
Abstract
Abstract
Purpose:
To describe the outcomes of intravitreal anti-vascular endothelial growth factor (VEGF) in the treatment of retinal angiomatous proliferation (RAP) in real-life practice in 7 Italian centers under the Progetto Luce initiative.
Methods:
Clinical data of 95 eyes of 95 patients affected by RAP, regularly followed up and treated with either intravitreal ranibizumab or bevacizumab over 12 months, were examined. After a loading phase of 3 consecutive injections, retreatments were administered following a pro-re-nata regimen on the basis of the persistence or the recurrence of subretinal/intraretinal fluid on optical coherence tomography, or leakage on fluorescein angiography.
Results:
Overall, the mean best corrected visual acuity changed from 0.66 to 0.53 LogMAR (P: 0.0003); 36.8% of eyes gained at least 3 ETDRS lines, whereas 13.7% lost >3 lines at the end of the follow-up. Mean central retinal thickness improved from 384 μm at baseline to 262 μm at the 12-month examination (P < 0.001). A serous pigment epithelium detachment (PED) was identified in 68.4% of eyes at baseline, and it was still detectable in 30.5% at the end of follow-up. The mean number of injections was 4.4 over the follow-up. A significantly greater proportion of eyes showed PED resolution in the subgroup treated with ranibizumab (P < 0.001).
Conclusions:
Intravitreal anti-VEGF treatment in routine clinical practice allows a significant improvement in visual function in patients affected by RAP. A limited number of anti-VEGF injections are generally required in most cases.
Introduction
R
The aim of the present study is to analyze the management of patients with RAP receiving anti-VEGF treatment in routine clinical practice in 7 Italian clinical centers.
Methods
The design of the study was a retrospective, interventional multicenter study conducted in 7 Italian centers of Lombardy, under the Progetto Luce initiative.
Patients affected by RAP, who underwent intravitreal anti-VEGF between June 2012 and January 2014, were considered. Written consent from each patient before inclusion and approval from the institutional review boards were obtained. Inclusion criteria were as follows: diagnosis of RAP achieved by means of fluorescein angiography (FA), indocyanine green angiography (ICGA), and spectral-domain optical coherence tomography (SD-OCT); best corrected visual acuity (BCVA) of at least 20/400; follow-up of at least 12 months; and intravitreal treatment with either ranibizumab or bevacizumab. All charts of the included patients must comply with these parameters: presence of a complete ophthalmologic examination, including BCVA on Early Treatment Diabetic Retinopathy Study charts, FA, ICGA, and SD-OCT at baseline. Exclusion criteria were as follows: any previous treatment for RAP (laser photocoagulation, submacular surgery, and photodynamic therapy); complications due to the neovascularization process, such as rips in the retinal pigment epithelium (RPE), RPE atrophy, and scarring; and presence of any other macular or optic nerve disease. The treatments were performed using intravitreal injections either of ranibizumab (Lucentis; Novartis Pharma, Switzerland) or bevacizumab (Avastin; Roche, Switzerland). Bevacizumab was fractioned by each hospital pharmacy, according to the guidelines of Italian Society of Ophthalmology. The treatment protocol included a loading phase of 3 consecutive injections, with further retreatments following a pro-re-nata regimen on the basis of the identification of persistence or recurrence of subretinal/intraretinal fluid on SD-OCT, and leakage on FA. Each patient underwent a monthly examination complete of BCVA measurement, biomicroscopic examination, and SD-OCT scan. FA and ICGA had to be carried out every 3 months. Furthermore, each investigator could perform additional FA and ICGA at any time over the follow-up to clarify uncertain cases.
The study complied with the tenets of the Declaration of Helsinki.
The main outcome measure was the change in the mean BCVA at 12 months. Secondary outcomes included changes in the mean central retinal thickness (CRT) and number of injections over the 12-month follow-up.
Results
Overall, clinical data of 95 eyes of 95 patients were analyzed. Mean ± standard deviation age was 62 ± 19 years, with 53 males and 42 females. Complete clinical data are listed in Table 1. No bilateral cases were included. All patients completed the 12-month follow-up.
A statistically significant improvement in visual acuity and central retinal thickness was recorded in all subgroups. A statistically significant difference was found comparing data of eyes showing resolution of pigment epithelium detachment at the 12-month examination, favoring treatment with ranibizumab (P < 0.001).
BCVA, best corrected visual acuity; CRT, central retinal thickness; PED, pigment epithelium detachment.
The mean BCVA changed from 0.66 ± 0.28 LogMAR to 0.53 ± 0.32 LogMAR (P: 0.0003) at the end of the 12-month follow-up. Thirty-five eyes (36.8%) gained at least 3 ETDRS lines, whereas 13 eyes (13.7%) lost >3 lines. Examining in more detail the 13 patients who lost >3 lines, 8 eyes showed the development of subretinal fibrosis and 7 eyes disclosed atrophic changes at the end of the follow-up (Fig. 1).
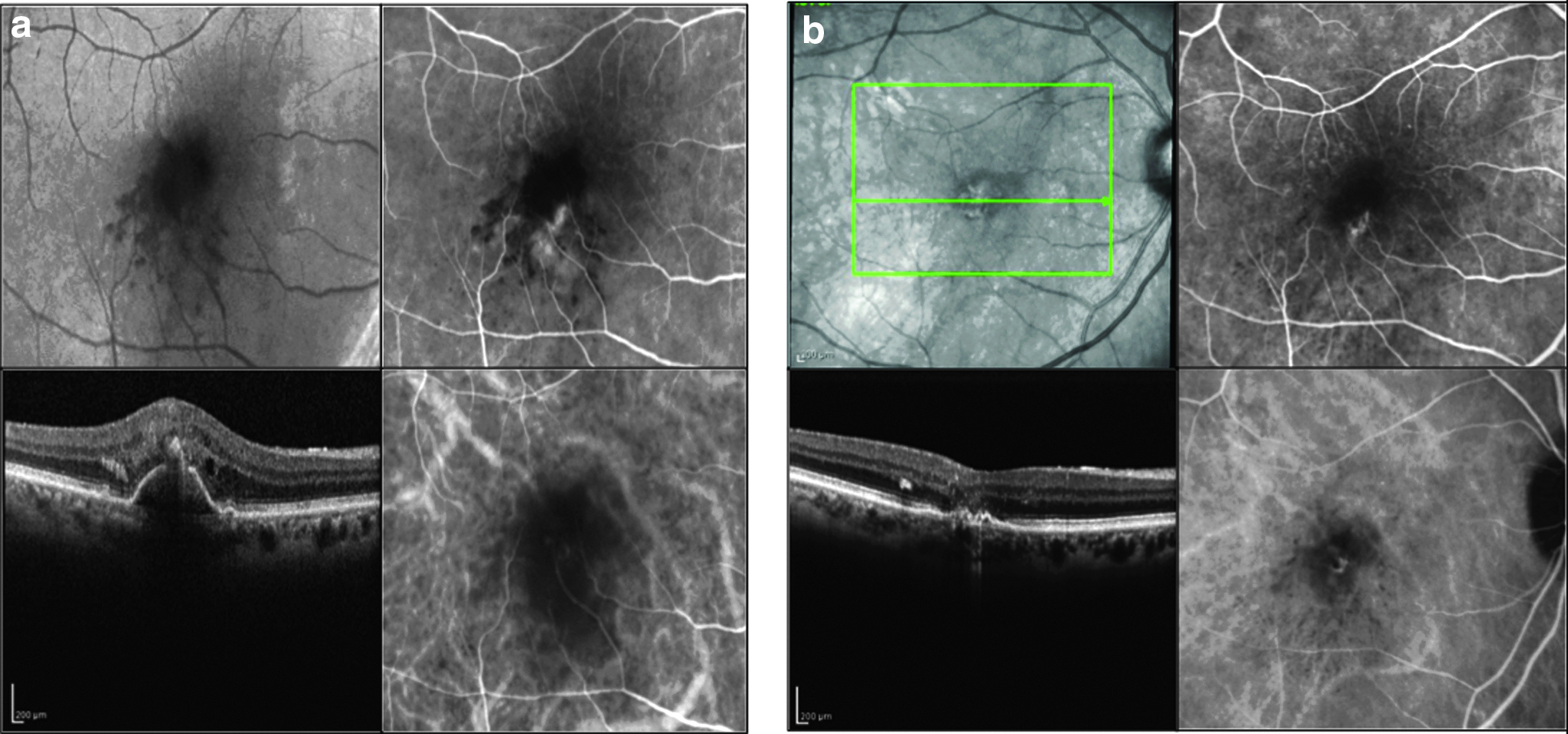
Example of RAP lesion:
The mean CRT improved from 384 ± 137 to 262 ± 112 μm (P < 0.01).
The morphological assessment of the treated lesions revealed that 10 eyes presented a RAP stage 1 (10.7%), 17 eyes a RAP stage 2 (17.8%), and 68 eyes a RAP stage 3 (71.5%).
Sixty-five eyes (68.1%) showed serous pigment epithelium detachment (PED) at baseline, which was still visible in 29 eyes (30.5%) at the end of the follow-up (Table 2).
FA, fluorescein angiography; IRF, intraretinal fluid; RAP, retinal angiomatous proliferation; SRF, subretinal fluid.
Each patient received a mean of 4.4 ± 1.2 injections within the 12-month follow-up.
Examination of patient distribution regarding the drug administered over the follow-up revealed that 26 patients (27.3%) received bevacizumab, whereas 69 (72.6%) patients were treated with ranibizumab. All the eyes were treated using the same drug over the whole follow-up.
A statistically significant improvement both in mean visual acuity and in CRT was registered in both subgroups at the end of the follow-up (Table 1). No difference was found between the 2 subgroups regarding the number of injections, but a statistically significant difference was registered comparing the rate of resolution of PED at the 12-month examination, where ranibizumab appeared more effective than bevacizumab (P < 0.05).
No ocular or systemic side effects were registered over the 12-month follow-up.
Discussion
The anti-VEGF approach has greatly improved the treatment outcomes in eyes affected by exudative neovascular AMD. In particular, both the morphological and the functional effects of anti-VEGF treatment of RAP generally provide better results in comparison to the other subtypes of AMD-related neovascularizations. The results obtained from several prospective clinical trials have shown that a remarkable improvement in visual acuity could be achieved in a large proportion of patients, both in short- and long-term follow-up. In addition, the mean number of injections over the first year was relatively low, ranging from 3.9 to 6.1.19–24
Nevertheless, the actual translation from clinical trials to real-life clinical practice is often hard, generally resulting in a more limited visual acuity gain, mainly related to a lower number of anti-VEGF injections.25–31
Our retrospective study on the real-life anti-VEGF treatment of RAP involving 7 Italian centers demonstrates that results comparable to those obtained in the clinical trials can also be achieved in routine clinical practice.
It is remarkable that the mean number of anti-VEGF injections registered in our study corresponds to 4.4. This finding is perfectly in line with that already shown by previous studies.19–24,32 Indeed, most of the real-life studies regarding anti-VEGF management of AMD reported that the mean number of injection in the first year lies between 4 and 5. Thus, the common real-life management leading to an apparently low number of injections may turn out to be enough for the practical management of RAP lesions. A clinical trial extending the follow-up to the 3 years indicated that 10.2 injections were required overall, suggesting that RAP could necessitate fewer injections compared to the other neovascular AMD subforms. 32 A recent CATT report showed that at both 1 and 2 years after initiation of anti-VEGF treatment in eyes with RAP received a lower mean number of injections in year 1 and 2 with respect to eyes without RAP, with a similar functional improvement. 19
Comparing the outcomes of the 2 molecules used in our retrospective study, the results appeared to be quite similar for BCVA gain, CRT, and number of injections. The marginal superiority of ranibizumab especially regarding the flattening of PED has already been highlighted by another trial. 22 This response could be ascribed to the deeper penetration of the ranibizumab molecule, allowing a powerful effect in drying the fluid, as also shown by the CATT and IVAN trials.19,33,34
It is not surprising that almost 3 quarters of the patients in our case series received ranibizumab injections, due to the regulations in Italy, where ranibizumab was approved and specifically reimbursed for AMD. The administration of bevacizumab was allowed only in some departments when economical issues were stringent.
We acknowledge that the present study has some limitations. First, the retrospective evaluation of patients' charts could be a source of bias, as well as the multicenter nature of the study. We decided to include just patients who fully completed 12-month follow-up with complete adherence to the visit protocol, but we cannot rule out possible discrepancies in the treatment assessment among the centers. Second, 2 different molecules were used in the centers according to the local availability. Thus, while this condition perfectly reflects the current practical situation, the specific choice could have affected the outcomes. In addition, there was no central reading center, allowing the retreatment to be decided on the basis of the local center discretion.
In conclusion, our data indicate that anti-VEGF management of RAP can also provide good clinical results in routine clinical practice. A mean number of 4.5 anti-VEGF injections can ensure a good clinical stabilization in most patients affected by RAP. Further clinical-practice studies are needed to assess the effects of anti-VEGF molecules for each specific AMD subform.
Footnotes
Author Disclosure statement
No competing financial interests exist.