) has become available to treat vision loss in patients suffering from macular edema due to retinal vein occlusion and noninfectious uveitis.6–8 Although it has been shown in randomized controlled trials that the dexamethasone 0.7 mg implant can be a favorable treatment option in patients with macular edema due to BRVO and CRVO, long-term adverse events associated with the single or repeated implantation of the biodegradable drug-delivery system are still undetermined. Since its first approval in the United States in 2009, new data regarding the clinical safety profile of the dexamethasone 0.7 mg implant have emerged. In our first clinical experience, we found indications that the steroid response to the dexamethasone 0.7 mg implant might be higher than noted in the approval studies especially after repeated injections of the drug carrier.
We investigate in this prospective study the rate of secondary glaucoma or steroid response following intravitreal injection of dexamethasone 0.7 mg (Ozurdex) with 2 tonometric methods: the Goldmann applanation tonometry (GAT) and the Pascal dynamic contour tonometry (DCT). The second allows for objective intraocular pressure (IOP) measurements independent of corneal properties and it is less prone to examiner dependant measurement bias. Here we present for the first time data on the rate of IOP elevation after Ozurdex implantation with an objective method in a systematic fashion.
Methods
Study design
A prospective study of a series of 16 patients (9 males, 7 females; mean age 76 years, 5 CRVO, 11 BRVO), with recent retinal vein occlusion and macular edema were treated with dexamethasone 0.7 mg implant and followed up over 12 months. Patients were enrolled in this study at the Herzog Carl-Theodor Eye Clinic between January and June 2011. Complete ophthalmological examinations were performed before implantation and at follow up visits (1,2, 3, 6, 8, 10, and 12 months) after the dexamethasone 0.7 mg implantation, including visual acuity, biomicroscopy, GAT, DCT, optical coherence tomography (OCT), and fluorescein angiography if applicable. Focal and/or panretinal laser coagulation was performed as required. Pachymetry was performed at the baseline visit to correct for interindividual differences in central corneal thickness.
The primary patient eligibility criteria for the study were age over 18 years, recent retinal vein occlusion (no longer than 3 months), no history of glaucoma or suspected glaucoma, no known steroid response, and no history of pretreatment with other intravitreal injections, such as anti-VEGF, triamcinolone, and topical steroids. Absence of glaucoma was ascertained by a negative family or personal medical history for glaucoma disease, no pretreatment with IOP-lowering medications, and no-glaucoma suspicion on the study entry examination (including IOP and optic nerve head evaluation). To exclude secondary neovascular glaucoma, gonioscopy was performed on each patient. Written informed consent, according to the principles of the declaration of Helsinki, was obtained from each participant.
Study treatment
On entry, study eyes received 1 initial treatment with dexamethasone 0.7 mg implant. Reinjection criteria were determined based on clinical judgment, such as recurrence of macular edema (increase of central retinal thickness in OCT ≥100 μm) and deterioration or loss of best-corrected visual acuity (BCVA) (off at least 1 line) after an initial clinical improvement. Repeated injections were administered no earlier than 3 months after the first dexamethasone 0.7 mg implantation. Altogether 9 out of 16 patients required reinjection of dexamethasone 0.7 mg at least once over the follow-up time of 12 months. One of these 9 patients required 2 dexamethasone 0.7 mg reinjections within the study period.
Outcome measures
Main outcome measures were IOP measured with GAT and Pascal DCT. Furthermore BCVA and central retinal thickness (OCT) was recorded at every follow-up visit.
Measurements of IOP
After instillation of proparacaine 0.5% topical anesthetic, IOP measurements were obtained in miosis by GAT and DCT with a time interval of 5 min between them. The same examiner obtained all IOP measurements. GAT was performed with a slit lamp tonometer calibrated according to the manufacturer's guidelines. Three GAT readings were obtained for each eye and mean IOP was calculated.
DCT was performed with the Pascal digital tonometer (dynamic contour tonometer, DCT-PASCAL; Ziemer Ophthalmic Systems Group Co.) mounted to a slit lamp. The IOP value and a quality score (Q) indicating the reliability of the measurement are displayed on the instrument after every measurement. According to the manufacturer's instructions only measurements with excellent quality (Q1 and Q2) were included in data analysis as a mean value of 3 repeated measurements.
Results
Visual acuity
After intravitreal implantation of dexamethasone 0.7 mg, BCVA (LogMAR) initially improved in treated patients from mean 0.81 at baseline to mean 0.5 after 4 weeks. BCVA reached a peak of 0.47 after 2 months. Thereafter, BCVA consecutively decreased over a period of 3–6 months after the initial treatment. Repeated injections were necessary in 9 out of 16 patients. After a repeated injection BCVA increased again to a mean of BCVA 0.61 after 6 months. At 12 months, mean BCVA of all patients was 0.87. Mean BCVA over the observation period of 12 months is given in Fig. 1.

Mean best-corrected visual acuity
Central retinal thickness
Central retinal thickness decreased within the first 2 months after treatment with dexamethasone 0.7 mg as measured with OCT (Fig. 2) (Mean 541 μm preinjection to mean 236 μm 2 months after injection). After 3–4 months, macular edema recurred and central retinal thickness increased again in the same manner as BCVA deteriorated. In all cases of repeated injections with dexamethasone 0.7 mg, macular edema decreased after a second or third treatment with mean central retinal thickness at 444 μm measured after 12 months. However, OCT scans of most patients showed progressive irregularities of the RPE and the neurosensory retina appeared atrophic. These morphological changes were pronounced in patients requiring repeated injections due to recurring macular edema.
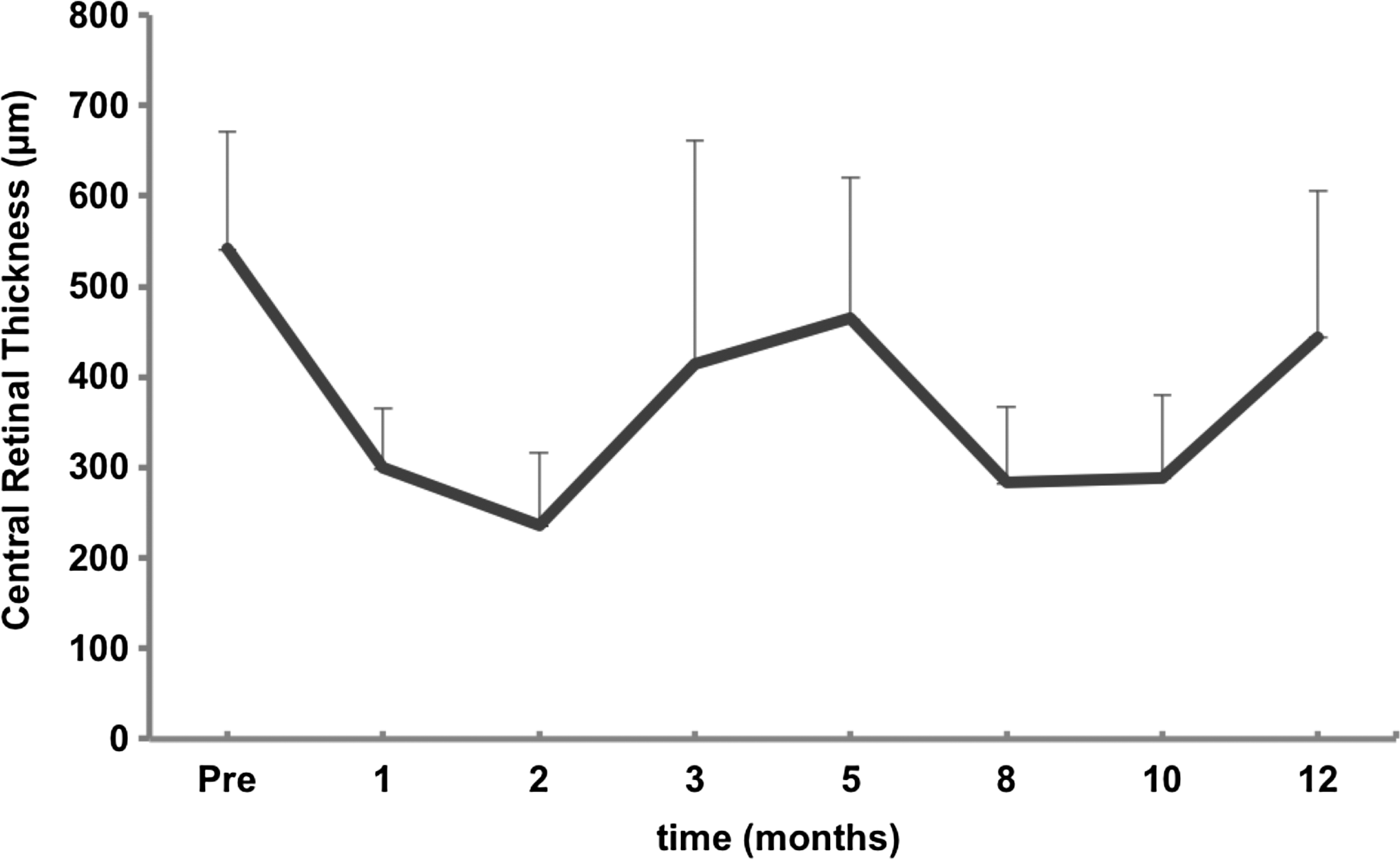
Mean central retinal thickness in μm after dexamethasone 0.7 mg treatment. Observation period 12 months. Bar is 95% CI of the mean.
IOP (Goldmann tonometry Pascal tonometry)
Over the follow-up time of 12 months in total 11 out of 16 patients (69%) treated with dexamethasone 0.7 mg had an increase of IOP of ≥5 mmHg, whereof 8 patients (50%) had an increase of ≥10 mmHg at least once in the observation period. These patients were classified as “Responder.” In total 9 out of 16 patients (56%) had an IOP ≥25 mmHg during the study period. Patients with IOP increase of less than 5 mmHg were classified as “Non-Responder” (5 out 16 patients, 31%). Mean IOP of Responders and Non-Responders is given in Figs. 3 and 4. In Fig. 3, the asterisk (*) marks significant IOP differences (P≤0.05, paired t-test) between Responders and Non-Responders. GAT measurements were in average 2–3 mmHg higher than DCT readings.
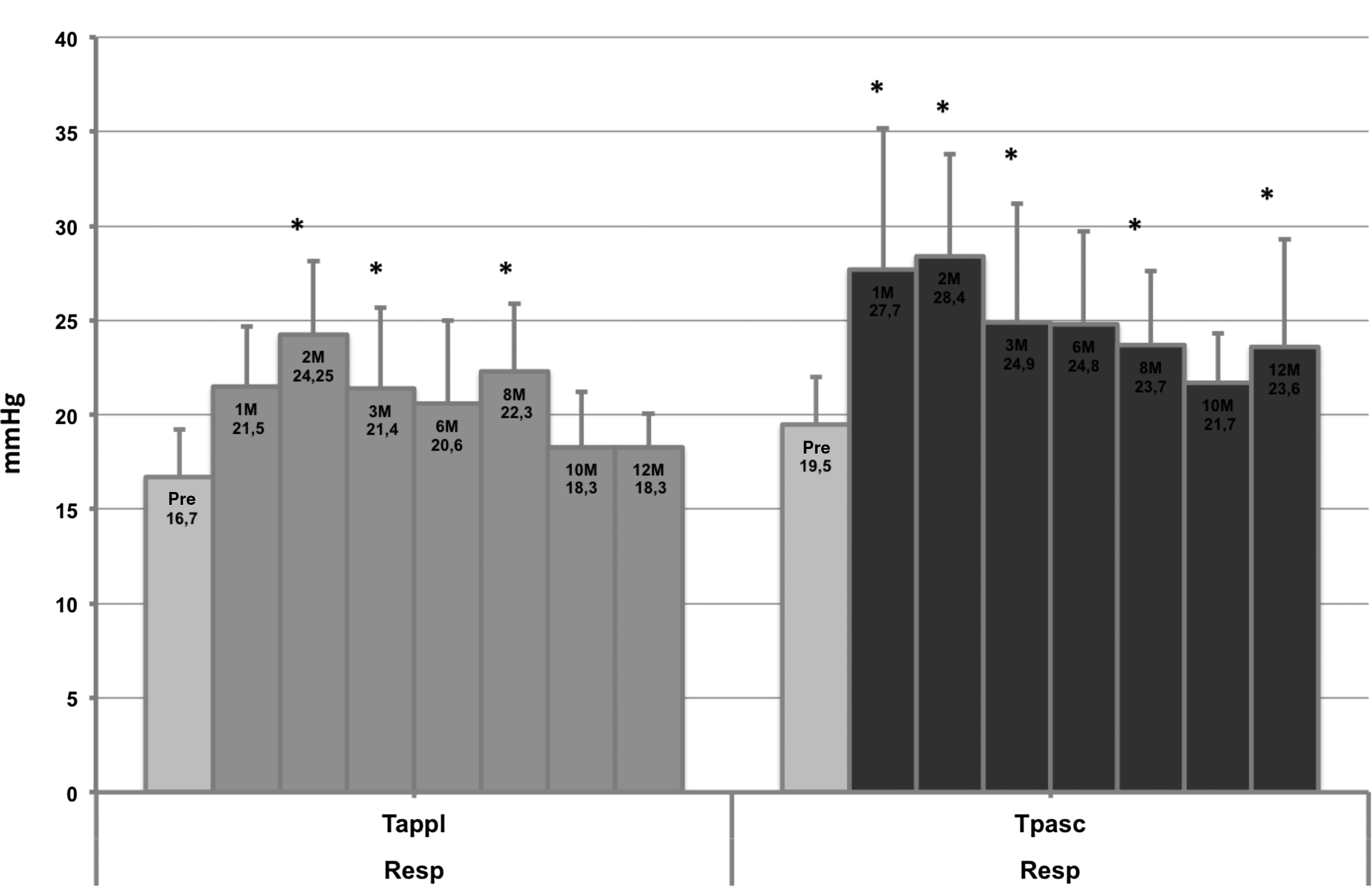
Mean intraocular pressure (IOP) of Responder (n=11) treated with dexamethasone 0.7 mg measured with Goldmann applanation tonometry (GAT) and dynamic contour tonometry (DCT) over observation period of 12 months. Bar is 95% confidence interval for the mean. *Statistical significant difference of mean IOP compared to Non-Responder (P≤0.05, paired t-test).
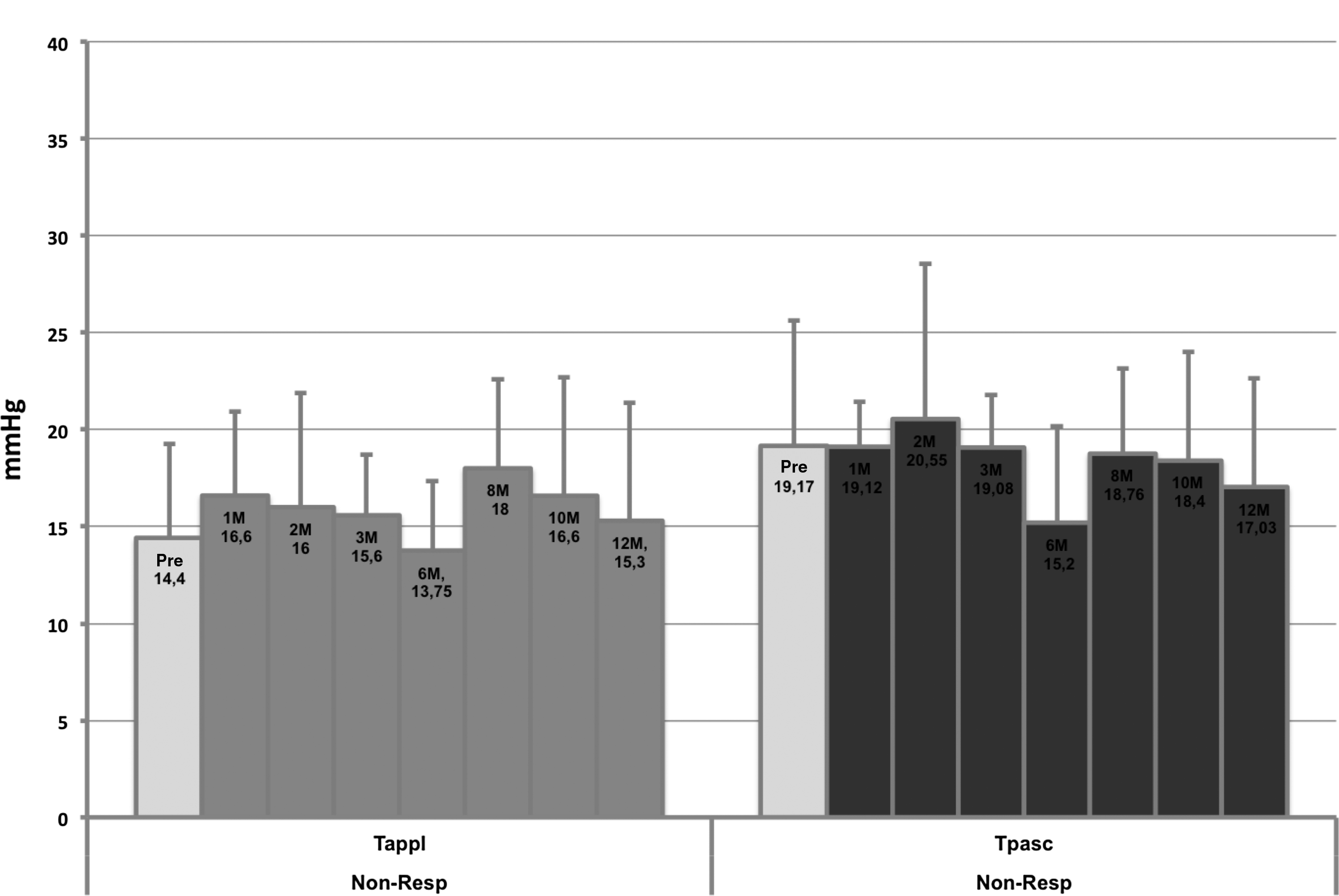
Mean IOP of Non-Responder (n=5) treated with dexamethasone 0.7 mg measured with GAT and DCT over observation period of 12 months. Bar is 95% confidence interval for the mean.
IOP difference before and after dexamethasone 0.7 mg treatment
Mean IOP difference between the dexamethasone 0.7 mg intravitreal implant treated eyes and the fellow untreated eyes is given in Fig. 5 for the group of Responders and in Fig. 6 for the Non-Responders, respectively. As indicated by the 95% confidence interval, the IOP increase was significant at observation points 1, 2, 3, and 8 months (*) in the group of Responders since the confidence interval does not include zero (Fig. 5). The IOP difference between treated and untreated eyes in the Non-Responder group was not significant at any observation point. Here the 95% confidence interval does include zero at all measurement points (Fig. 6).
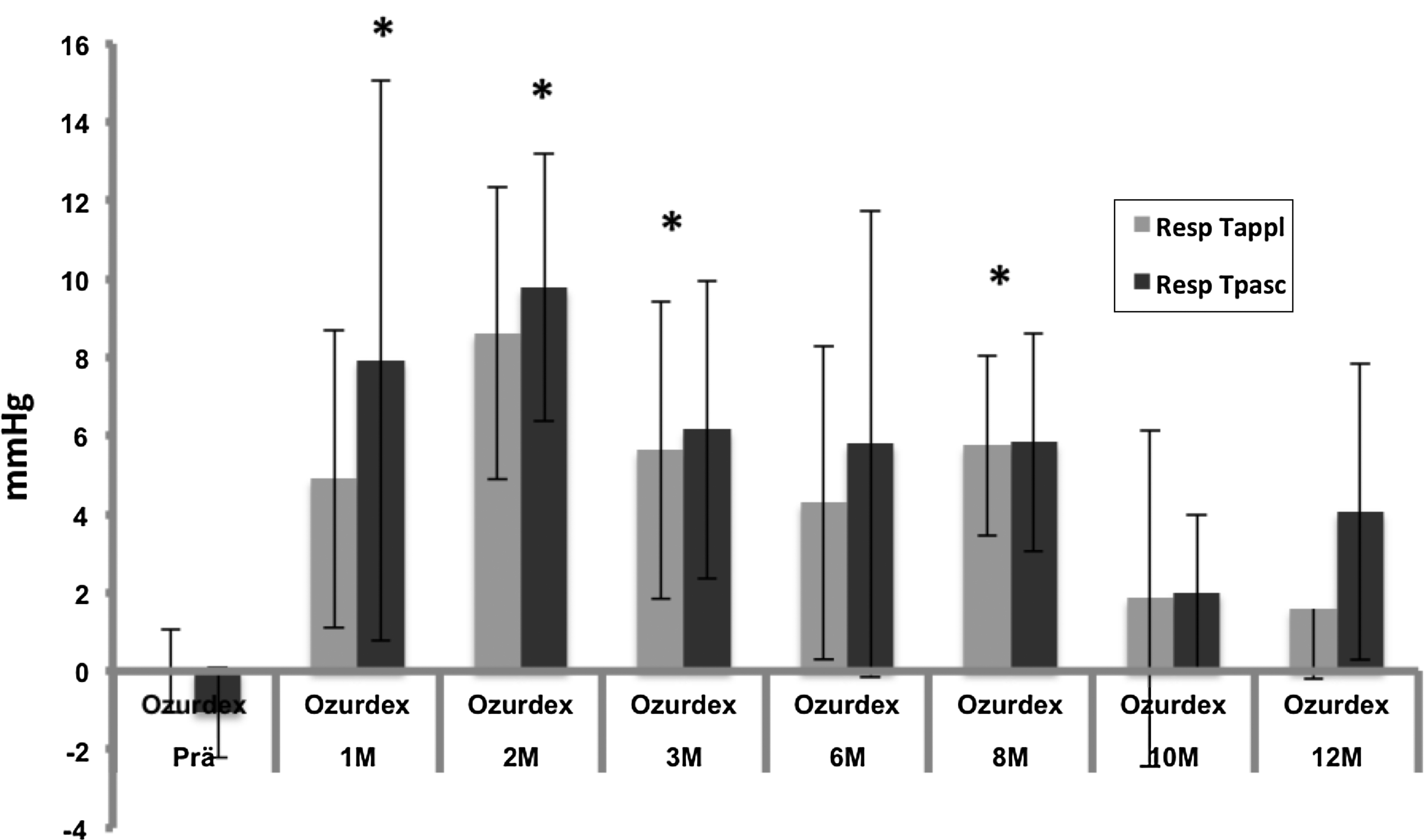
Mean IOP difference between treated and untreated eyes in Responder group (n=11). Observation period 12 months. Bar is 95% CI for the mean of IOP difference. *Statistical significant difference.
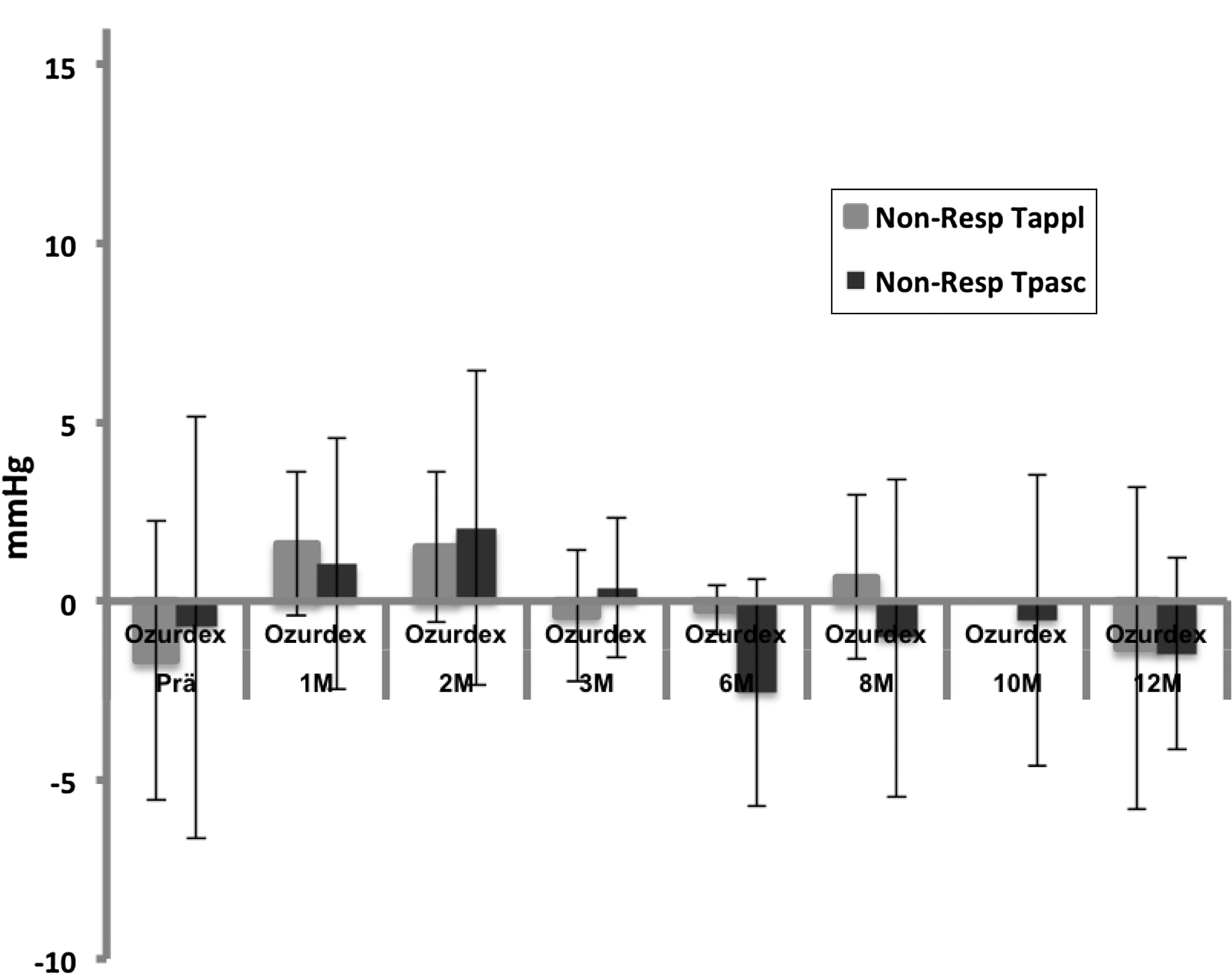
Mean IOP difference between treated and untreated eyes in Non-Responder group (n=5). Observation period 12 months. Bar is 95% CI for the mean IOP difference.
Treatment with IOP-lowering medications
Treatment with IOP-lowering eye drops (brinzolamid or dorzolamid plus timolol) was necessary in 69% of patients during the observation period. Topical antiglaucomatous treatment was ongoing in these patients at the observation point 12 months. One patient developed an increase of IOP up to 57.9 mmHg (DCT) and was treated additionally to topical treatment with intravenous and oral acetazolamide.
Adverse events
The highest IOP was 57.9 mmHg (DCT) in a patient 4 weeks after dexamethasone 0.7 mg implantation. This adverse event was treated successfully with IOP lowering oral and local medication without the need for surgical intervention. Significant cataract development was observed in phakic patients progressing from the second dexamethasone 0.7 mg injection onward. No cataract surgery was performed in these cases within the observation period of 12 months but is planned for the near future. No other adverse events, such as retinal detachment and or endophthalmitis occurred in the study population.
Discussion
Dexamethasone 0.7 mg intravitreal implant has shown in randomized clinical trials initial efficiency in the treatment of macular edema due to retinal vein occlusion.6,7,9 Similar to data published in the GENEVA study, our patients showed after a single intervention a significant BCVA improvement from baseline that lasted on average 2–4 months. However, in our population earlier reinjections were necessary in most patients with CRVO but also in 3 out of 5 patients with BRVO to maintain a visual improvement over the observation period of 12 months. Nevertheless, mean BCVA (logMAR) after 12 months of intensive treatment was 0.87, almost the same as on study entry. The recurrence rate of macular edema was considerably high (15 out of 16 patients, 94%) making retreatment necessary in almost all patients.
Still undetermined are the long-term adverse events of required repeated dexamethasone 0.7 mg injections, beyond the rigid 6-monthly interval regime of the GENEVA study, such as cataract development and secondary glaucoma. In concordance with GENEVA results, in our study population, the first injection did not cause cataract in phakic patients but from the second injection onward lens opacities increased significantly as judged with the slit lamp.
Intraocular pressure
We present here for the first time examiner-independent data on IOP after dexamethasone 0.7 mg implantation by utilizing the Pascal DCT. Even though GAT is currently the most widely used method for IOP measurement, 10 DCT has attracted much attention in recent years as a promising novel method that overcomes some limitations of applanation tonometry. In contrast to GAT, the Pascal tonometry provides direct transcorneal IOP measurements independent of central corneal thickness, corneal curvature, and is less prone to examiner dependant measurement bias.11–15 As expected, Pascal readings in our study were in mean 2–4 mmHg higher than GAT readings.16–19 However, even after correcting for this well described fact, Pascal readings detected IOP elevations more sensitive, especially at IOP values ≥25 mmHg as in 1 patient that had an IOP of 32 mmHg measured with GAT but 57.9 mmHg measured with Pascal DCT.
Similar to the results of the GENEVA study, we found a peak of IOP elevation 2 months after dexamethasone 0.7 mg injections. Even though most IOP elevations were transient and could be controlled with IOP lowering eye drops we did find indications for a higher steroid response than the published 16% in the GENEVA studies.
In our opinion, the most interesting finding of our study, aside from the relatively small sample size, is the fact that 11 out of 16 patients (69%) showed a biological response with an elevation of IOP of at least 5 mmHg to the intravitreal dexamethasone implant 0.7 mg. Furthermore, a transient raised IOP of 10 mmHg or more was documented in 50% of patients. These findings are comparable to rates of secondary glaucoma after treatment with intravitreal Triamcinolon reported by the SCORE study group of 41%.20,21 Even though it is well known that dexamethasone treatment may cause the onset of secondary glaucoma as an adverse event 22 the exact molecular mechanism of steroid–induced glaucoma is still elusive. Evidence points to excessive extracellular matrix material aggregation within the outflow channels in the trabecular meshwork tissues, which subsequently leads to increased outflow resistance.23,24 Our data indicate that, especially after repeated injections with dexamethasone 0.7 mg, the prolonged exposure of intraocular structures to the dexamethasone implant exceeds a dose-threshold that leads to alterations in the trabecular meshwork causing secondary outflow obstruction. That effect is most probable due to an accumulative effect of dexamethasone in the vitreous cavity, especially after repeated injections of the implant. This finding deserves attention and needs to be considered seriously since reinjections are clinically required frequently, in our population already after 3–4 months, to sustain a long-term treatment success. The question that remains to be clarified is whether these, in the transient majority, cases of secondary glaucoma have clinical significance.
We conclude that the long-term treatment with dexamethasone 0.7 mg should be reserved to pseudophakic patients that might for other reasons not be applicable for alternative treatments, such as monthly anti-VEGF injections. Furthermore, the rate of transient secondary glaucoma after especially repeated intravitreal injections of dexamethasone 0.7 mg might be underestimated in the 6-monthly treatment regimen of the GENEVA studies. We suggest that frequent IOP controls, preferably with DCT, should be the standard of care if dexamethasone 0.7 mg is chosen as a long-term treatment. However, to adequately address our findings further observation in a larger cohort of patients requiring multiple treatments is needed.
Footnotes
Acknowledgments
This study has been presented as an Abstract on the meeting of the German Society of Ophthalmology Annual Meeting (Deutsche Ophthalmologische Gesellschaft, DOG), Berlin September 2012, Berlin, Germany.
Author Disclosure Statement
No competing financial interests exist.