
Abstract
Abstract
Purpose:
Intravitreal steroids, including dexamethasone implant (Ozurdex®), are effective for the treatment of diabetic macular edema (DME). However, the dosing regimen for Ozurdex in DME is unclear, and thus, this study was designed to evaluate the dosing regimen for dexamethasone in real-life clinical practice.
Methods:
Results are presented from 3 studies based on a questionnaire that was sent out by e-mail to physicians; the monitoring of drugs dispensing over time through pharmacies; and the French Social Security database for 2011 and 2012. Data are presented as the average number of dexamethasone treatments per year and the time interval between injections.
Results:
Study 1 involved 111 ophthalmologists and assessed DME prescriptions. The number of injections per year and the time interval between 2 successive injections were measured as 2.3 and 4.8 months, respectively. In study 2, the survey incorporated 570 prescriptions from retail pharmacies; the mean follow-up period was 13.7 months, and 2.3 injections were administered per year with a time interval between injections of 5.2 months. In study 3, relating to the reimbursements by social security, 114 patients were initially identified and, among these, 15 patients were treated with Ozurdex. Over the course of a 25-month follow-up period, an average of 2.5 Ozurdex implants were injected per year with 4.7 months between injections.
Conclusions:
The average number of dexamethasone implant injections was consistent between studies with an average of 2.4 injections per year and 4.9 months between treatments. This highlights the need for a study to evaluate the optimal treatment frequency in DME.
Introduction
D
Laser photocoagulation is the reference treatment, resulting in modest improvements in visual acuity in a small number of patients with center involving DME.6–8 The possible complications of this method include paracentral scotoma, accidental damage to the fovea, and neovascularization around a scar induced by the photocoagulation, therefore limiting the number of retreatment procedures. 9 Interestingly, the Early Treatment Diabetic Retinopathy Study (ETDRS) guidelines suggests that all patients with clinically significant DME should be treated with laser to prevent loss of visual acuity, whatever the stage of the disease. 10
However, intravitreal anti-VEGF (ranibizumab, Lucentis®; Genentech, Inc.) should be considered as the first-line treatment for diffuse or mixed DME. 11 The recommended dose in Europe is 0.5 mg and involves monthly administration until maximum visual acuity has been restored, that is, until the patient's visual acuity has been stable over 3 successive monthly assessments while the ranibizumab treatment is underway. If no improvement in visual acuity is obtained after 3 consecutive injections, the course of treatment could be questioned. 12 Subsequently, visual acuity should be checked every month. If visual acuity is observed to drop as a result of DME, treatment should be resumed and continued until visual acuity is stable for 3 successive monthly assessments (ie, for at least 2 more injections).13,14
Short acting corticosteroids such as IVT triamcinolone (Kenacort®; Bristol-Myers Squibb Australia Pty Ltd) rapidly dries out DME, but its positive effects on sight are mitigated by the fact that it could induce serious adverse events that may lead to blindness as reported by the distributor and French Drug Agency in 2007.15,16 In DRCR Protocol I (NCT00444600), patients with a pseudophakic lens and receiving 4 mg of triamcinolone and prompt laser arm appeared to have comparable results in terms of visual acuity to that in the ranibizumab groups, although its use is limited by risks of cataract and ocular hypertension. 17
In DME, dexamethasone implants (Ozurdex®; Allergan, Inc.) have been shown to improve visual acuity up to roughly 4 months accompanied by a manageable safety profile (common side effects are cataract formation and raised intraocular pressure). 18 Its usage in patients with resistant chronic DME (ie, unresponsive to 6 monthly consecutive intravitreal injections of ranibizumab) has also been investigated. 19 Since 2012, dexamethasone implant has been reimbursed in France for the treatment of adults with macular edema following branch retinal vein occlusion [(B)RVO] or central [(C)RVO], or inflammation of the posterior segment of the eye (eg, noninfectious uveitis). However, very little real-world data exist for the use of dexamethasone implants in DME and this means there are no data concerning the optimal posology for Ozurdex in DME.
This study aimed to assess, in real-world practice, the optimal posology by measuring the average number of dexamethasone implants injected per year and the time interval between successive injections in patients with DME and treated with this short-acting steroid.
Methods
Results are presented from the analysis of 3 independent studies by means of questionnaire sent out by e-mail to physicians (Survey: Ophthalmologists); monitoring the dispensing of drugs over time through pharmacies (Survey: Retail Pharmacies); and from the French Social Security (FSS) database for 2011 and 2012 (Table 1). All studies were made in France between July 2011 and May 2014, a period during which ranibizumab was approved in DME but not dexamethasone implant. Since the surveys are based on patient results, these studies adhered to the tenets of the Declaration of Helsinki.
Survey: retina specialist ophthalmologists
This study was conducted by Icomed (part of the Cegedim Group) using a questionnaire sent out by e-mail to selected physicians. The French Retina Society members’ database was used to select 900 active retina specialists involved in treating DME. Finally, among 900 selected participants, 111 valid questionnaires were part of the analysis in March 2014, from 20th to 28th. The questionnaire consisted of 4 questions where physicians were asked to complete empty boxes:
(1) How many patients are you treating for DME per month? (reply = 0, exclusion from the questionnaire) (2) Among these patients with DME, how many are treated per month with laser, anti-VEGF, and corticosteroid separately? (3) When you use the dexamethasone implant to treat chronic DME, how many injections are required per eye and per year? (4) What is the mean interval between successive injections of dexamethasone implant when you are treating chronic DME per month?
Survey: retail pharmacies
Monitoring the dispensing of drugs over time through pharmacies—the methodology of the IMS LifeLink™ Treatment Dynamics (LTD) study—is part of the development of postmarketing surveillance. It gives a real-world, pharmacy-based picture of drug use.
Each participating pharmacy activates a special application that interfaces with the pharmacy's operating software. Anonymous data are sent by the pharmacy to a trusted third party who makes a second anonymization.
IMS collected data from 6,312 pharmacies spread throughout France on all prescriptions dispensed from a cohort corresponding to 34% of patients in the French population with homogeneous coverage of all age groups.
A cohort of diabetic patients dispensed dexamethasone implant or ranibizumab at least once between March 2012 and May 2014 was selected. Two eligibility filters were then applied:
(1) “Pharmacies”: this filters out pharmacies that do not send data regularly enough. (2) “Patients”: this filters out peripatetic patients whose data might distort the results of analysis (missed pharmacy visits, etc.). This filter selects patients with enough pharmacy visits recorded (whatever the product) over the study period.
With this filtering, 575 eligible patients were followed in the cohort.
For patients in the cohort for this study, distinction was made between bilateral patients (being treated on both eyes) and unilateral patients. Bilateral patients included both those who received more than 1 injection on the same day and those who had more than 2 injections within 12 days (12 days was chosen as the threshold to avoid excluding prescriptions for 2 injections into the same eye).
As a result of application of this threshold, 5 patients who only had 2 prescriptions within 12 days during their whole course of treatment were automatically excluded. Eventually, 570 eligible patients were followed for this study. In addition, distinction was made between patients who made a “Switch” of products with no switch back and those who used the products alternately with switch back from a product to another (referred to as “Mixed” in this study) (Fig. 1). Patients who only had 2 or 3 injections during their course of treatment were all classified as Mixed.

“SWITCH” and “MIXED” patients in the retail pharmacies survey.
Ultimately, the group of patients analyzed for the study breaks down into 448 patients in the mixed group (331 unilateral, 157 bilateral) and 82 patients in the switch group (55 unilateral, 27 bilateral).
For each patient, the time interval between the first injection and the last injection registered in the study was used.
The duration of treatment was assessed by defining the interval between the dispensation of the first dexamethasone implant and the dispensation of the next DME treatment. This second treatment could be either another dexamethasone implant (DEX 1→DEX 2) or a ranibizumab injection (DEX 1→RBZ 2). Two types of mean were calculated (Fig. 2).
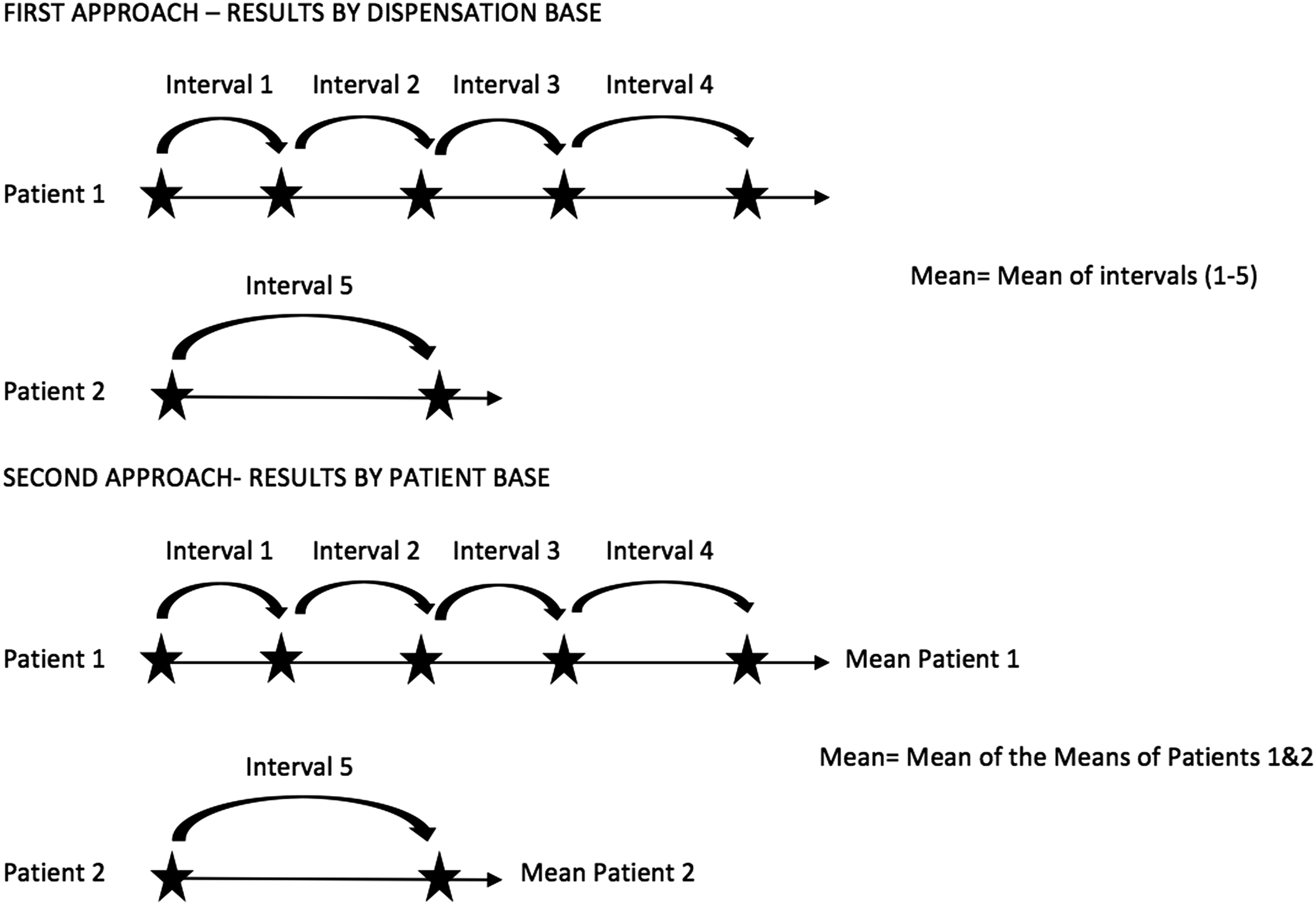
Two types of calculation for the mean interval between injections in the Retail Pharmacies Survey.
- For each of the patients, the time interval between each dexamethasone implant and the next intravitreal injection (regardless of drug class) was measured. The mean of all these intervals across all studied patients was calculated. Results based on this mean calculation are indicated by “Result (dispensation base),” which gives a same weight to all injections. Patients receiving multiple dexamethasone implants are weighted higher than patients receiving a single implant.
- For each of the patients, the mean time interval between each dexamethasone implant and the next intravitreal injection was measured individually. We thus have a mean time interval for each of the studied patients. Then, the overall mean across all these patients’ individual means is calculated. Results based on this mean calculation are indicated by “Result (patient base).” With this approach, all the patients are taken into account with the same weight even if they had different overall number of injections.
Therefore, all dispensations were pooled based on these criteria and assessed the mean duration as a function of patient category, that is, Unilateral or Bilateral and Mixed or Switch.
The “Dexamethasone implant—Mixed” patient panel comprised 292 patients, of whom 201 were in the unilateral group and 91 in the bilateral group. For each patient in the Mixed panel, those who during their courses of treatment had an injection of dexamethasone implant followed by another injection (DEX or RBZ) were identified. Then, each interval between the dispensation of dexamethasone implant and the next intravitreal therapy was measured.
Annual frequency of dexamethasone implant and ranibizumab injections was evaluated for each patient of the panel, the mean time interval between successive dispensations was determined, and then the mean interval for the whole panel was calculated.
Analysis of the FSS database extract
DME cannot be identified directly with an international Classification of Diseases diagnostic code in health insurance databases for the following reasons: DME is a complication of diabetes and is therefore 100% reimbursed as a long-term condition in France. This disease does not therefore allow for its treatments to be correlated with an explicit diagnosis. Treatments for DME are administered as outpatient procedures and are not recorded in reimbursement hospital files. In addition, treatments for DME (laser photocoagulation or intravitreal corticosteroids or anti-VEGF) are not used exclusively to treat diabetic conditions and so cannot be used to identify it indirectly using a selection algorithm to differentiate reliably between patients with DME and those with neovascular age-related macular degeneration (AMD).
Taking into account these restrictions, the extraction from the social security database was made for 2011 and 2012 using the following algorithm: patients with a ranibizumab injection for type 1 or type 2 diabetes; with a first dispensation of ranibizumab during the second semester of 2011 or civil year 2012 (ranibizumab indication was extended in June 2011); not having been dispensed Visudyne® or Macugen® during this period (AMD-specific treatment modalities).
Results
Survey: retina specialist ophthalmologists
The study revealed a mean of 2.34 injections of dexamethasone implant required per eye and per year, that is, about 7 injections for 3 years and a mean time interval of 4.77 months between successive injections, that is, about 7.5 injections for 3 years (Tables 2 and 3).
Survey: retail pharmacies database
On the basis of the cohort of 570 patients, 3 main parameters were measured: mean treatment interval per patient, and annual frequency of injection of dexamethasone implant.
The panel of patients was broken down according to the type of treatment (Unilateral/Bilateral, Switch/Mixed) and the total number of times dexamethasone implant was dispensed to the patients during their courses of treatment (Table 4). The mean follow-up time was 418.4 days (∼13.7 months) (Table 5).
In the final analysis, the distribution was fairly broad with a high standard deviation. The mean global time interval between 2 successive dexamethasone implants was 147.8 days (∼4.9 months). How the mean interval duration breaks down according to the total number of dispensations of dexamethasone implant is shown in Table 6.
The “patient base” study shows how mean interval duration breaks down on the basis of the mean per patient with an average of 160.4 days (∼5.3 months) (Table 7).
The “Dexamethasone implant—Switch” cohort consists of 77 patients, of whom 55 were in the Unilateral group and 22 in the Bilateral group whose injections of dexamethasone implant were administered continuously (before or after ranibizumab injections) rather than regularly alternating with injections of ranibizumab).
Analysis of the interval between successive dispensations shows, similarly to what was seen in the “Mixed” group, the mean was 137.0 days (∼4.5 months), which corresponds to the mean interval duration in the “Switch” patient panel. The data on how the mean interval between successive dispensations breaks down (dispensation base) are presented in Table 8.
Analysis shows great disparity between the means in the Unilateral and Bilateral groups. This difference could be partly due to the small size of this group as well as being affected by the results for patients who only underwent 2 dexamethasone implants. There is indeed great disparity between the mean for 2 dexamethasone implant (177.8 days) and the mean for more than 3 dexamethasone implant (89.7 days). Finally, it is worth noting that the means for the Unilateral and Bilateral groups are similar (∼90 days) for patients administered more than 3 successive injections of dexamethasone implant, suggesting the real mean interval between dexamethasone injections as experienced by the patients (Table 8).
The “Patient base” results in Table 9 show how mean interval between dispensations breaks down on the basis of mean calculation per patient.
The estimated mean annual number of injections was calculated from the mean interval between successive dispensations calculated on the basis of each of the 570 patients on our panel; this mean interval was extrapolated to an annual basis to estimate the mean annual number of injections (Table 10).
On average, the frequency of injection in patients with DME was slightly higher in the Switch cohort than in the Mixed cohort. This was observed for both dexamethasone implant and ranibizumab. Globally, for the whole entire panel, patients were administered ∼2.3 injections of dexamethasone implant per year compared with nearly 4.5 injections of ranibizumab.
Analysis of the FSS database
A total of 114 patients were identified using the algorithm. Their mean age was 70.4 (standard deviation 13.1) with 49.1% women. A proportion of 86% had type 2 diabetes (CIM10) and the mean duration of the disease was 13.1 years since classification as a Long-Term Care (standard deviation 8.1). Five patients died during the observation period. Among them, 15 patients were dispensed with dexamethasone implant at least once (2 bilateral and 13 unilateral) with mean number of dispensations of dexamethasone implant 1.5 in 7.1-month average follow-up period (mean number of dispensations of dexamethasone implant: 1 for bilateral and 1.6 for unilateral).
Linear extrapolation on a period of 1 year gives an estimate of the mean number of annual injections of dexamethasone implant by 2.5 with a mean of 4.7 months between successive injections.
Discussion
In this study, we evaluated the average number of dexamethasone implant treatments per year and the interval between dexamethasone implant treatments.
In the first 2 studies, “Ophthalmologists” and “Retail Pharmacies Surveys,” the average number of dexamethasone implant injections was 2.3 in both, with a similar frequency between dexamethasone implant injections (4.8 and 5.2 months, respectively). There was a similar result in the third study: 2.5 injections per year with a 4.7-month interval.
Boyer et al. recently reported the result of a 3-year, randomized trial of intravitreal dexamethasone implant in 1,048 DME patients (MEAD study). 19 This study was sponsored by the manufacturer to support the indication of dexamethasone in DME. Patients who completed the study had a mean value of 5 injections. In the MEAD study protocol, patients were not allowed to receive retreatment with dexamethasone implant earlier than 6 months. It drives to 2 consequences; first, the optimal number of injections during 3 years is underestimated and cannot be extrapolated from this trial. Second, all patients who needed an earlier retreatment were excluded. In its assessment report, the European Medical Agency (EMA) asked the company to conduct a postapproval study to further investigate the optimal posology in terms of frequency of retreatment. 20 The French medical authority also raises this point and talks about a loss of efficacy, 4 months after the injection. 21
Callanan et al. reported in 2013, a phase 2 prospective study (PLACID study), 22 which was also part of dexamethasone registration dossier. They compared the efficacy of dexamethasone and laser alone after 12 months in 253 patients. The dropout rate is important (around 20%) as the interval between injections had to be at least 6 months with a retreatment criteria based on the central foveal thickness. As in the MEAD study, the protocol influenced the frequency of dexamethasone injections. In addition, the mean number of injections of 1.67 in 12 months should be interpreted with caution as the PLACID study failed to meet its primary efficacy endpoint and therefore seems to have been influenced by the dosing of dexamethasone.
Guigou et al. reported in 2014, a retrospective, observational, multicenter study of dexamethasone implant treatment in patients with loss of visual acuity secondary to DME (MOZART study). 23 Sixty-nine eyes (59 patients) with DME (17% type 1 diabetes, 83% type 2 diabetes) were followed and monitored for ≥6 months (mean follow-up 9.8 months) across 5 ophthalmology centers in France. The patients were given 1.2 injections of dexamethasone implant on average at 6 months with a mean interval to reinjection of 5.4 months. 23 This study is presented as a retrospective study, and as retreatment criteria and concomitant therapies (laser, anti-VEGF) are not described, the results could hardly be interpreted.
In 2014, Gillies et al. reported the results from a prospective, comparative, open label study (BEVORDEX study) that compared the efficacy of dexamethasone with bevacizumab in the treatment of 88 eyes (61 patients; 42 eyes were treated with bevacizumab and 46 with dexamethasone) with center-involving DME. After 12 months, the results showed that bevacizumab-treated eyes received a mean of 8.6 injections versus 2.7 for dexamethasone. 24 The results of BEVORDEX study were recently presented (Arvo 2015 Congress) for the second year of treatment. For dexamethasone, the cumulative number was 5 (2.7 injections in the first year and 2.3 injections in the second year). In this independent study, the authors allowed a retreatment not earlier than 16 weeks after the previous one. Then, the decision to retreat the patient was based on the visual acuity evaluation.
Scaramuzzi et al. in a retrospective study presented the effects of repeated intravitreal dexamethasone implant in 15 eyes (12 patients) with DME with at least 2 dexamethasone implant injections (0.7 mg) on an as-needed basis with a variable retreatment interval. 25 The authors showed a meaningful improvement in visual acuity and central macular thickness reduction using dexamethasone implant injection with no serious side effects. Retreatment with dexamethasone implant was given after a mean of 7.8 ± 4.1 months from the first administration, 4.8 ± 0.9 months from the second administration, 5.3 ± 1.5 months from the third administration, and 5.6 ± 2 months from the fourth administration. 25
All these studies are summarized in Table 11 with consistent data for the number of injections per year all along the studies except for 2 industry-sponsored studies.
Our studies have some limitations that are related to their observational design. We observe that despite those limitations, results from those 3 independent sources are likely identical. The main limitations of the survey sent to the physicians are the relatively low rate of responses (12%) and the design of the survey, which was on a declarative basis for participating ophthalmologists, without any reference to a chart review. For the second survey, the retail pharmacies sample covered a significant part of the French population (34%), but limitations could come from the possible disconnect between the date of delivery of the product to the patient and the date of treatment by the ophthalmologist and from the baseline hypothesis for defining bilateral injections. In the social security database extract, DME is not identified as a specific condition of the patient, and a specific selection algorithm had to be defined from convergent data to get a sufficient degree of confidence to study specifically patients receiving dexamethasone for the purpose of treating DME (known diabetic patients, DME treatment history, exclusion of AMD-specific treatments). One other limit could be the decrease of dexamethasone implant injections all along the years. Our studies evaluated the number of dexamethasone implant injections during an observational period. During this period, some patients have initiation of dexamethasone implant treatment and some others are studied after many previous injections. We think that our results mimic the mean number of implants seen in clinical practice when some patients begin their treatment and some others had already received prior injections. BEVORDEX, the only prospective pro re nata trial published, showed a decrease of 15% of injections between the first and the second years of study. A linear extrapolation on 3 years gives a number of 7 injections of dexamethasone implants when treatment is assessed each time it is needed.
In conclusion, despite limitations due to the observational design of the studies and the evaluation of dexamethasone implant usage in DME during a period when it was not yet licensed for DME (off label use), the outcomes of these 3 studies show very similar results. The average number of dexamethasone implants per year was 2.4 and the time interval between treatments was 4.9 months. These data support the need for a study to evaluate the optimal frequency for intravitreal injections of dexamethasone implant as was requested by the EMA. In keeping with the dexamethasone implant studies submitted to the EMA, analysis needs to determine the number of injections per year and the time between treatments over a 36-month period. The outcomes in terms of visual acuity gain and in terms of safety profile impact should then be assessed after optimizing the time between treatments.
Footnotes
Acknowledgment
Financial or material support for the research and the work: Alimera Sciences France.
Author Disclosure Statement
No competing financial interests exist.