
Abstract
Abstract
Purpose:
To compare same-day pain control and safety of 2 different anesthetic gels utilizing 5% and 2% lidocaine gel. Main outcome is to determine whether 5% lidocaine gel is more effective in decreasing pain during conjunctival clamping compared to 2% lidocaine gel 5 and 10 min after gel application.
Methods:
This is a prospective, randomized double-blind clinical trial. Patients were randomized to receive 2% or 5% lidocaine gel in each eye. Discomfort during the gel instillation and pain during conjunctival clamping 5 and 10 min after gel application were compared. Extent of corneal conjunctival staining was graded according to the Oxford scale.
Results:
Eighty eyes of 40 patients were enrolled. The groups were similar in gender, with a mean age of 48 ± 16.26 years. The 5% lidocaine gel resulted in higher discomfort during initial instillation (P = 0.092), however, the pain during conjunctival clamping was lower in the 5% lidocaine gel eyes (P = 0.564) in both 5 and 10 min later (P < 0.001). The majority of patients (80%) had no corneal conjunctival dye staining. The tear break-up time was not statistically different after lidocaine gel 2% (20.35 ± 7.37 s) and lidocaine 5% (19.75 ± 7.00 s).
Conclusion:
Five percent and 2% lidocaine gel have similar efficacy controlling pain 5 min after instillation, however, 5% lidocaine gel appears to be more effective with a longer duration of action, without corneal toxicity. There was no corneal toxicity noted with either concentration.
Introduction
L
Topical anesthesia was first described in 1884 by the Austrian physician, Karl Koller demonstrating the anesthetic effects of a 5% cocaine solution on the eyes. 2 However, due to adverse effects such as tachycardia, respiratory depression, and death, 3 this can no longer be used in medical practice. The use of topical anesthesia has been reported by several medical specialties. 4 Lidocaine gel 2% preparations are being used in several systemic procedures, including those of upper airway and gastrointestinal and urogenital tract, demonstrating excellent results.5,6 Later, lidocaine hydrochloride ophthalmic gel was shown to have good absorption following topical administration to mucous membranes.
Topical anesthetics play an important role in the practice of ophthalmology. Both the cornea and the conjunctiva are quite susceptible to topical anesthesia because their sensory nerve endings are free between the epithelial cells. 7 On the corneal surface, these ends are protected only by the tear film and epithelium. On the conjunctiva, the endings are covered by a nonkeratinized stratified epithelium, readily penetrated by topical anesthetics, if the pH conditions are adequate. 8 Topical ophthalmic anesthetic preparations are typically acidic, which contributes to the stinging sensation when first applied. The gel formulation of lidocaine may enhance anesthetic effect, and therefore superior to anesthetic solutions for topical cataract. The need for safe, long-acting, topical, ocular anesthetic agents is an ongoing need for ophthalmology practices, and has been highlighted by the increase of intravitreal administration of pharmacologic agents. Other ocular procedures requiring longer-acting topical anesthetic agent include cataract surgery, glaucoma filtration surgery, strabismus surgery, panretinal photocoagulation, focal laser coagulation, laser retinopexy, and vitreoretinal surgery.
Objectives
To compare same-day pain control and safety of 2 different anesthetic gels utilizing 5% and 2% lidocaine gel and evaluate the incidence of corneal toxicity. Main outcome is to determine whether 5% lidocaine gel is more effective in decreasing pain during conjunctival clamping compared to 2% lidocaine gel 5 and 10 min after gel application.
Methods
A prospective, randomized double-blind study was performed between August and September of 2013. The study was approved by the Research Ethics Committee of Plataforma Brasil (No. CAAE 02117212.9.0000.5505) and was performed in accordance with the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients before participation.
Vials containing lidocaine hydrochloride gel 2% and 5% with hydroxypropyl methylcellulose (HPMC) viscosity ranging from 1,000 to 2,000 mPa, preservative free, and of physiological pH, were produced by a pharmaceutical laboratory and were listed randomly.
Patients were asked to choose 1 vial from an opaque envelope containing 2 identical appearance vials with either lidocaine 2% or 5%. The vials were numbered and unmasked at the end of the study. Patient's eyes were randomly selected by a computer program (www.randomization.com) to a different preparation in each eye on the same day. Only healthy patients between the age of 18 and 75 were included in this study. The patients participated in the study voluntarily. Patients who had undergone ophthalmic procedures in the last 6 months with external ocular disease and 1-eyed patients were excluded.
Comparison of discomfort between different lidocaine gel concentrations was evaluated by each patient after randomization and receiving a drop of lidocaine gel 2% in 1 eye and 5% in the contralateral. A masked investigator administered visual analogue scale (VAS) questionnaire to evaluate the patient's discomfort level. Five minutes after the instillation of lidocaine, the inferior temporal bulbar conjunctiva of each eye was clamped with 0.3 mm conjunctival forceps and the pain intensity was recorded. This process was repeated after 10 min to determine which concentration had a longer duration of action.
The tear film break-up time (TBUT) is a test to measure the relative stability of the precorneal tear film. TBUT was measured by instilling 1 drop of 2% fluorescein into the lower fornix (Ophthalmos, Sao Paulo, Brazil). The patients were allowed to blink at a spontaneous rate, and the elapsed time from the last blink to the appearance of the first break in the continuous layer of fluorescein, as observed under cobalt blue light through a yellow filter, was measured in seconds. Corneal fluorescein staining was graded 1 min after fluorescein instillation based on the Oxford scale. The Oxford grading scale uses a series of panels, labeled A to E (6 groups) in order of increasing severity. This scoring system uses a chart consisting of a series of panels (A-B-C-D-E) in order of increasing severity. The amount of staining seen in each panel, represented by punctate dots, increases by 1 log unit between panel A and B and by 0.5 log units between other panels B to E. 9
After the data were collected, the concentrations of the anesthetic gel were revealed and formed into 2 groups. Group A composed of the eyes that received lidocaine gel 2% and group B 5%. Statistical analysis was performed with the program Statistical Package for the Social Sciences (SPSS) version 20.0 Statistics®.
The data collected with a normal distribution were evaluated by the Student t-test for paired samples, whereas variables with nonparametric distribution were analyzed using the Wilcoxon test. Differences with P < 0.05 were considered statistically significant.
Inclusion of 40 patients insured 95% power for detecting a difference between groups using 2-tail t-test. 10
Results
Eighty eyes of 40 patients, between the ages of 18 and 73 with an average age of 48 ± 16.26 years, were evaluated. The group consisted of 15 (37.5%) men and 25 (62.5%) women.
The analysis of pooled data revealed that discomfort during the instillation of lidocaine gel was slightly higher in group B (n = 20) than in group A (n = 12), but difference was not statistically significant (P = 0.092). Eight patients felt equal discomfort in both eyes.
Pain levels were assessed 5 and 10 min after the instillation of the anesthetic gel, during conjunctival clamping. At 5 min after the instillation of lidocaine, patients reported to be equally satisfied with pain control during conjunctival clamping. Discomfort in the group B (5% gel) compared to group A (2% gel) was not statistically significant (P = 0.564; Fig. 1). Ten minutes after the instillation of lidocaine, group B (5% gel) experienced significantly less pain during conjunctival clamping compared to group A (2% gel), and the difference was statistically significant (P < 0.001; Fig. 2).
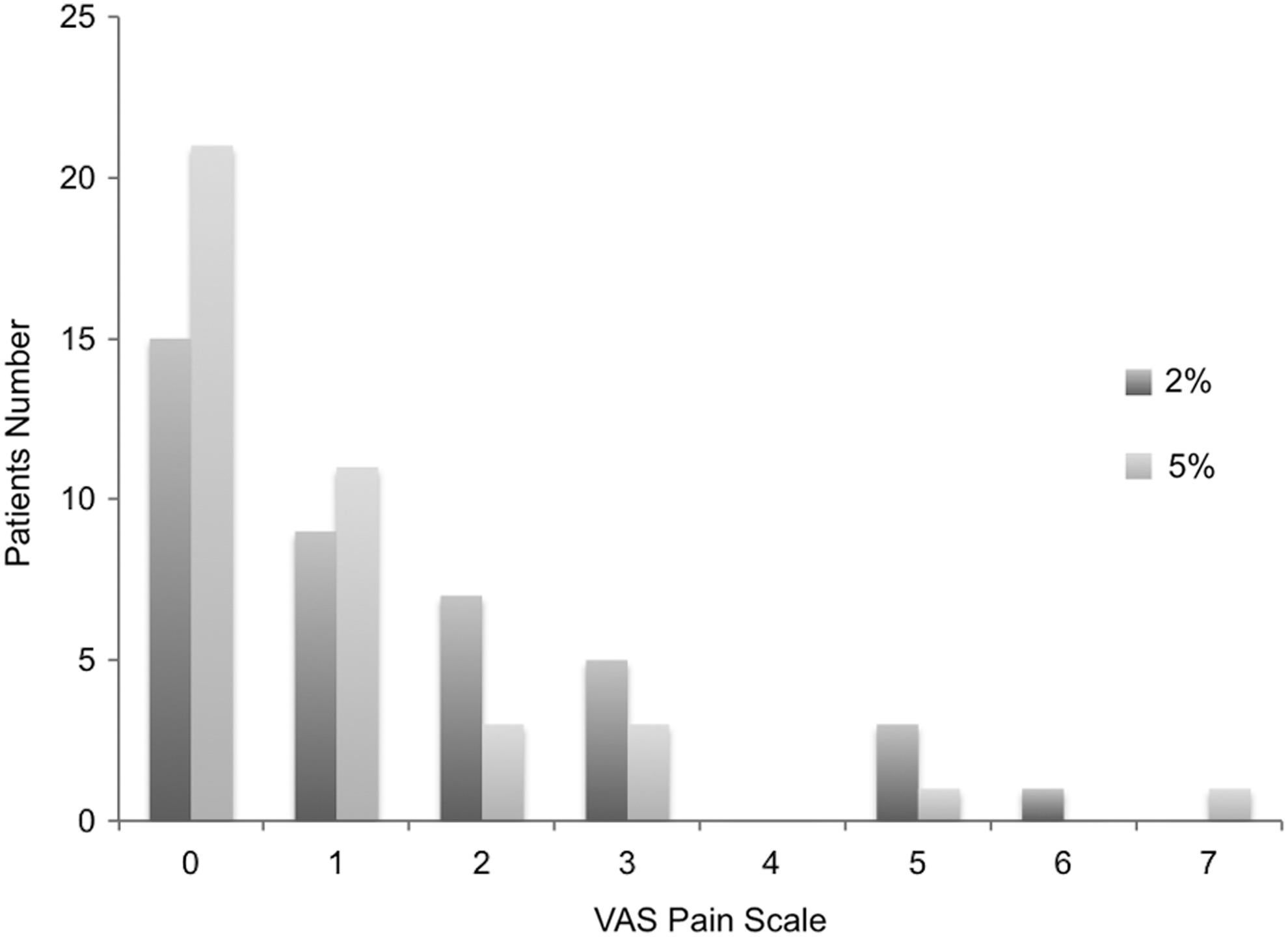
Histogram demonstrating the frequency of pain, during conjunctival clamping in the fifth minute after the instillation of lidocaine gel.
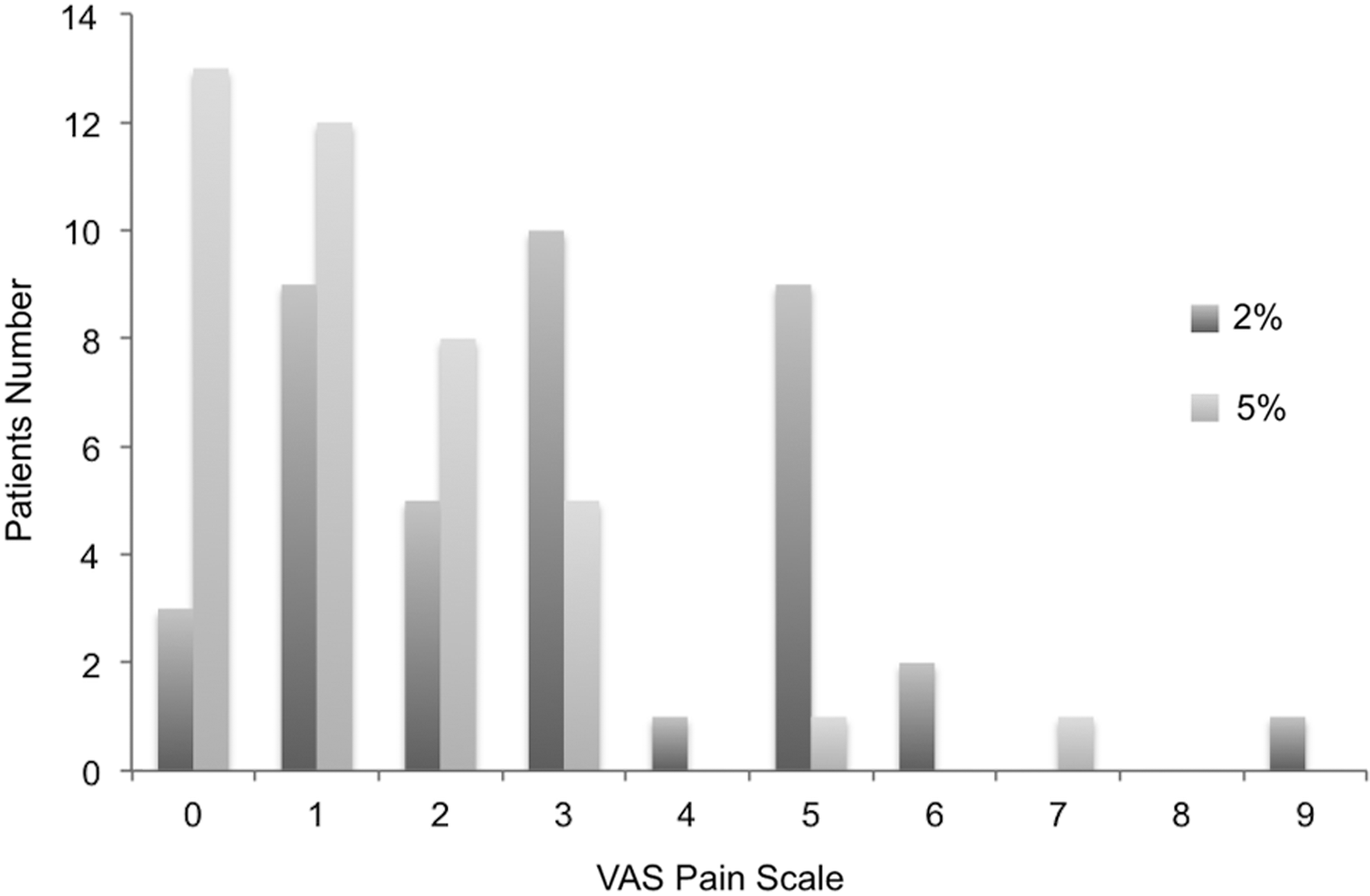
Pain during conjunctival clamping, in the 10th minute after the instillation of lidocaine gel.
The most common adverse event was corneal staining. Both groups had some degree of corneal fluorescein staining according to Oxford scale, with a trend of a higher incidence of corneal fluorescein staining in the group B (P = 0.562), although the difference was not statistically significant. No serious adverse events were noted.
The average TBUT result was not statistically significantly different (P = 0.55); in the group with lidocaine gel 2%, the TBUT was 20.35 ± 7.37 s compared to the group with lidocaine gel 5% of 19.75 ± 7.00 s.
Discussion
With the development of surgical techniques using microincisions and new pharmacological drugs for intravitreal injection, there was an increase in the number of ophthalmic procedures with short duration, 11 which may be performed satisfactorily under topical anesthesia, minimizing the risk of retrobulbar and peribulbar injection. Minimizing the use of needles and invasive techniques to deliver anesthesia has been an ongoing trend in ophthalmic anesthesia over the past decade.
The physicochemical characteristics of LA, as potency and the time and duration of action, are determined by the chemical configuration of the ends of the molecule. Anesthetic agents used in clinical practice are unstable in the amine form and insoluble in water. Therefore, they are prepared in the form of salts, becoming more stable at a relatively acidic pH. The low pH of commercially available solutions is the main cause of the stinging sensation during instillation. 12
Lidocaine was synthesized in 1946 by Landau et al. 13 and is an amide and a derivative of xylidine with a half-life of around 90 min. The proximetacaine is an ester with a half-life of ∼20 min, the instillation is comfortable and well tolerated by patients with low corneal toxicity. Clinical studies evaluated the effectiveness of lidocaine gel 3.5% (Akten®) and have demonstrated that this product was safe and provided good pain control in most cases. 2
In the literature, controversy exists regarding the possible side effects of the repeated use of local anesthetic, with studies showing a potential deleterious effect on the cornea. This may cause epitheliopathy, deep corneal infiltrates, and culminating in perforation. 14 Baraquet et al. found no damage in ocular tissue histopathology in an experimental study conducted in rabbits. 15 The anesthetic gel, in turn, showed lubricant properties on the cornea in cataract surgeries and can reduce the presence of keratitis in patients undergoing ophthalmic procedures. However, when preservatives are added to the solution, the epithelial toxicity is further pronounced. 16
In our study, instillation of lidocaine gel 5% caused more ocular discomfort compared to the concentration of 2%, but this difference was not statistically significant. We showed that both lidocaine concentrations resulted in minimal ocular surface changes (grades I and II on the Oxford scale) and the difference was not statistically significant.
Long-lasting effect of the topical ocular anesthetic with minimal side effects is crucial during surgical procedures. The viscous property of the gel allows a prolonged ocular surface contact time, lengthening its effect on pain-sensitive ocular structures, resulting in better distribution and better anesthesia. We demonstrated that the group receiving lidocaine gel 5% presented a more prolonged anesthetic effect compared to a lower concentration, corroborating the results found by Busbee et al., which showed an increased anesthesia time, using lidocaine gel 3.5%. Therefore, an anesthetic technique resulting in a longer duration with minimal corneal side effects should be preferred. The superior anesthetic effect of lidocaine gel 5% after 10 min may be useful for various ophthalmic procedures, including phacoemulsification, pterygium resection, and refractive surgery.
A previous study done by our group showed no statistical difference among different concentrations of topical lidocaine gel for intravitreal injection and pain. Mean pain scores (±SD) were 2.63 (±1.68) in the 2% lidocaine group, 2.08 (±1.35) in the 3.5% group, 2.00 (±1.65) in the 5% group, 1.93 (±1.40) in the 8% group, and 1.83 (±1.35) in the 12% group (P = 0.077). 17 There was a tendency for more comfort in patients who received higher concentration of lidocaine, justifying this trial using concentration of 5%. Of note, Akten is not available to several countries outside the United States.
The use of topical ophthalmic anesthetic can reduce reflex tear secretion and cause symptoms of dry eye. In this study, the average of BUT was higher than physiological for both concentrations. The presence of HPMC in the composition might have been responsible for the maintenance of adequate corneal lubrication.
Conclusion
The study concluded that lidocaine gel 5% was effective with a longer duration of action compared to lidocaine 2%, without adverse effects on cornea.
Footnotes
Author Disclosure Statement
No competing financial interests exist.