
Abstract
Abstract
Purpose:
To further evaluate the effect of intravitreal bevacizumab (IVB) for the treatment of central retinal vein occlusion (CRVO) by meta-analysis.
Methods:
Pertinent publications were identified through PubMed, EMBASE, and the Cochrane Controlled Trials Register up to January 30, 2013. Changes in central macular thickness (CMT) and best-corrected visual acuity (BCVA) were extracted at 4, 12, and 24 weeks after treatment, and a meta-analysis was carried out to compare results between groups receiving IVB and intravitreal triamcinolone acetonide (IVTA).
Results:
One randomized controlled trial and 4 comparative studies were identified and included. All of the funnel plots, the Egger's method and Begg method did not show publication bias. Our meta-analysis revealed that BCVA and CMT at 4, 12, and 24 weeks after treatment did not vary significantly between the IVB groups and IVTA groups (BCVA: at 4 weeks, P=0.27; at 12 weeks, P=0.51; at 24 weeks, P=0.64; CMT at 4 weeks, P=0.88; at 12 weeks, P=0.57; at 24 weeks, P=0.64). However, the rate of intraocular pressure rise after intravitreal injection varied significantly between the IVB groups and IVTA groups (P<0.001).
Conclusions:
Our results showed a similar improvement in BCVA and CMT among CRVO patients was obtained after intravitreal injections of both IVB, or IVTA, while the rate of IOP rise was significantly higher in the latter.
Introduction
The panoply of therapeutic possibilities increased dramatically with the development of intravitreal medical therapies, initially with the intravitreal use of triamcinolone (IVTA),4–8 followed by the intravitreal application of bevacizumab (IVB), and subsequently, the other antivascular endothelial growth factors in the recent 8 years.9–14 Although reduction of macular thickness and improvement of vision were observed after both treatments, as far as the authors were aware, no systematic reviews comparing the therapeutic effects of IVB and IVTA for CRVO have been published. It is necessary to review in greater depth, the benefits and risks of IVB and IVTA for CRVO. We have performed a meta-analysis to review the literature to compare the effect and safety profiles of both IVB and IVTA, in treating patients with CRVO.
Methods
Two reviewers independently searched the following electronic databases: PubMed, EMBASE, and the Cochrane Controlled Trials Register up to 30 January 2013. Free text and thesaurus terms, including “bevacizumab,” “triamcinolone acetonide,” “central retinal vein occlusion,” and “macular edema” were used. When titles and/or abstracts met the objectives, the full article would be retrieved. A manual cross-reference search for bibliographies of relevant articles was also conducted. The inclusion criteria for references were (1) all published studies comparing IVB versus IVTA for CRVO, including randomized controlled trials (RCTs) and high-quality comparative studies; and (2) all articles, where pre- and post-treatment visual acuity and the macular thickness were measured and recorded. There was no language restriction. For the publications from the same group of authors, only the article with the largest number of patients was used. The selected articles were then critically appraised by 2 reviewers, who independently assessed their quality using the modified Jadad score table. 15 Parameters judging the methodological quality included allocation concealment, the method of intervention allocation, the degree of masking, and the completeness in subject follow-up. The postoperative outcome parameters included best-corrected visual acuity (BCVA) and central macular thickness (CMT).
The following data from the original articles were being extracted: first author and year of publication; study site; study design; sample size and age of the participants; treatment method and follow-up duration; numbers lost to follow-up; and treatment outcome in terms of BCVA and CMT. Data extraction was conducted by the 2 reviewers independently, and discordance was resolved through discussion until 100% agreement was reached.
A meta-analysis on the effect of IVB or IVTA on macular edema secondary to CRVO was performed using Cochrane Review Manager (RevMan; version 5.0 software). The treatment effect was estimated by means of weighted mean deviation (WMD) in BCVA and CMT. The incidence of adverse events such as ocular hypertension was evaluated by the risk ratio (RR). Random effect models were used for the meta-analysis, and were verified using the Q test (P<0.10 was considered to indicate statistically significant heterogeneity) and the I2 statistic (values of 25%, 50%, and 75% are considered to represent low, medium, and high heterogeneity, respectively). Publication bias was assessed by visually inspecting a funnel plot.
Results
A total of 69 articles were identified, of which 55 articles were excluded due to the above-mentioned reasons. A full review was performed for the remaining 14 articles. Nine out of 14 were further excluded due to similarities with previous studies from the same group of authors (Fig. 1). Five articles published between 2005 and 2012 were finally included into the meta-analysis (Table 1).9,11–14

Flowchart of literature search and study selection.
IVB, intravitreal bevacizumab; IVTA, intravitreal triamcinolone acetonide.
There were one RCT and 4 nonrandomized controlled studies (Table 1). The sample sizes varied from 18 to 75 subjects, and mean follow-up durations varied from 9 to 12 months. The treatment outcome estimates were provided for a total of 92 eyes in the IVB group and 103 eyes in the IVTA group. In all studies, distribution of age, gender, and history of CRVO did not vary significantly between the IVB group and the IVTA group.
Four studies reported data on BCVA at 4 weeks after the initial treatment. The BCVAs were converted to logarithm of the minimum angle of resolution (logMAR) vision and were summarized by means of meta-analysis (I2=0%). The BCVA at 4 weeks after IVB treatment did not vary significantly when compared to those using IVTA (WMD=0.06; 95% CI: −0.04–0.16; P= 0.27). All the 5 studies reported data on BCVA at 12 weeks after the initial treatment, and demonstrated low heterogeneity (I2=0%). The improvement in BCVA did not vary significantly between the IVB and IVTA groups (WMD=0.03; 95% CI:−0.06–0.13; P= 0.51). Four studies reported data on BCVA at 24 weeks after the initial treatment, and showed low heterogeneity (I2=0%). Again, the improvement in BCVA did not vary significantly between the IVB and IVTA groups (WMD=0.02; 95% CI: −0.08–0.13; P= 0.64) (Table 2) (Fig. 2).
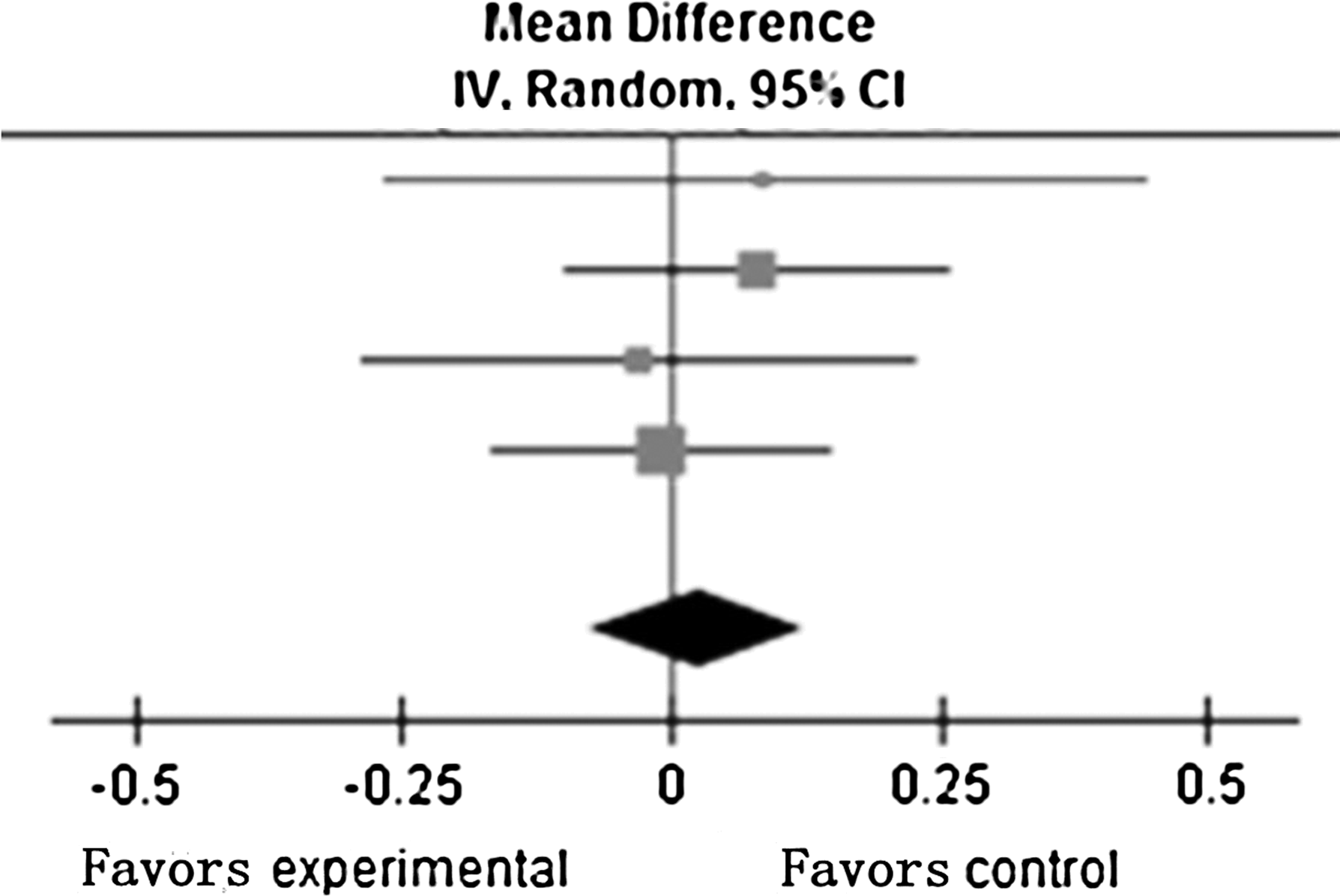
Comparison of best-corrected visual acuity at 24 weeks after initial treatment between intravitreal injection of bevacizumab (IVB) groups and intravitreal injection of triamcinolone acenotide (IVTA) groups in published studies (from top to bottom): Ding et al., 12 Guthoff et al., 37 Lim et al., 11 and Tao and Jonas. 5
Heterogeneity: Tau 2 =0.00; χ2=0.84, df=3 (P=0.84); I2=0%.
Test for overall effect: Z=0.46 (P=0.64).
Four studies reported data on CMT at 4 weeks after the initial treatment. Low heterogeneity between studies was detected (I2=0%). Changes in CMT at 4 weeks after IVB did not vary significantly as compared to those using IVTA (WMD=−4.97; 95% CI: −71.41–61.47; P= 0.88). All 5 studies reported data on CMT at 12 weeks after the initial treatment, and demonstrated low heterogeneity (I2=32%). Changes in CMT also did not vary significantly between the IVB and IVTA groups (WMD=20.29; 95% CI: −50.53–91.12; P= 0.57). Four studies reported data on CMT at 24 weeks after the initial treatment, but showed high heterogeneity (I2=58%). Changes in CMT at 24 weeks after IVB treatment did not vary significantly as compared to those that received IVTA (WMD=67.75; 95% CI: −35.30–170.79; P= 0.20) (Table 3) (Fig. 3).

Heterogeneity: Tau 2 =6177.35; χ2=7.17, df=3 (P=0.07); I2=58%.
Test for overall effect: Z=1.29 (P=0.20).
All 5 studies reported complications during the follow-up period, such as intraocular pressure (IOP) rise. No patients had IOP rise after IVB, but IOP rise after IVTA was reported to be as high as 50.5% in one study (52/103). All cases with IOP rise after injection were controllable by medication. Low heterogeneity between studies was detected (I2=0%). Random-effects model analysis demonstrated a significant difference between IVB and IVTA in this regard (RR, relative risk=0.06; 95% CI: 0.02–0.22; P<0.001) (Table 4) (Fig. 4).
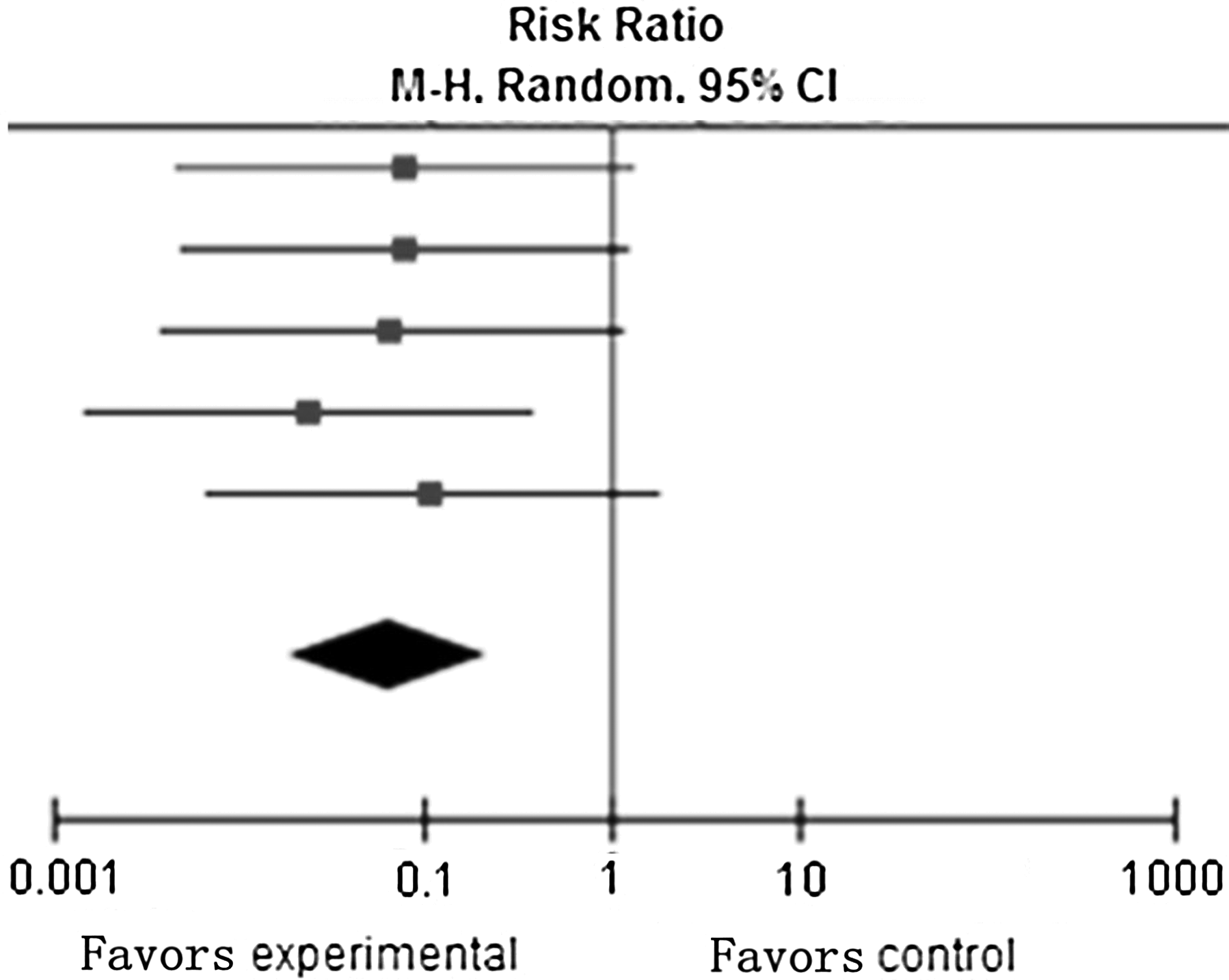
Heterogeneity: Tau 2 =0.00; χ2=0.77, df=4 (P=0.94); I2=0%.
Test for overall effect: Z=4.35 (P<0.0001).
Based on funnel plots, no obvious evidence of publication bias was found for the treatment outcome estimates (BCVA and CMT at 12 weeks after initial treatment) (Figs. 5 and 6). Since the number of enrolled studies was low, additional tests (the Egger's Method, and the Begg's method) were used to measure publication bias, but none was able to detect any (BCVA at 12 weeks after initial treatment: the Egger's method: P= 0.14, the Begg's method: P= 0.09; CMT at 12 weeks after initial treatment, the Egger's method: P= 0.26, the Begg's method: P= 0.81).
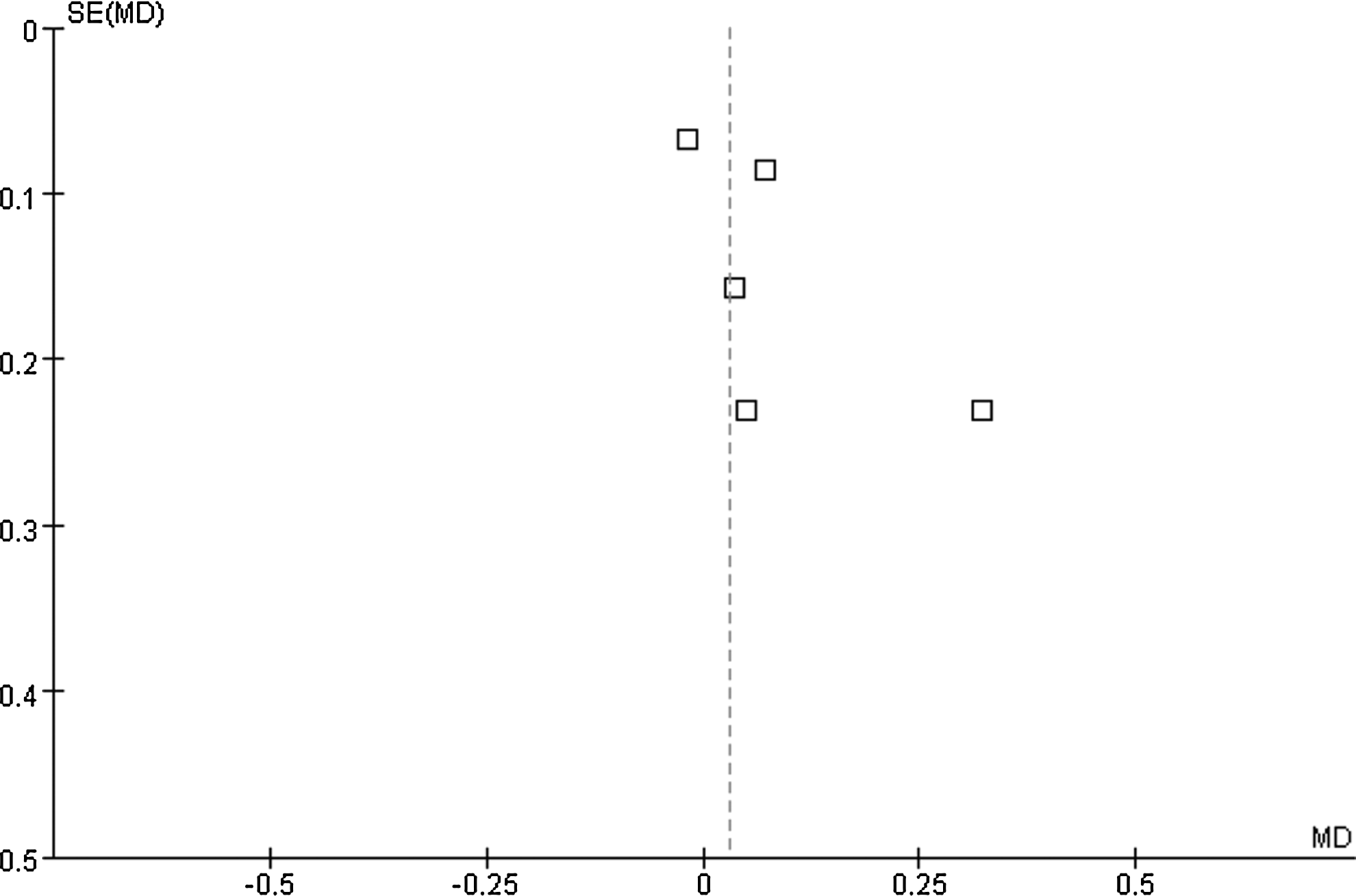
Funnel plots with respect to best-corrected visual acuity at 12 weeks after initial treatment.

Funnel plots with respect to CMT at 12 weeks after initial treatment.
Discussion
Our meta-analysis failed to detect any statistical significant difference between the IVB and the IVTA groups, in terms of BCVA measured at 4, 12, and 24 weeks after baseline (at 4 weeks: P= 0.27; at 12 weeks: P= 0.51; at 24 weeks: P=0.64). Similarly, the difference in reduction in CMT between the 2 groups also did not vary significantly at 4, 12, and 24 weeks (at 4 weeks: P= 0.88; at 12 weeks: P= 0.57; at 24 weeks: P=0.64). However, the rates of IOP rise were significantly higher in the IVB groups than the IVTA groups (P<0.001).
There have been several studies looking into the effect of bevacizumab in macular edema secondary to CRVO. The common results were improvements in BCVA, reduction in CMT on optical coherence tomography (OCT), or improvement in electroretinographic outcomes. At the same time, common shortcomings were the short-term efficacy of IVB, and the high recurrence rates of macular edema after the wearing off of its effect. While the dosage varied from 1.25 to 2.0 mg, there is no difference in terms of the outcomes.16–23 On the other hand, similar improvements in BCVA and CMT after IVTA for CRVO were also observed in some other reports.4,5,8,24–30 After IVTA, IOP readings higher than 21/30/35/40 mmHg, was reported in as high as 36.2/8.5/4.2/1.5% of patients, respectively. 5 The International Intravitreal Bevacizumab Safety Survey gathered adverse events after IVB from doctors around the world using the internet and found that all ocular and systemic side effects were below 0.21%, including corneal abrasion and lens injury. 31
These results were in agreement with other comparative studies between IVB and IVTA for the treatment of branch retinal vein occlusion (BRVO).32–35 In a study by Kwon et al., both IVTA- and IVB-treated groups showed improvement after injections for BRVO, and there was no significant difference in the visual outcome and macular thickness at 6 months. 32 Considering the potential risks with IVTA injections, some authors recommended prescheduled repeated IVB injections for BRVO cases. 33
The findings in our meta-analysis were partly in disagreement with comparative studies between IVB and IVTA for diabetic macular edema (DME). A recent published meta-analysis showed that IVTA was more effective in improving BCVA than IVB in DME, while reduction in CMT was unsustainable. 36
The main limitation of this study was that the number of included studies and the total number of subjects were relatively low. This probably reflected the strict inclusion and exclusion criteria. The included studies, however, originated from several regions, and all except one 9 led to similar conclusions in the outcomes measured.
In conclusion, our meta-analysis showed a similar improvement BCVA and CMT in CRVO patients after intravitreal injections of either IVB or IVTA, but IVB appeared to be devoid of unfavorable IOP elevation after injections.
Footnotes
Acknowledgment
This study was supported by the Program for New Century Excellent Talents in University (No. NCET-12-0010).
Author Disclosure Statement
J.B.J.: Consultant for Allergan, Inc., Merck & Co., Inc., Alimera Co., and patent holder with CellMed AG, Alzenau, Germany; all other authors: none.