
Abstract
Abstract
Purpose:
Corneal crosslinking by UV light (UV-CXL) has become a popular treatment for keratoconus and corneal ectasia. Fluoroquinolones (FQs), commonly administered topically before UV-CXL, are known to be phototoxic to the skin and lens. The purpose of this study was to investigate phototoxic effects of topical FQ treatment on murine corneas before UV-CXL, in which the corneal epithelium was kept intact.
Methods:
Murine corneas were treated with various antibiotics with or without riboflavin before UV-CXL. At 24 h, the animals were sacrificed, and the corneas were analyzed for histologic evidence of inflammation and apoptosis and for expression of apoptosis markers BAX and caspases 3 and 9 and for expression of matrix metalloproteinase 9 (MMP-9). Spectrofluorometric analysis was performed.
Results:
Corneas treated with topical FQ with or without riboflavin before UV-CXL showed mild corneal stromal inflammation, apoptosis by both terminal deoxynucleotidyl transferase dUTP nick end labeling staining and increased expression of BAX gene and caspases 3 and 9 by densitometric analysis. Untreated corneas, corneas treated with azithromycin before UV-CXL, and corneas undergoing UV-CXL without any antibiotic or riboflavin pretreatment showed normal histology, no staining for apoptosis, and no increased production of apoptosis markers by polymerase chain reaction.
Conclusions:
The phototoxic effects of FQs on the cornea may lead surgeons to consider another antibiotic class for prophylaxis against infectious keratitis in UV-CXL. These effects, along with the known cytotoxic effects of FQs independent of UV radiation, may contribute to some of the complications of corneal UV-CXL. Dosage studies may be warranted.
Introduction
I
Topical fluoroquinolone drops can be administered immediately before the corneal-CXL as prophylaxis against corneal infection. 6 However, it is well documented that fluoroquinolones (FQs) are phototoxic to the skin 7 and lens. 8 FQs absorb UV radiation and induce long-lived triplet states, which produce singlet oxygen, superoxide, and other reactive species on interaction with oxygen, 9 damaging the lens and leading to formation of a cataract in vivo. 10 Aside from phototoxic effects of FQs, studies of cultured human corneal keratocytes suggest that levofloxacin, 11 moxifloxacin, 11 ofloxacin, 12 norfloxacin, 12 and ciprofloxacin 12 without UV radiation are toxic to keratocytes. In vivo rabbit studies of ofloxacin demonstrate the same finding, giving rise to a hypothesis that ofloxacin, acting synergistically with a yet to be identified factor, induces apoptosis in keratocytes, predisposing some corneas to perforation. 13 In vivo studies have shown that newer FQs can lead to epithelial thinning. 14
The purpose of this study was to investigate possible phototoxicity from topical FQ administered to murine eyes before UV-CXL, in which corneal epithelium was kept intact to avert introduction of inflammation and wound healing related to epithelial debridement.
Methods
All animals were treated in accordance with the tenets of the Association for Research in Vision and Ophthalmology (ARVO) statement for the use of animals in Ophthalmic and Vision Research and Catholic University of Cordoba, Medicine. Anesthesia was achieved by intramuscular injection of 0.5 mL/kg body weight of a mixture 1:1 of 100 mg/mL ketamine and 20 mg/mL xylazine. There were 7 treatment groups of mice (N = 16 per group); only the right eyes of each group were studied. Group 1 consisted of normal untreated corneas; Group 2 was UV-CXL without riboflavin or any antibiotic; Group 3 was UV-CXL with moxifloxacin pretreatment; Group 4 was UV-CXL with gatifloxacin pretreatment; Group 5 was UV-CXL with azithromycin pretreatment; Group 6 was UV-CXL with riboflavin but no antibiotic pretreatment; and Group 7 was UV-CXL with riboflavin and moxifloxacin pretreatment. Drops of riboflavin 0.1% were given at intervals of 1–5 min for 15–30 min, or until riboflavin could be seen in the anterior chamber of the eye by use of the blue filter on portable slit lamp examination. In groups 3, 4, 5, and 7, pretreatment with antibiotic comprised drops every 2 h starting 12 h before UV-CXL. UV-light treatment commenced 15–20 min after the last set of antibiotic drops at a power of 1.4–7.3 J/cm2 (0.7–4 mW/cm2) for 20 min without epithelial debridement.
Immediately after the procedure, study eyes were thoroughly irrigated with balanced salt solution. Animals were sacrificed 24 h after start of the investigation. The corneas from animals were removed, embedded in ornithine carbamoyltransferase compound (OCT Tissue-Tek; Miles, Inc., Elkhart, IN), and frozen at −80°C. Evidence of corneal phototoxicity was presumed by the presence of staining for apoptosis; apoptosis markers BAX and caspases 3 and 9; and degradative matrix metalloproteinase 9 (MMP-9) in corneas. Cryostat sections of the central 8 μm of each cornea were stained with hematoxylin and eosin and stained for apoptosis fragments of cell nuclei using terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL). Polymerase chain reaction (PCR) for BAX and caspases 3 and 9 was performed according to the manufacturer's guidelines (BioRad, Life Science, CA). Zymography for MMP-9 was also performed. Immunohistochemical analysis was performed using an avidin–biotin–peroxidase complex technique (Oncogene, Cambridge, MA, and Chemicon, Temecula, CA).
Statistical analysis
For each group, the number of corneas that stained with TUNEL or for apoptosis markers BAX, caspase 3, or caspase 9, or inflammatory marker MMP-9 was counted in an observer-blinded manner and compared with Group 1 using Fisher's exact test (Table 1). PCR for apoptosis markers and MMP-9 zymograms was quantified using scanning densitometry analysis (Molecular Dynamics, Sunnyvale, CA) and averaged (each cornea was analyzed in duplicate). One-way analysis of variance (ANOVA), Dunnett's multiple comparison test, and Bonferroni correction for multiple comparisons were performed between control and treatment groups [SPSS, ver. 10.0 for Windows; SPSS, Inc., Chicago, IL, and Microstat-Ecosoft, Inc., Indianapolis, IN] (Fig. 2). A P value <0.05 was considered statistically significant.
Immunostaining is reported as a proportion of number of corneas with positive TUNEL or immunostaining for Bax, Caspase 3 or 9, or MMP/total number of corneas examined.
Statistically significant difference when compared to Group 1 (Control), to Group 2 (UV light), and to Group 5 (UV-CXL+Azithromycin) (P < 0.001 using Fisher's exact test analysis).
MMP-9, matrix metalloproteinase 9; n/s, not statistically significant; TUNEL, terminal deoxynucleotidyl transferase dUTP nick end labeling; UV-CXL, UV corneal crosslinking.
UV crosslinking parameters
The CSO VEGA corneal crosslinking device (Scandicci Firenze, Italy) used in this study emits peak UV light wavelength at 370 nm, with a spectrum of irradiation between 358 and 382 nm, and has a power of 3 mW/cm2 with an irradiation size up to 9 mm at a distance of 12 cm from corneal tissue.
Spectrofluorometric analysis
Three different diluted solutions of the commercially available antibiotics eye drops were prepared (concentration = 1.25 × 10−4%) and 20 μL aliquots of this solution were used to record the emission spectrum at different levels of excitation (365, 370, and 375 nm, respectively).
Spectrofluorometric analysis was performed using a Cary Eclipse Fluorescence spectrophotometer (Agilent Technologies, Inc. Headquarter, Santa Clara, CA) with a xenon flash lamp. All the reagents were analytical grade and Milli-Q water (Merck Millipore, Billerica, MA) was used.
Results
Portable slit lamp examination of eyes before sacrifice showed no conjunctival injection, thinning, or anterior chamber reaction. There was no case of perforation.
Untreated corneas, corneas pretreated with azithromycin, and corneas undergoing UV-CXL without antibiotic or riboflavin pretreatment were clear and compact on slit lamp examination and demonstrated normal histology, no inflammatory infiltrates, no TUNEL staining (Fig. 1A), and no staining or expression of apoptosis markers BAX or caspases 3 or 9 by densitometric analysis. Zymography for MMP-9 was minimal (Table 1, Fig. 2).

TUNEL (terminal deoxynucleotidyl transferase-mediated dUTP-biotin nick end labeling) marked fluorescence microscopic images of murine corneas.

Corneas were subjected to densitometry analysis (means with standard deviation bars) of inflammatory marker MMP-9 and apoptotic markers BAX and caspases 3 and 9. Phototoxic effects of topical fluoroquinolones with or without riboflavin in UV-CXL compared to untreated corneas, corneas treated with azithromycin, and corneas treated with UV-CXL without antibiotic or riboflavin are shown. *Denotes that treatment with topical FQs with or without riboflavin before UV-CXL increased expression of MMP-9, BAX, and caspases 3 and 9 compared with other groups (ANOVA, P < 0.001). ANOVA, analysis of variance; azithro, azithromycin; FQs, fluoroquinolones; gati, gatifloxacin; MMP-9, matrix metalloproteinase 9; moxi, moxifloxacin; SD, standard deviation; UV-CXL, UV crosslinked corneas.
Corneas treated with FQ or riboflavin or riboflavin plus moxifloxacin before UV-CXL showed light epithelial haze on portable slit lamp examination. Histologic examination revealed mild inflammatory recruitment in the superficial stroma. TUNEL staining for apoptosis was positive (Fig. 1B), and expression of BAX, caspases 3 and 9, and MMP-9 (Table 1, Fig. 2) was increased in FQ, riboflavin, and riboflavin plus moxifloxacin groups compared with untreated, UV-CXL, and azithromycin groups.
BAX, caspases 3 and 9, and MMP-9 expression was higher in either FQ group, in riboflavin-pretreated, and riboflavin- and moxifloxacin-pretreated corneas compared with the other groups: untreated, azithromycin, and UV-CXL (ANOVA, P < 0.001) (Fig. 2). The highest expression of BAX, caspases 3 and 9, and MMP-9 was in the group pretreated with riboflavin and moxifloxacin.
By spectrofluorometry, we found absorption spectra (Fig. 3) of FQs moxifloxacin and gatifloxacin, with negative absorption results for azithromycin. The emission (Fig. 4) and excitation (Fig. 5) spectra by irradiation at different wavelengths were centered around 483–510 nm for each FQ, respectively. The excitation spectra are coincident with the absorbance spectra (Fig. 3). The Fig. 5 shows the excitation of both FQs at the wavelength used for corneal crosslinking.

Absorption spectrum of azithromycin, gatifloxacin, moxifloxacin, and Milli-Q water. Azithromycin was observed to have no absorption, gatifloxacin has a maximum absorption peak at 292 nm (absorption 0.916), and moxifloxacin has a maximum absorption peak at 293 nm to (absorption 1.229). Milli-Q water sample served as a negative control.
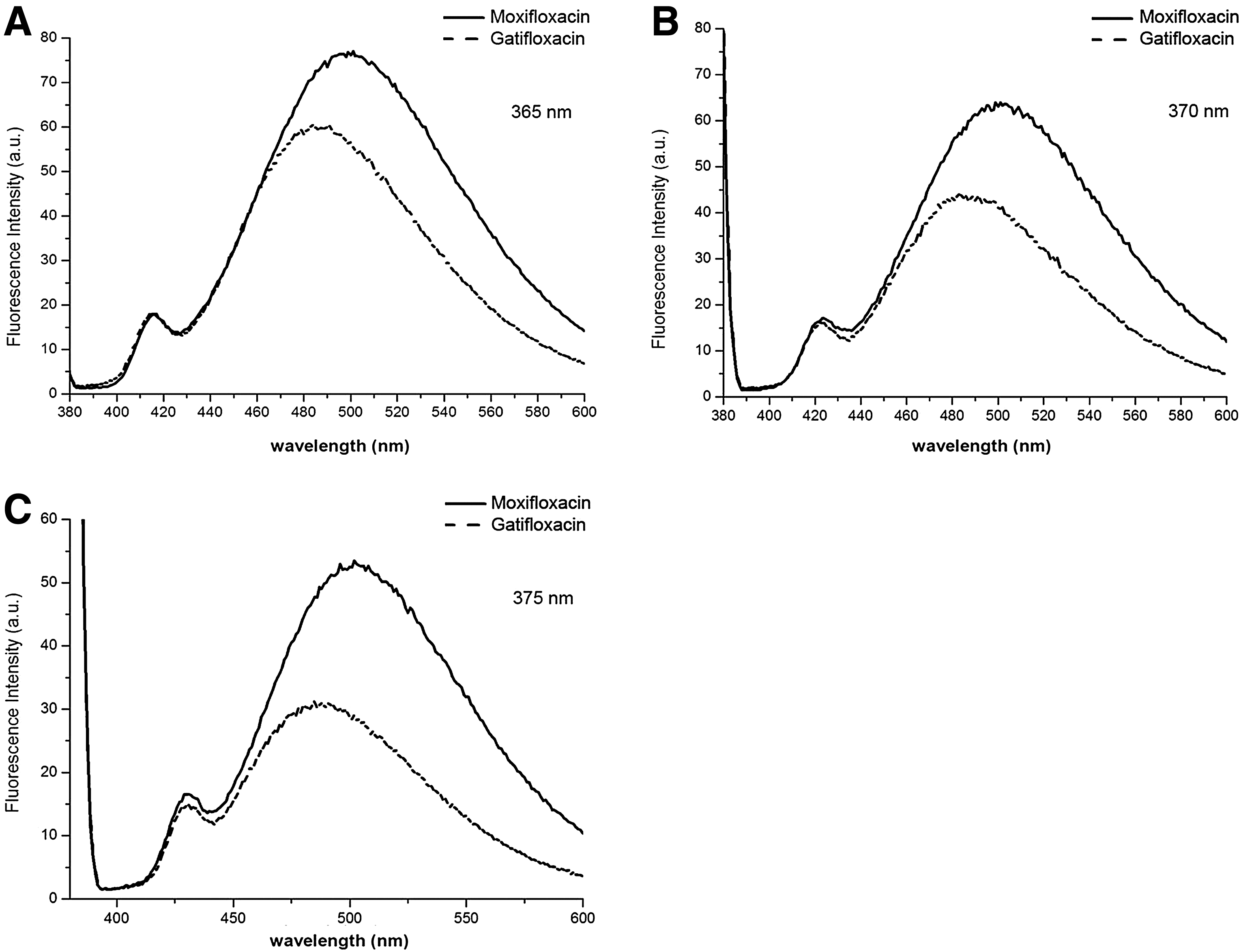
Emission spectrum of gatifloxacin and moxifloxacin at 365, 370, and 375 nm, respectively
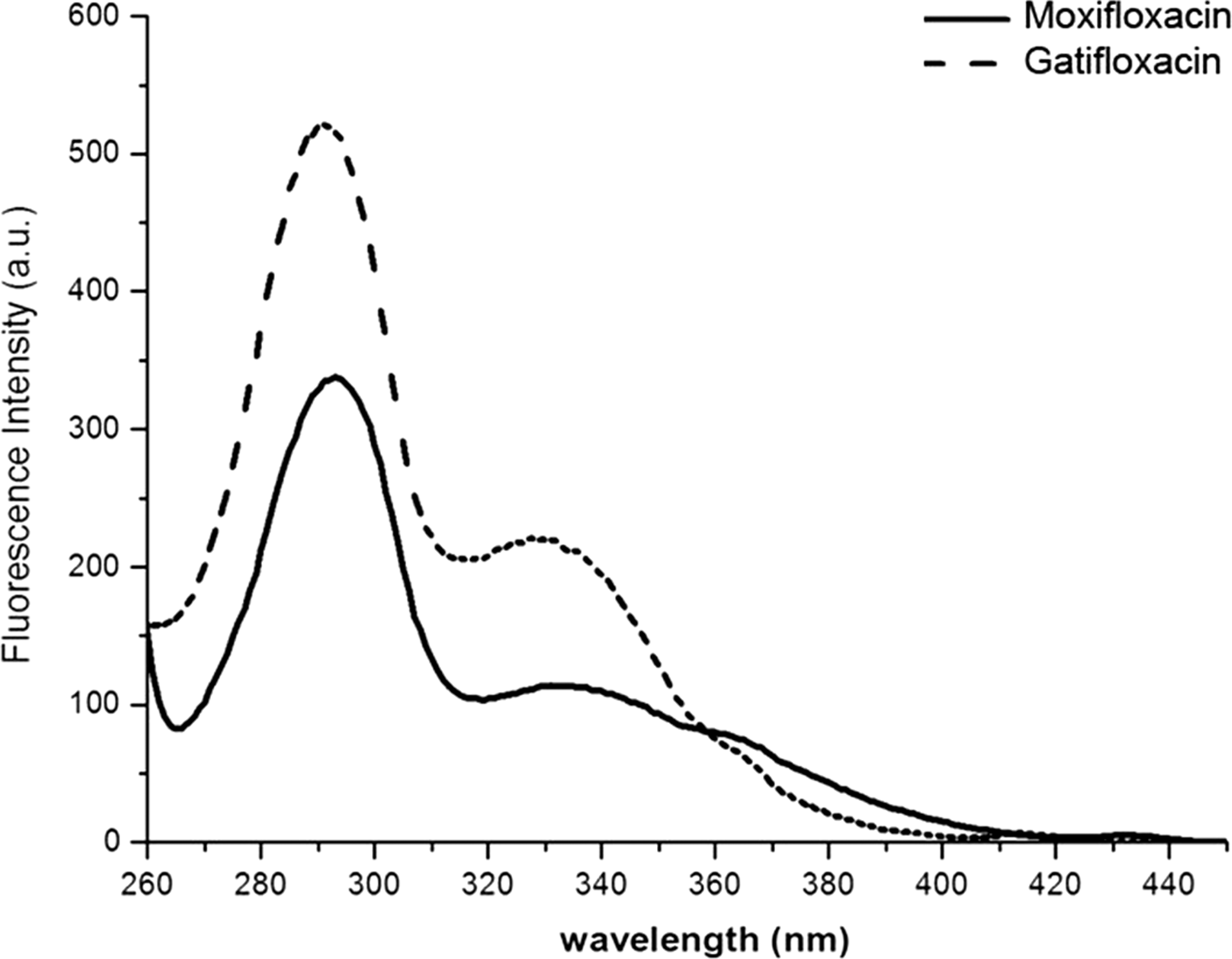
Excitation spectrum of moxifloxacin (483 nm) and gatifloxacin (504 nm), arbitrary units (a.u.). This excitation spectrum is coincident with the absorption spectrum, implying that there is no aggregation in this medium. That neither gatifloxacin nor moxifloxacin manifests phenomena of aggregation or formation of new complexes means that under these conditions, drugs remained unchanged in this experiment.
Discussion
In murine corneas undergoing UV-CXL, pretreatment with FQ drops induced stromal apoptosis, inflammation, and MMP-9 production in the same manner that riboflavin as a photosensitizer in UV-CXL induces changes such as apoptosis 15 ; combined riboflavin and moxifloxacin pretreatment (as in the clinical scenario) induced the highest expression of apoptosis markers and degradative MMP-9. We believe these findings result from photosensitization by riboflavin and phototoxicity of FQs. As FQs alone without riboflavin can induce a phototoxic reaction that includes necrosis, apoptosis, and loss of human lens epithelial cells, 8 it is possible that FQs administered topically before UV-CXL bind to corneal components not yet identified, leading to similar pathologic findings in the cornea 13 and corneal complications after UV-CXL.
Although the FQs in this study have absorption peaks at lower wavelengths, 16 it is still possible for higher wavelengths from the crosslinking device to excite higher singlet states, leading one to observe peaks in the excitation spectrum. This result is shown in Fig. 3. These absorptions/excitations at higher wavelengths do eventually lead to emission from the lowest singlet state evidenced by the peak emissions (Figs. 3 and 4). It is unlikely given factory specifications for our crosslinking device that the UV-light was nonspecific and caused excitation to higher energy than specified.
Intermolecular quenching can be expected to suppress the excitation of a drug (riboflavin by antibiotic or vice versa, depending on concentration in the aqueous humor), but by inference from our results of apoptosis marker expression (which was highest in the group pretreated with riboflavin and moxifloxacin), we presume there was not substantial suppression of riboflavin excitation by moxifloxacin or vice versa. Given the scope of our study, however, we do not purport to describe the interaction between riboflavin and antibiotic eye drops on corneal tissue during crosslinking, which can be influenced by local tissue pH 17 ; oxygen levels 17 ; effect of UV irradiation of different wavelengths, powers, and varying distances from the cornea; the wound-healing cascade; and other in vivo factors that remain to be elucidated.
In this experiment, the corneal epithelium was kept intact; epithelial debridement (which most surgeons perform in UV-CXL) causes inflammation and cytokine expression. By retaining the epithelium, findings of inflammation, expression of apoptosis markers, and increased MMP-9 expression may be attributed to the combination of UV-CXL and FQs alone. Apoptosis is regulated by BAX and caspases-3 and −9, the initiator and effector proteins, respectively; MMP-9, a zinc metalloproteinase, degrades the collagens of the extracellular matrix and is found in inflamed corneas. At 24 h, apoptosis staining and expression of these enzymes—the outcomes of interest for this study—were already present; at 36–48 h and beyond, corneal wound healing starts to occur and might have obfuscated some of the phototoxic effects. Given biologic variability, it is possible some (or many) corneas can heal from such insult; however, antibiotics without phototoxic effects are available. Translated to the clinical scenario, CXL is effective for many patients, but the intended outcome still eludes some patients, with complications such as scar (a finding of aberrant wound healing), endotheliitis, and perforation.
If a photosensitizing drug binds to lens proteins, retention time in the lens increases and the hazard to the lens (loss of transparency and formation of a cataract in vivo) increases. 8 FQs have also been implicated in drug-induced phototoxicity in melanocytes in cell culture, 18 which may have implications for pigmented tissue such as skin and ocular structures. One reason for the popularity of FQs in ophthalmic use is that topical (and systemic) administration penetrates ocular tissues sufficiently to achieve aqueous humor concentrations higher than the MIC90 for most microorganisms associated with corneal ulceration and endophthalmitis. 19 With high levels of penetration and a known phototoxic profile, it is possible that FQs in UV-CXL exert a phototoxic effect on keratocytes. In the clinical scenario, surgeons may prescribe FQs postoperatively or preoperatively. A preoperative regimen might be FQ instillation 24 h before CXL or in the immediate preoperative period as some surgeons choose to do before cataract extraction; in the current investigation, the duration of drop instillation (12 h before CXL) served as a compromise between these 2 practices.
Some toxic reactions caused by FQs (topical, intracameral, or intravitreal) are independent of UV radiation, for example, corneal stromal edema perhaps from inhibition of the corneal endothelial pump, 13 altered cellular function and morphology with reduced intercellular contacts, cellular disorganization, and keratocyte death.13,20 Because FQs absorb UV radiation and induce reactive states that interact with oxygen to produce reactive species, it is possible that in corneal UV-CXL, UV light potentiates the cytotoxic effects of FQ on corneas. Our study strongly suggests that FQs can cause phototoxicity because as other studies and ours show, they can be excited by various wavelengths of UV-light, causing multiple peaks in excitation spectrum. 17 Phototoxicity may be influenced by local factors such as tissue pH and oxygen levels. 17
Gatifloxacin (ZYMAXID®; Allergan, Irvine, CA) has a maximum absorption peak at 292 nm and moxifloxacin (Vigamox®; Alcon, Fort Worth, TX) has a maximum absorption peak at 293 nm. When the emissions were analyzed, dilutions of both drugs fluoresced when the wavelength was 365, 370 (as in corneal crosslinking), and 375 nm. This result suggests that if such a low concentration of drug achieved this amount of fluorescence, perhaps when a commercial drug (undiluted) is used and subjected to crosslinking via 15 and 30 min of irradiation with UV-A light, fluorescence should increase, although not in proportion to the increased concentration because of self-quenching. This possibility could explain the activation of apoptotic cellular processes observed in this experiment. Additional studies are needed to clarify the in vivo interaction of UV light on FQs on corneas. Given the increasing popularity of UV-CXL and concomitant use of FQ prophylaxis, the phototoxic effects of FQs bear consideration. Since FQ use in the corneal crosslinking procedure serves to prevent (not treat) an infectious condition, antibiotics without phototoxic properties might be used instead.
Footnotes
Disclosure Statement
No competing financial interests exist.