
Abstract
Abstract
Purpose:
To compare the effects of topical diclofenac and betamethasone on postoperative inflammation after combined sutureless cataract and vitreoretinal surgery in patients with macular hole (MH), epiretinal membrane (ERM), diabetic macular edema (DME), and rhegmatogenous retinal detachment (RRD).
Methods:
The study involved 180 eligible eyes that underwent the combined surgery, followed by treatment with topical diclofenac (n = 100) or betamethasone (n = 80) for 12 weeks. Maximum postoperative inflammation index (maxPOI), assessed by laser flare–cell meter, and intraocular pressure (IOP) were monitored. The relationships between maxPOI and total operation time or number of endophotocoagulations during surgery were investigated.
Results:
Postoperative inflammation peaked at 2 weeks and decreased thereafter in all 4 diseases, without significant differences between 2 treated groups. Postoperative IOP in MH and ERM was significantly higher in the betamethasone group. In DME and RRD, a greater number of endophotocoagulations increased maxPOI in both diclofenac and betamethasone groups, while longer operation time increased maxPOI only in diclofenac groups.
Conclusions:
In MH and ERM, topical diclofenac and betamethasone equally suppressed postoperative inflammation after the combined surgery, although diclofenac better controlled postoperative IOP. In DME and RRD, both drugs were equally effective in suppressing inflammation and controlling IOP, but diclofenac showed weaker suppression following longer operation.
Introduction
C
This prospective study compared the effects of the topical NSAID, 0.1% diclofenac, and the topical corticosteroid, 0.1% betamethasone, on postoperative inflammation in patients who underwent combined sutureless cataract and vitreoretinal surgery for various vitreoretinal diseases, including macular hole (MH), epiretinal membrane (ERM), diabetic macular edema (DME), and rhegmatogenous retinal detachment (RRD).
Methods
This prospective study was performed in accordance with the Institutional Guidelines of Tokyo Medical University Hachioji Medical Center Clinical Research Ethics Committee and was approved by its Institutional Review Board (No. 2013-002). The procedures conformed to the tenets of the World Medical Association's Declaration of Helsinki. Informed consent was obtained from each patient after they were provided with information on the procedures to be performed.
Patient eligibility
This prospective study recruited 200 eyes of 200 consecutive patients with MH, ERM, DME, and RRD, requiring cataract and vitreoretinal surgery at the time of initial visit in our clinic. Indications for surgery included subjective symptoms of visual dysfunction and clinically significant cataract necessitating surgery. Eyes with glaucoma, uveitis, high myopia (more severe than −6.0D), vitreous hemorrhage, prior ocular surgery, or prior intravitreous injections of any drugs were excluded.
Surgical procedure
All eyes underwent cataract surgery and vitrectomy at the same time by 2 experienced surgeons (K.Y. and M.S.) at Tokyo Medical University Hachioji Medical Center. Local anesthesia was induced by retrobulbar injection of 4 mL 2% xylocaine, followed by standard cataract surgery, consisting of continuous capsulorhexis, phacoemulsification, and implantation of a foldable acrylic intraocular lens (Eternity NX-70; Santen Pharmaceutical Co., Ltd., Osaka, Japan) into the lens capsule through a 3.0-mm corneoscleral incision. This was followed by standard 25-gauge 3-port pars plana vitrectomy with insertion of a transconjunctival cannula using a beveled trocar with a self-sealing valve. Following intravitreal injection of triamcinolone acetonide (TA: Maqaid; Wakamoto Pharmaceutical Co., Ltd., Tokyo, Japan) for better visualization, the posterior vitreous was removed using a wide viewing system. All eyes with DME and some with RRD underwent extensive removal of the peripheral vitreous up to the vitreous base with indentation. The inner limiting membrane of the macular area was peeled off in all eyes except those with RRD. Endophotocoagulation was performed as appropriate only in eyes with DME and RRD. This was followed by fluid–air exchange and subsequent endotamponade with 20% sulfur hexafluoride (SF6) gas. At the end of each operation, removal of the intraocular TA was visually confirmed, as was the spontaneous closure of all surgical wounds, including the corneoscleral incision and the 3 ports; eyes that required suturing for these wounds were excluded from this study.
Study design
All eyes were administered the topical antimicrobial drug, 0.5% levofloxacin ophthalmic solution (Clavid®; Santen Pharmaceutical Co., Ltd., Osaka, Japan), 4 times per day before and after surgery. Beginning the day after surgery, each eye was treated with topical 0.1% diclofenac (Diclod®; Wakamoto Pharmaceutical Co., Ltd., Tokyo, Japan) or topical 0.1% betamethasone (Rindelon®; Shionogi Pharmaceutical Co., Ltd., Osaka, Japan) 4 times per day, along with 0.5% levofloxacin ophthalmic solution, for 12 weeks. Eyes administered postoperative diclofenac or betamethasone were determined at random.
Eyes that developed an IOP greater than 25 mmHg during the 12-week period were administered antiglaucoma eye drops. Eyes requiring additional surgical procedures, including photocoagulation, vitrectomy, filtration surgery, and conjunctival injection of steroids, were noted and excluded from analysis.
Total operation times for cataract surgery and vitrectomy were recorded for each eye. Intraocular inflammation was assessed by anterior chamber flare (ACF) score, using a laser flare and cell meter 11 (LFCM1000; Kowa, Tokyo, Japan), before and 2, 4, 8, and 12 weeks after surgery. Maximum postoperative inflammation index (maxPOI) was defined as the maximum ACF score after the operation normalized to the initial ACF score of each eye. Best-corrected visual acuity (VA), measured with a logMAR chart (5 m; NEITZ LVC-10, Tokyo, Japan), and IOP, measured with an applanation tonometer, were assessed at the same times. The relationships between maxPOI and surgical parameters, including the total operation time and the number of endophotocoagulations during vitrectomy, if required, were investigated.
Statistics
Data are presented as mean ± standard deviation (SD). Differences between follow-up points in the same eyes were assessed using paired 2-tailed Student's t-tests, whereas differences between diclofenac-treated and betamethasone-treated eyes were assessed using the Mann–Whitney U test. The relationships between maxPOI and surgical parameters, including operation time and number of endophotocoagulations, were assessed by linear regression analysis. All statistical analyses were performed using SPSS ver. 11 software (Chicago, IL), with p < 0.05 considered statistically significant.
Results
Of the 200 consecutive eligible eyes, 191 eyes were recruited, including 106 eyes treated with diclofenac and 85 treated with betamethasone. During the postoperative period, no eyes with preoperative MH or ERM required additional treatment. Severe postoperative inflammation with expression of fibrin in the anterior chamber was observed for up to 4 weeks in 3 eyes with preoperative DME, including 2 treated with diclofenac (maxPOI = 6.22 and 5.57, respectively) and one treated with betamethasone (maxPOI = 5.29), and in 4 eyes with preoperative RRD, including 2 treated with diclofenac (maxPOI = 11.87 and 9.94, respectively) and 2 treated with betamethasone (maxPOI = 18.29 and 11.30, respectively); these 7 patients were excluded from this study. Two eyes with DME required repeat vitrectomy due to vitreous hemorrhage, one each treated with diclofenac (maxPOI = 4.48) and betamethasone (maxPOI = 3.66); and 3 eyes with RRD required repeat vitrectomy due to postoperative proliferative vitreoretinopathy (PVR), including 2 treated with diclofenac (maxPOI = 16.35 and 10.17, respectively) and one treated with betamethasone (maxPOI = 13.46). Overall, 5 eyes with DME, 3 treated with diclofenac and 2 with betamethasone, and 6 with RRD, 3 each treated with diclofenac and betamethasone, were excluded from postoperative statistical analysis. Thus, 180 eyes completed this study, including 100 treated with diclofenac (28 with MH, 30 with ERM, 24 with DME, and 18 with RRD) and 80 treated with betamethasone (24 with MH, 20 with ERM, 18 with DME, and 18 with RRD).
Patient characteristics
The demographic and clinical characteristics of the 2 patient groups are depicted in Table 1. There were no statistically significant differences in age, initial VA, ACF score, IOP, and total operation time between diclofenac- and betamethasone-treated eyes in the 4 disease subgroups. Although age and initial IOP did not differ significantly among these 4 subgroups, initial VA and ACF score were significantly higher in eyes with DME than in the other 3 groups, and initial IOP was significantly lower in eyes with RRD than in the other 3 groups. Total operation times for eyes with DME and RRD were significantly longer than those for eyes with MH and ERM.
Asterisk (*) indicates statistically significant difference among 4 diseases in each group.
ACF, anterior chamber flare; DME, diabetic macular hole; ERM, epiretinal membrane; IOP, intraocular pressure; MH, macular hole; OT, operation time; RRD, rhegmatogenous retinal detachment; VA, best-corrected visual acuity.
Operation
All eyes with DME underwent extensive removal of peripheral vitreous with indentation, as did 11 of the 36 eyes with RRD, 6 treated with diclofenac and 5 with betamethasone. All eyes with DME and RRD underwent endophotocoagulation. Among eyes with DME, the mean number of endophotocoagulation shots was similar in the diclofenac- and betamethasone-treated groups (432.7 ± 261.9 [range 106–967] vs. 595.7 ± 301.2 [range 107–1,156], p = 0.083). Similarly, there was no difference in mean number of endophotocoagulation shots in RRD eyes treated with diclofenac and betamethasone (673.8 ± 283.5 [range 256–1,256] vs. 544.0 ± 221.7 [range 208–911], p = 0.135).
Dynamic changes in ACF scores
Dynamic changes in ACF scores in eyes with each disease are shown in Fig. 1. In eyes with MH and ERM (Fig. 1a, b), ACF scores increased significantly after surgery and returned to their initial levels after 12 weeks, with no significant differences in ACF scores between the diclofenac and betamethasone groups at each time point for each disease. In eyes with DME and RRD (Fig. 1c, d), however, the ACF score increased significantly after surgery and remained higher over 12 weeks than before surgery. However, there were no statistically significant differences between diclofenac- and betamethasone-treated eyes at each time point for each disease.

Dynamic changes in ACF scores, as determined by the laser flare–cell meter, after combined sutureless cataract and vitreoretinal surgery in eyes with
Mean maxPOI was similar in diclofenac-treated and betamethasone-treated eyes with all 4 diseases, including MH (1.20 ± 0.22 [range 0.91–1.88] vs. 1.23 ± 0.18 [range 0.96–1.84], p = 0.344); ERM, (1.26 ± 0.26 [range 0.95–1.87] vs. 1.23 ± 0.31 [range 0.79–2.17], p = 0.600); DME (2.27 ± 1.69 [range 0.69–8.31] vs. 2.45 ± 1.64 [range 1.03–7.98], p = 0.474); and RRD (4.85 ± 3.90 [range 0.93–13.46] vs. 3.22 ± 3.52 [range 0.90–14.65], p = 0.179). Regardless of treatment with diclofenac or betamethasone, maxPOI was significantly higher in eyes with DME and RRD than in eyes with MH and ERM (Fig. 2a, b).
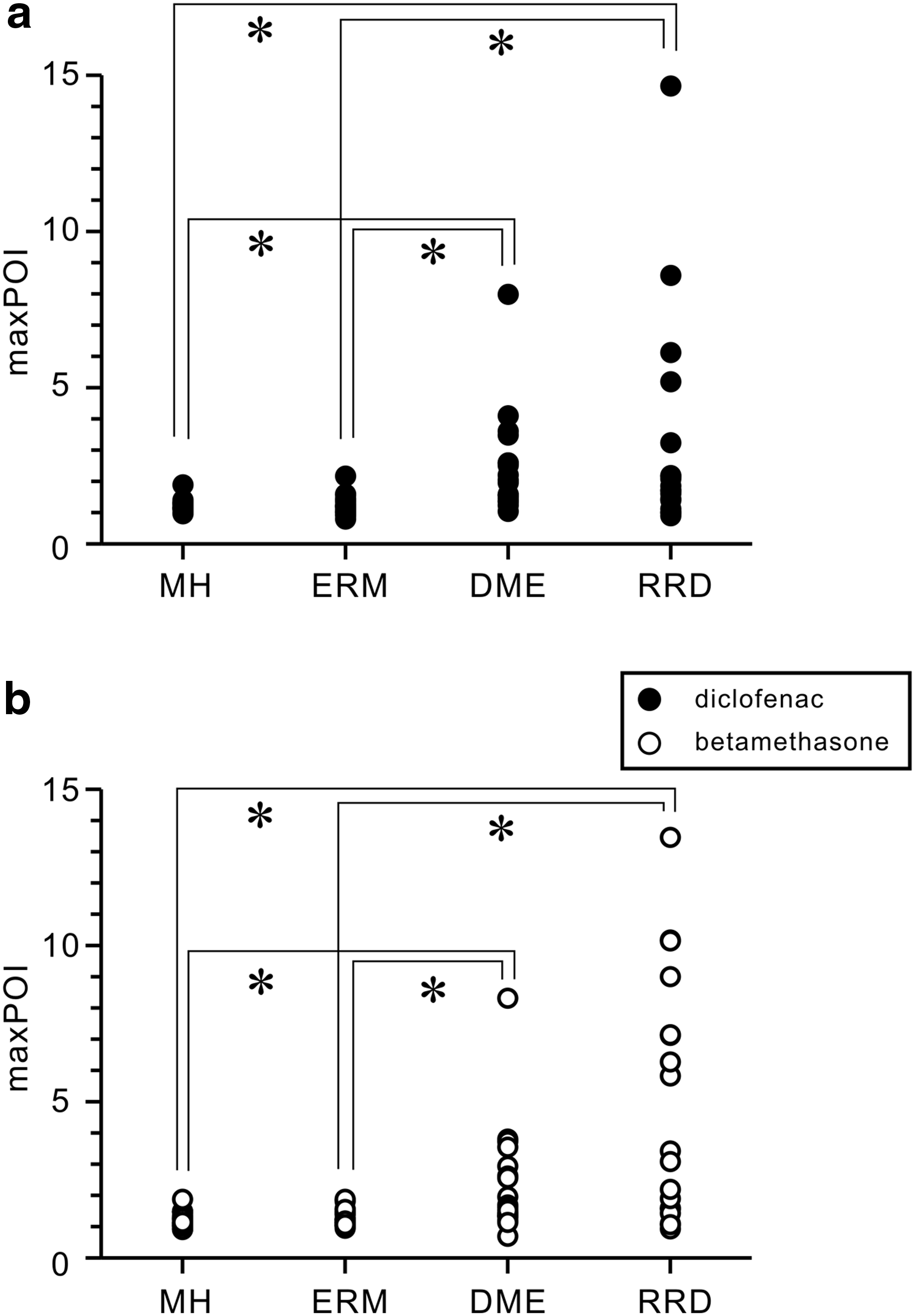
maxPOI in eyes with MH, ERM, DME, and RRD following treatment with topical diclofenac (
Dynamic changes in IOP
Dynamic changes in IOP in each group are shown in Fig. 3. In eyes with MH and ERM, IOP increased significantly after surgery, regardless of treatment. By 4 weeks, postoperative IOP in the diclofenac-treated eyes returned to their initial level, significantly decreasing thereafter until 12 weeks. In contrast, postoperative IOP in the betamethasone-treated eyes remained significantly higher than baseline during the entire 12 weeks, with significant differences in postoperative IOP between diclofenac- and betamethasone-treated eyes at 4 weeks (MH) and at 8 and 12 weeks (MH and ERM) (Fig. 3a, b). None of these eyes required treatment with antiglaucoma drugs.

Dynamic changes in IOP after combined sutureless cataract and vitreoretinal surgery in eyes with
In eyes with DME, IOP showed a transient increase for up to 4 weeks, regardless of treatment with diclofenac or betamethasone. IOP in the diclofenac-treated eyes returned to their initial levels after 8 weeks, but remained elevated in betamethasone-treated eyes for 12 weeks. However, there were no significant differences in postoperative IOP at any time point between diclofenac- and betamethasone-treated eyes (Fig. 3c). Five eyes, 2 treated with diclofenac and 3 with betamethasone, required antiglaucoma eye drops during the 12-week period due to IOP >25 mmHg, with these drops controlling IOP under 20 mmHg. IOP in eyes with RRD increased after surgery, regardless of treatment with diclofenac or betamethasone, and remained higher than initial levels throughout the 12-week treatment period. Only at 12 weeks was IOP significantly higher in betamethasone- than in diclofenac-treated eyes (Fig. 3d). Two eyes, one each treated with diclofenac and betamethasone, required antiglaucoma eye drops during the 12-week period.
Totally, 7 eyes in DME (5 eyes) and RRD (2 eyes) showed elevation of IOP and received endophotocoagulation shots of 741.7 ± 239.7 [range 502–1,156], which is significantly higher than the other photocoagulated eyes of 538 ± 275.9 shots [range 106–1,256] (p = 0.035).
Relationships between postoperative inflammation and surgical parameters
Figure 4 shows the relationship between maxPOI and total operation time in each group. There were no statistical correlations in eyes with MH (diclofenac: r2 = 0.137, p = 0.053, betamethasone: r2 = 0.068, p = 0.143) and ERM (diclofenac: r2 = 0.027, p = 0.385, betamethasone: r2 = 0.001, p = 0.898) groups. Significant correlations were observed in diclofenac-treated eyes with DME (r2 = 0.232, p = 0.031) and RRD (r2 = 0.393, p = 0.005), but not in betamethasone-treated eyes with DME (r2 = 0.128, p = 0.145) and RRD (r2 = 0.072, p = 0.281).
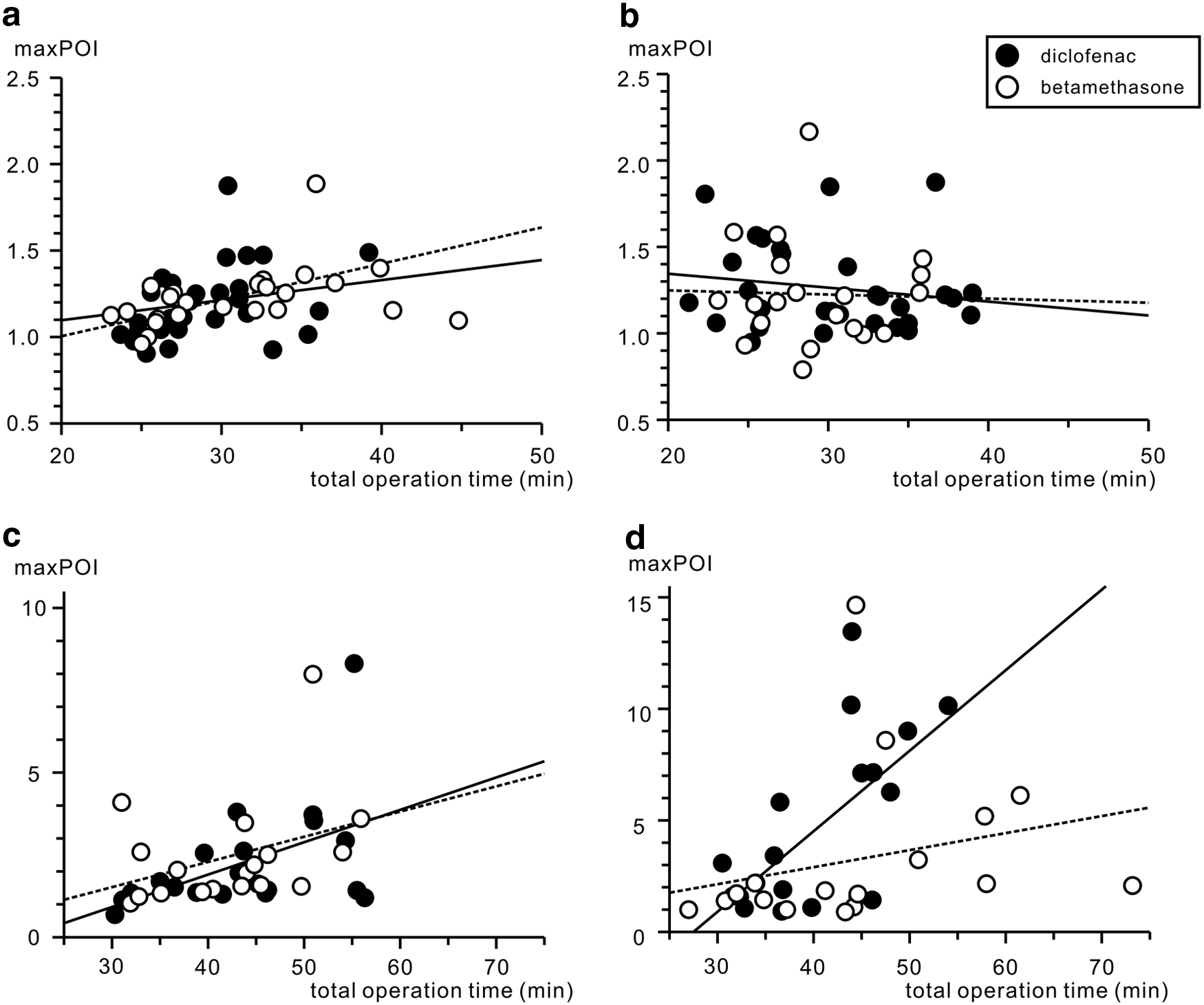
Relationships between maxPOI and total operation time in eyes with
The relationship between maxPOI and the number of endophotocoagulations is shown in Fig. 5. MaxPOI was significantly correlated with the number of endophotocoagulations in diclofenac-treated eyes with DME (r2 = 0.223, p = 0.036) and RRD (r2 = 0.416, p = 0.004), as well as in betamethasone-treated eyes with DME (r2 = 0.229, p = 0.045) and RRD (r2 = 0.237, p = 0.041).
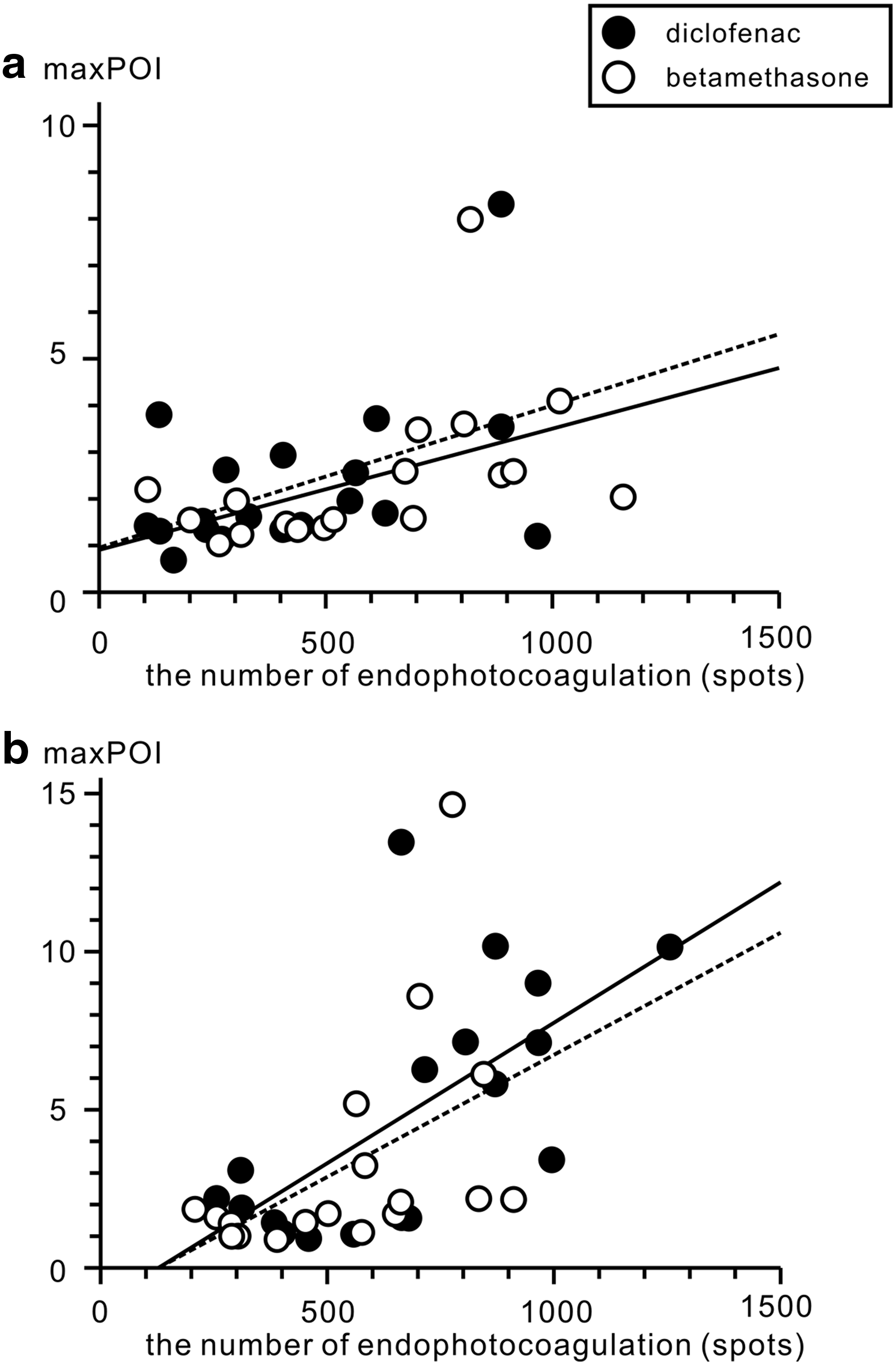
Relationships between maxPOI and the number of endophotocoagulations during surgery in eyes with
Analysis of RRD eyes showed that maxPOI was significantly higher in diclofenac-treated [8.02 ± 3.59 (n = 6) vs. 3.27 ± 3.08 (n = 12), p = 0.017] and betamethasone-treated [7.32 ± 4.71 (n = 5) vs. 1.64 ± 0.64 (n = 13), p = 0.004] eyes with than without indentation during vitrectomy.
Discussion
This prospective study quantitatively evaluated and compared the effects of a topical NSAID and a topical corticosteroid on postoperative inflammation after combined sutureless cataract and vitreoretinal surgery in patients with 4 vitroretinal conditions of MH, ERM, DME and RRD. The primary finding of this study was that dynamic changes in postoperative inflammation in these 4 vitreoretinal diseases did not differ significantly in eyes treated with these 2 topical anti-inflammatory drugs. In contrast, dynamic changes in postoperative IOP, especially in eyes with MH and ERM, were influenced by these 2 agents. That is, in diclofenac-treated eyes, IOP was transiently increased soon after the combined surgery and returned to its initial or a lower level within 1 month, whereas in betamethasone-treated eyes, IOP remained higher than the initial level over 3 months. In eyes with DME, IOP increased postoperatively and remained higher over 3 months, with no significant differences between diclofenac- and betamethasone-treated eyes. Postoperative IOP significantly increased in both diclofenac- and betamethasone-treated eyes with RRD, but was significantly higher in the latter only at 12 weeks.
Analysis of correlation between postoperative inflammation and total operation time showed that in eyes with MH and ERM, these parameters were not significantly correlated, regardless of treatment with diclofenac or betamethasone. In eyes with DME and RRD, however, postoperative inflammation showed a significant correlation with total operation time only in eyes treated with diclofenac, not betamethasone. Furthermore, postoperative inflammation was significantly correlated with the number of endophotocoagulations in both diclofenac- and betamethasone-treated eyes with DME and RRD.
Several studies have compared the effects of topical NSAIDs and corticosteroids on postoperative inflammation following cataract surgery.6,7,12,13 Topical NSAIDs not only more effectively suppressed postoperative inflammation but also showed stronger suppression of postoperative adverse effects, including cystoid macular edema, increased IOP, and ocular pain. To our knowledge, however, these classes of agents had not been compared in eyes undergoing combined cataract and vitreoretinal surgery. Combined cataract and vitreoretinal surgery has become widely accepted as safe and effective for patients with selected vitreoretinal diseases, including MH, ERM, DME, and RRD.3,14 Furthermore, sutureless phacoemulsification and sutureless vitrectomy have the advantages of faster rehabilitation, reduced postoperative inflammation and discomfort, and a single period of convalescence.3,14 Antibiotics and anti-inflammatory eye drops are usually administered after combined surgery, but the choice of anti-inflammatory drops, whether topical corticosteroid, topical NSAID, or both, is determined by each surgeon.
The anti-inflammatory effects of topical corticosteroids include inhibition of the enzyme phospholipase A2, inhibiting arachidonic acid synthesis; downstream prostaglandin synthesis by regulating cyclooxygenase (COX) expression; and downstream leukotriene synthesis by regulating lipoxygenase expression. 15 In addition, corticosteroids inhibit macrophage and neutrophil migration and decrease capillary permeability and vasodilation, 15 all suppressing postoperative inflammation. In contrast, topical NSAIDs specifically inhibit COX expression in the metabolic cascade of arachidonic acid and block prostaglandin synthesis. Although both drug classes have anti-inflammatory effects, topical NSAIDs are more effective than topical steroids in reestablishing the blood–aqueous barrier, as measured by anterior ocular fluorophotometry. 16 Moreover, these 2 classes are equally effective in suppressing postoperative inflammation and IOP elevation.
This study also found that ACF score was higher in patients with DME than in patients with MH and ERM. Postoperative inflammation remained high in patients with DME, not returning to preoperative levels after 3 months of treatment with either diclofenac or betamethasone. Intraocular conditions are unique in diabetic patients, with a breakdown of the blood–retinal barrier observed even in patients with preclinical retinopathy. 17 Furthermore, the concentrations of hemodynamic- and/or inflammation-related cytokines have been reported to be increased in the vitreous of these patients. 18 Thus, diabetic retinopathy is characterized preoperatively by chronic inflammation, which may be exacerbated by surgical intervention. Three eyes with DME, including 2 of 27 treated with diclofenac and 1 of 20 treated with betamethasone, showed severe postoperative inflammation and required repeated subconjunctival injections of corticosteroids. Thus, topical application alone may be insufficient to suppress postoperative inflammation in patients with DME.
Postoperative inflammation varied among individual patients with RRD, making it difficult to determine whether topical diclofenac or betamethasone was effective in suppressing postoperative inflammation. Three eyes with RRD experienced postoperative PVR, with maxPOIs of 16.35, 13.46, and 10.17. Higher ACF scores may be indicative of the risk of PVR. Our results suggest the need for more careful monitoring of eyes with greater numbers of endophotocoagulations and those that underwent removal of the peripheral vitreous with indentation and/or required a longer time for combined surgery.
In this study, only 5 eyes in the DME group and 2 in the RRD group experienced postoperative IOP >25 mmHg and required topical antiglaucoma drugs. Risk factors for elevated IOP following vitreoretinal surgery have been reported to include the number of photocoagulations, the severity of postoperative vitreous hemorrhage, and the use of gas tamponade. 19 In this study, gas tamponade was used in all eyes with DME and RRD. The mean number of photocoagulations in the 7 eyes with elevated IOP was significantly higher than the other photocoagulated eyes and may explain the higher transient IOP in the former. These findings suggest that postoperative IOP should be monitored carefully in DME and RRD eyes with higher numbers of endophotocoagulations.
Our finding—postoperative topical diclofenac and betamethasone monotherapy were equally effective in suppressing inflammation in eyes with MH and ERM, while diclofenac was more effective in suppressing elevated IOP, after combined cataract and vitreoretinal surgery—suggests that the use of diclofenac be recommended in these patients. In contrast, these 2 agents were equally effective in suppressing postoperative inflammation and IOP elevation in eyes with DME and RRD, although topical betamethasone showed stronger suppression following a longer operation time, suggesting the latter be used in patients with these conditions. Regardless of agent, however, the number of endophotocoagulations was correlated with the severity of postoperative inflammation.
This study has some limitations, including the residual effects of intravitreal triamcinolone acetonide, which could influence postoperative inflammation, but not impact comparative results. Thus, additional studies, with larger numbers of patients and longer follow-up time, are necessary to confirm these findings.
Footnotes
Acknowledgments
The authors thank Theranostic Instruments Research Laboratories for technical support of statistical analyses and useful comments. This study was supported by a grant-in-aid for scientific research from the Japan Society for the Promotion of Science to M.S. (JSPS KAKENHI No. 25462737) and to K.Y. (JSPS KAKENHI No. 15K10849).
Author Disclosure Statement
None of the authors has any conflicts of interest to be disclosed in this study.