
Abstract
Abstract
Purpose:
To compare the efficacy and safety of bimatoprost 0.01% with the fixed combination travoprost 0.004%/timolol 0.5% in subjects with stable intraocular pressure (IOP) control on latanoprost and timolol.
Methods:
This was a randomized, prospective, investigator masked, crossover study comparing bimatoprost 0.01% with travoprost/timolol in 40 subjects diagnosed with primary open-angle glaucoma. Subjects were randomized to bimatoprost 0.01% qpm or travoprost/timolol qam and followed for 12 weeks, at which time they were crossed over to the alternate medication and followed for another 12 weeks. Intraocular pressure and hyperemia (rated on a standardized, 5-point photographic scale) were evaluated as change from baseline to 12 weeks following each therapy, and subject preference was elicited at the end of the study.
Results:
Both treatments were well tolerated and the majority of patients achieved effective IOP control relative to baseline. After 12 weeks of treatment, mean reductions from baseline IOP were −1.68 mmHg OD (right eye) and −1.58 mmHg OS (left eye) with bimatoprost and −0.45 mmHg OD and −0.53 mmHg OS with travoprost/timolol, although the differences between drugs were not statistically significant. Hyperemia scores were significantly higher with the fixed combination of travoprost/timolol than bimatoprost 0.01% as measured at 8 am (both P<0.01). Subject preference at the end of the study was more than 3 to 1 in favor of bimatoprost, with most citing greater tolerability.
Conclusion:
Bimatoprost 0.01% and travoprost/timolol are both effective at reducing IOP in subjects with stable IOP control on latanoprost and timolol, but bimatoprost 0.01% is associated with less hyperemia.
Introduction
P
The efficacy of IOP lowering agents as adjunctive therapy may depend on the particular combination of agents.4,5 Currently, beta-adrenergic antagonists are the most common IOP lowering agents used adjunctively with the PGAs. Studies have also evaluated alpha-adrenergic agonists and carbonic anhydrase inhibitors as adjuncts to PGAs.6,7 Until recently, the PGA most commonly prescribed as initial monotherapy in Canada has been latanoprost. If after a period of time, target IOP cannot be maintained, it has been common to see the addition of a beta blocker with a formulation that allows for a qam prescribing frequency or, more recently, to switch within class of the PGA to one believed to have improved IOP lowering efficacy.
Recently, several generic substitutes for latanoprost have been introduced, and concerns have arisen about the comparative efficacy and safety of these products.8,9 Compounding the issue has been the supply shortage of generic timolol maleate 0.5% XE. Moreover, it is desirable to move patients to a once daily dosing regimen when possible because it may be associated with improved adherence to treatment and patients prefer it.10,11 These events have resulted in shifts in the treatment regimens for patients receiving latanoprost and timolol for IOP control.
Among the many options for these patients are conversions to the fixed combination travoprost 0.004%/timolol 0.5% or the monotherapy with bimatoprost 0.01%. The logic for travoprost/timolol is the ability to continue with the PGA/beta blocker combination, but with the compliance and other advantages of a monotherapy regimen. The choice of bimatoprost 0.01% monotherapy comes from data indicating that some patients develop tachyphylaxis with long-term beta-blocker therapy, as well as multiple studies indicating the superior efficacy of bimatoprost over that of latanoprost.12–14 Given that both travoprost/timolol and bimatoprost 0.01% monotherapy are viable options for patients switching from timolol maleate 0.5% XE and latanoprost 0.005%, several questions arise: (1) How do the travoprost/timolol and bimatoprost 0.01% regimens compare to one another in terms of safety, efficacy, and patient preference? (2) How do the travoprost/timolol and bimatoprost 0.01% regimens compare to the timolol and latanoprost regimen? The present crossover study was undertaken to address these questions.
Methods
Study design and subjects
This was an investigator masked, prospective, randomized, parallel group, crossover study comparing bimatoprost (Lumigan® RC 0.01% ophthalmic solution; Allergan, Inc., Irvine, CA) and travoprost/timolol (DuoTrav® 40; Alcon Canada, Inc., Mississauga, Ontario, Canada) in patients with primary open-angle glaucoma (POAG). The study was conducted at a single center in Barrie, Ontario, Canada from January 11, 2012 to September 26, 2012 and was approved by an Institutional Review Board (Institutional Review Board Services, Aurora, Ontario, Canada).
Subjects were adults with POAG who had been treated with latanoprost 0.005% (Xalatan®; Pfizer Canada, Inc., Markham, Ontario, Canada) qhs and timolol maleate 0.5% qam continuously for at least 6 weeks before study enrollment. American Academy of Ophthalmology criteria were used for the diagnosis of POAG (evidence of optic nerve damage, adult onset, open anterior chamber angles, absence of other known explanations). 15 Subjects must have had no more than a 5 mmHg difference between eyes in baseline IOP if both eyes were eligible for the study and had best corrected Snellen visual acuity of 20/100 or better in both eyes. Subjects were ineligible for the study if they had secondary OAG, closed-angle glaucoma, or neovascular glaucoma or if they previously undergone incisional surgery or refractive surgery. Subjects were also excluded if they had any systemic or abnormal ocular conditions or symptoms that could have interfered with the trial (e.g., ocular inflammation, previous glaucoma laser surgery) or would contraindicate participation in the trial (e.g., known sensitivity/allergy to any of the study medications or their components). Women of childbearing potential were required to have a negative urine pregnancy test at study entry, could not be lactating, and must have been willing to use effective contraception during the study.
All subjects provided informed consent and signed an authorization for the use and disclosure of health information for research before any study-related procedures. Subjects received a small monetary compensation ($50 for enrollment+$30 for each of the 4 follow-up visits for a total of $170 for full completion of the study) to defray travel and other incidental costs of participating in this study. This study conformed to the Declaration of Helsinki.
Study procedures and outcome measures
Clinic patients diagnosed with OHT or glaucoma stable on latanoprost and timolol for 6 weeks or more were evaluated at a screening visit to determine whether they satisfied the inclusion/exclusion criteria. Patients who were eligible were invited to participate in the study, and those who agreed to enroll were randomized to receive either travaprost 0.004%/timolol maleate 0.5% qam or bimatoprost 0.01% qpm. Randomization was performed using the random number generator in Microsoft Excel. Subjects were instructed to instill 1 drop of timolol maleate/travoprost into each eye at 8:00 am±15 min or 1 drop of bimatoprost 0.01% into each eye at 8:00 pm±15 min daily. After 12 weeks of treatment, subjects were crossed over to the opposite medication for another 12 weeks. No washout period was included before enrollment or between crossover periods because the study was designed to mimic actual clinical practice for patients who needed to be switched from latanoprost and timolol to another regimen, while maintaining their target IOP. Subjects were not masked to treatment.
Outcome measures were evaluated at baseline and 6 and 12 weeks after beginning each medication. Six weeks was selected as the first follow-up time point to allow the previous drug(s) to be completely cleared from the system. At baseline and each follow-up visit, IOP was measured using a tonometer affixed to a slit lamp with the patient seated. Two consecutive IOP measurements were taken in each eye and a third measurement was taken if the first 2 differed by more than 2 mmHg; the mean of the 3 values was retained as the final IOP if the first 2 differed by more than 2 mmHg. In addition, at baseline and at each follow-up visit, ocular hyperemia was rated on a photographic 5-point grading scale as follows: 0=none: normal, +0.5=trace: trace flush reddish pink, +1=mild: mild flush reddish color, +2=moderate: bright red color, +3=severe: deep, bright, diffuse redness. 14 At all study visits, each subject's IOP and hyperemia measurements were taken before instillation of the study medication; follow-up measurements were performed at ∼8:00 am (±30 min) for every patient throughout the study.
At each follow-up visit, subjects were asked about adverse experiences that may have occurred since a previous visit. All adverse events were recorded, along with their severity, action taken, and relationship to the study medication(s). Best corrected visual acuity and concomitant medications were also documented at each visit. At the end of the study, subjects were asked which medication they preferred and why.
Statistical analyses
Demographic and adverse event analyses included all subjects who completed the screening/baseline visit. IOP and hyperemia analyses included all subjects who completed the study. Data were pooled across the treatment order such that data from all subjects were included in the analysis for each medication regardless of which medication they received first. Order effects for IOP data were assessed using 2-tailed t-tests for unequal variances to compare change from prestudy baseline to week 24 (end of study) values for the 2 drugs for each eye; the same procedure was used for hyperemia data except that Wilcoxon rank sum tests were conducted. Pooled data analyses assessing differences between study drugs were conducted on change from baseline data, with the prestudy baseline used for the first arm of the study and the week 12 data used as the baseline for the second arm of the study.
Pooled IOP data were assessed using paired, 1-tailed t-tests conducted separately for each eye based on the hypothesis that bimatoprost would produce greater reductions in IOP than travoprost/timolol. Pooled hyperemia data were analyzed using paired, 1-tailed Wilcoxon rank sum tests conducted separately for each eye based on the hypothesis that bimatoprost would produce less hyperemia than travoprost/timolol. These analyses were conducted on change from baseline data, with the prestudy baseline used for the first arm of the study and the week 12 data used as the baseline for the second arm of the study.
Paired t-tests were used to compare IOP data (which was normally distributed) and Wilcoxon rank sum tests were used to compare hyperemia data (which was not normally distributed) for each drug and each eye at baseline versus each of the follow-up time points to evaluate the effects of both drugs compared to latanoprost and timolol (the prestudy drug regimen). These tests were 1-tailed based on the predictions that both study drugs would be associated with reduced IOP and increased hyperemia from prestudy baseline.
Microsoft Excel was used for all analyses. The significance level for all analyses was set at P≤0.05; P values were not adjusted for multiple comparisons because only 2 outcome variables were assessed.
Results
Subjects and disposition
A total of 45 patients met the inclusion/exclusion criteria for this study and were invited to enroll. Five patients declined because they were not available for the entire duration of the study (6 months) and 40 subjects enrolled. Of these 40 subjects, 38 completed the entire study and 2 discontinued due to adverse events (both presented with intolerable hyperemia while on travoprost/timolol, with one in each arm of the study). Before study enrollment, 38 of the subjects had been treated with timolol maleate gel (Timoptic XE®) and 2 had been treated with timolol bid; all subjects had also been treated with latanoprost 0.005% qhs (Xalatan) as per the inclusion criteria. Subject characteristics are shown in Table 1. All subjects included in the study had evidence of POAG.
SD, standard deviation.
Intraocular pressure
Mean IOP levels at the prestudy baseline were 16.1 to 16.6 mmHg for both eyes, and were not significantly different between groups (OD, (right eye), P=0.65; OS, (left eye), P=0.84). No order effects were detected for IOP data (OD, P=0.37; OS, P=0.42). Based on the pooled data set, travoprost/timolol treatment led to a mean decrease from baseline of −0.53 mmHg in the right eye and −0.86 in the left eye after 6 weeks of treatment and −0.45 mmHg in the right eye and −0.53 in the left eye after 12 weeks of treatment (Fig. 1). Bimatoprost treatment resulted in a mean decrease from baseline of −1.55 in the right eye and −1.66 in the left eye after 6 weeks of treatment and −1.68 in the right eye and −1.58 in the left eye after 12 weeks of treatment (Fig. 1). Although the decreases were numerically greater with bimatoprost than travoprost/timolol in both eyes at both time points, they were not statistically significant (6 weeks: OD, P=0.11; OS, P=0.16; 12 weeks: OD, P=0.08; OS, P=0.13; Fig. 1).

Mean changes from baseline intraocular pressure (IOP) (–SEM) following treatment with travoprost/timolol (Trav) or bimatoprost (Bimat) based on the pooled data set. Asterisks indicate significant decreases from baseline IOP (P<0.05). OD, right eye; OS, left eye.
The decreases from baseline IOP were statistically significant in both eyes after 6 and 12 weeks of bimatoprost treatment (OD, P<0.001; OS, P<0.001; Fig. 1). However, the decrease from baseline IOP after travoprost/timolol treatment was significant only in the left eye after 6 weeks of treatment (OD, P=0.20; OS, P=0.04; Fig. 1).
Hyperemia
Median hyperemia scores at baseline were 0.5 (trace flush reddish pink) for both groups and both eyes, and were not significantly different between groups (OD, P=0.73; OS, P=0.57). No order effects were observed for hyperemia data in the left eye (P=0.27), but significant order effects were observed in the right eye (P=0.04). Between-group comparisons based on the pooled data showed that hyperemia scores were significantly lower with bimatoprost than travoprost/timolol in both the right eye (P=0.0016) and left eye (P<0.01) (Fig. 2). The majority of subjects showed either no change in hyperemia after treatment with either medication, or a slight increase or decrease of 0.5 points on the hyperemia scale (Table 2).
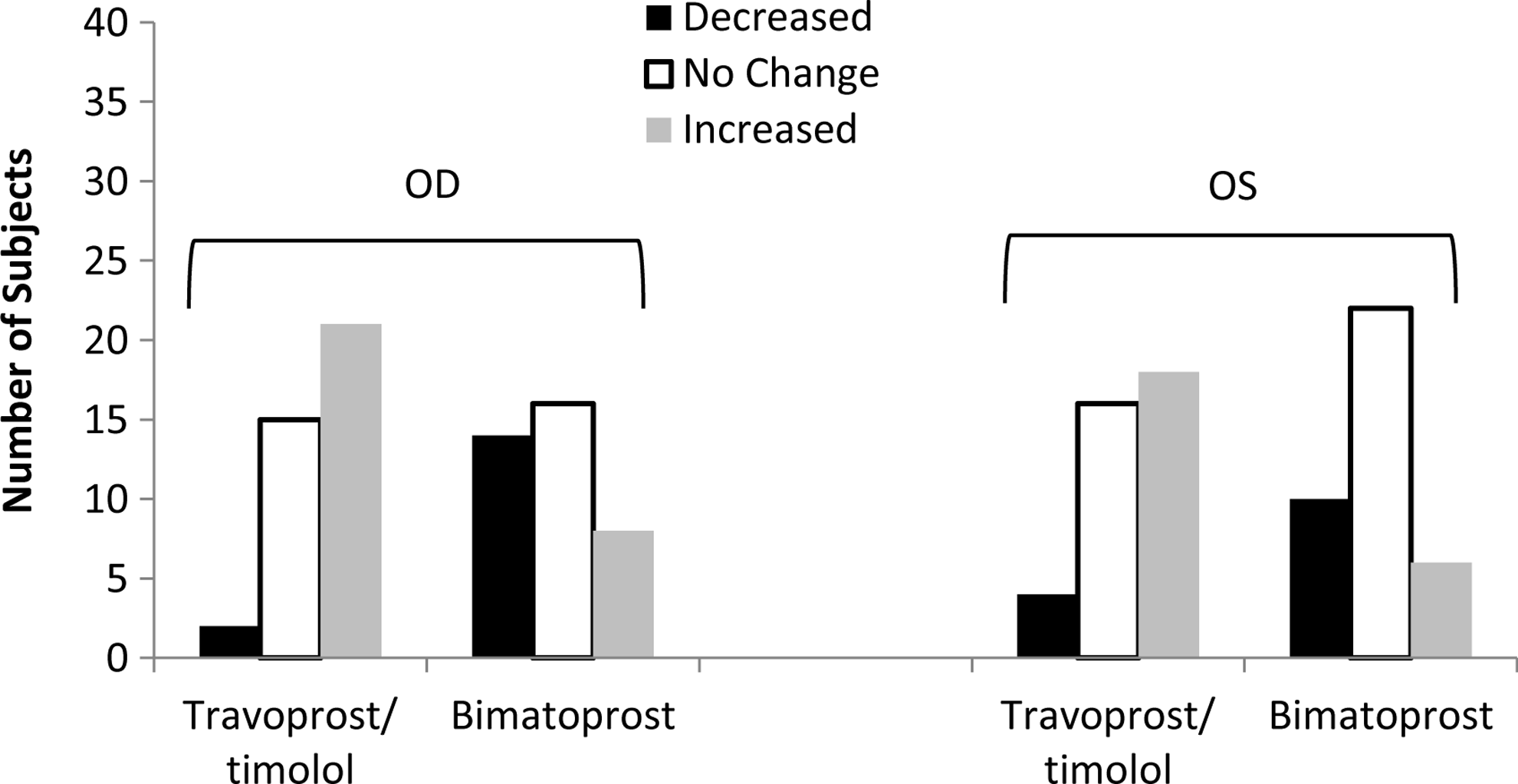
Number of subjects showing an increase, decrease, or no change in hyperemia scores following 12 weeks of treatment with travoprost/timolol or bimatoprost based on the pooled data set.
OD, right eye; OS, left eye.
Subject preference
At the end of the study, the investigator was unmasked and subjects were asked which of the 2 regimens they preferred and why. Of the 38 subjects who completed the study, 28 preferred bimatoprost, with 23 reporting that it was more tolerable with less irritation, drying, and redness, and 5 indicating preference for the evening dosing schedule. In contrast, only 9 subjects preferred the fixed combination of travoprost/timolol, with 8 indicating preference for the morning dosing schedule and one indicating that it was more tolerable.
Adverse events
Two subjects reported adverse events during the study, both of which were intolerable hyperemia that required study discontinuation. Upon unmasking, both subjects were found to be on the fixed combination travoprost/timolol; one subject discontinued 2 weeks into the first arm of the study and the other discontinued 2 weeks into the second arm of the study.
Best corrected visual acuity and concomitant medications
Best corrected visual acuity was unchanged in all subjects in the study except the 2 that were removed from the study due to adverse events, where there was a 1+ line decrease in visual acuity associated with the hyperemia. Neither of these subjects had evidence of toxic keratitis; however, both showed hyperemia of the lid margin and conjunctiva and experienced tearing and discomfort. Whether the medication increased pre-existing, but subclinical ocular surface disease, or created an unstable tear film in these patients was not determined. None of the subjects reported any changes in concomitant medications during the study.
Discussion
The relative success of medical therapy for OHT and OAG is influenced by many factors. The timing of the initial diagnosis and the stage of disease affect the ability of the optic nerve to resist further progression of damage. The initiation of proper medical therapy following accepted treatment algorithms with the goal of IOP reduction matched to the stage of the disease has been shown to minimize disease progression. Finally, patient adherence to the treatment regimen, education related to drop instillation, simplification of the drop(s) frequency, and tolerability of the drops themselves are believed to have a significant effect on the maintenance of IOP reduction and disease outcome. 16
The present study was initiated based on a transient loss of access to timolol maleate 0.5% XE and the change to one of several generic versions of latanoprost. We and others have observed variability in the generic formulations of latanoprost that may manifest as reduced tolerability and/or IOP lowering effects.8,17 In a laboratory study that used liquid chromatography–tandem mass spectrometry to evaluate drug levels in several glaucoma medications, 2 versions of generic latanoprost were found to contain 10% greater levels of the active ingredient than their labeled values. 9 In contrast, the amount of active ingredient in the name-brand latanoprost was within the labeled range. Moreover, exposure of the generic latanoprost products to 25°C for 30 days resulted in a significant loss of active ingredient that was not seen with the name-brand product. It is possible that these variations may affect the clinical response to generic latanoprost formulations.
In addition to the problems that have been observed with generic glaucoma medications, patients on a regimen of timolol maleate 0.5% XE and latanoprost are required to instill drops twice daily, which is not optimal for promoting adherence. Indeed, medication regimen and situational/environmental factors are the most common reasons that patients cite for lack of adherence to treatment. 18 In an attempt to mitigate the drawbacks associated with a twice daily regimen and the variability associated with generic latanoprost, patients were switched to once daily treatment with either bimatoprost 0.01% or travoprost/timolol.
In the present study, no statistically significant differences between medications were observed in IOP at either of the follow-up time points, although the reductions with bimatoprost 0.01% were numerically greater than those of travoprost/timolol at both 6 and 12 weeks. Previous studies comparing bimatoprost 0.03% with travoprost 0.004% have generally found greater IOP reductions with bimatoprost, 19 and no significant differences have been found in IOP reductions between bimatoprost 0.03% and 0.01%. 14 In a recent observational study that evaluated IOP following a change in glaucoma medications, patients switched to bimatoprost 0.01% from travoprost 0.004% showed significantly greater reductions in IOP levels after 12 weeks of treatment (Crichton, A.C., 2012).
The present study did find differences between the 2 medications in hyperemia, with scores significantly higher after 12 weeks of travoprost/timolol than 12 weeks of bimatoprost 0.01%. Although most subjects showed no or only minimal changes in hyperemia scores (±0.5 points), 6 subjects showed at least a 1-point worsening of hyperemia scores following 12 weeks of travoprost/timolol compared with only 1 subject following 12 weeks of bimatoprost 0.01%. Additionally, 2 subjects treated with travoprost/timolol discontinued the study due to intolerable hyperemia. Subject preferences generally mirrored the hyperemia results, with 23 subjects reporting that they preferred bimatoprost due to less irritation, drying, and redness and only 1 subject indicating a preference for travoprost/timolol based on greater tolerability.
If the observed differences in hyperemia between the 2 glaucoma therapies affected the tolerability of the medications, then even in a short study such as this, adherence to treatment may have been altered. Reduced adherence to the fixed combination of travoprost/timolol due to hyperemia could explain the numeric differences in IOP lowering between the 2 therapies, although these were not statistically significant.
Additionally, there may be an advantage to a single medication therapy with the avoidance of a beta blocker if the efficacy is similar. The beta blocker can be associated with stinging on instillation, which may affect tolerability; there is also the possibility of allergy over time to this medication. Systemic effects on the cardiovascular and respiratory systems are also possible, 20 with the potential for heart irregularities and aggravation of reactive airway diseases.
This study has several limitations. Subjects were not masked to treatment and thus could have unintentionally biased the results. Additionally, the study population may not have been large enough to detect differences between the 2 drugs in IOP lowering effects even with the crossover design.
A washout period was not included because the study was designed to resemble actual clinical practice. Moreover, subjects were under good control at the initiation of the study and the outcome variables were measured after 6 and 12 weeks of treatment with each medication. This duration was believed to be adequate to allow for the washout of the previous drug(s) effect and reflect a steady state on the new regimen.
Finally, IOP was measured at only one time during the day, at 8 am (±30 min). This single time point was selected because it was convenient for patients and indeed follow up was 100%. However, the different times of drug administration for the 2 regimens (fixed combination in the morning and bimatoprost in the evening) meant that the outcome measures were assessed at different intervals postinstillation. That is, measurements were taken ∼12 h after bimatoprost administration (assuming an 8 pm instillation) and ∼24 h after the fixed combination (just before the morning instillation). Given that prostaglandins exhibit peak effects between 8 and 12 h, the IOP measurement may have slightly favored bimatoprost and the hyperemia measurement may have slightly favored the fixed combination. Although no significant differences were noted between improvements in IOP with the 2 regimens, the fixed combination was associated with slightly greater hyperemia than bimatoprost even though the 8-am follow-up time should have favored it.
In summary, the present study has demonstrated that patients initially controlled on latanoprost and timolol can be switched to either bimatoprost 0.01% or the fixed combination of travoprost/timolol with the advantage of further IOP lowering that was statistically significant for bimatoprost. Bimatoprost 0.01% was better tolerated in this study population and, consequently, was preferred over travoprost/timolol, but both medication regimens were well tolerated.
Footnotes
Acknowledgments
The author acknowledges the assistance of Nathalie Stiévenart, MS, for statistical support and Mary Ann Chapman, PhD, for manuscript editing.
Author Disclosure Statement
This study was partially funded by a grant from Allergan, Inc. Dr. Nixon is a consultant for Allergan, Inc.