
Abstract
Abstract
Purpose:
Chronic use of topical hypotensive therapies in glaucoma patients leads to chronic inflammation of the ocular surface, which decreases the success rate of long-term glaucoma management. The aim of this study is to evaluate the effect of topical palmitoylethanolamide (PEA) (Defluxa©), a well-known anti-inflammatory and analgesic agent, in suppressing the ocular surface inflammation associated with the use of hypotensive eye drops.
Methods:
In a pilot clinical trial, we enrolled 15 glaucomatous patients who received topical PEA (Defluxa) in addition to the current antiglaucoma drugs, while 15 glaucomatous patients did not receive any additional treatment. At 3 different time points (day 0, 15, and 30), signs of ocular surface involvement, adverse events, visual acuity, and intraocular pressure were assessed.
Results:
Topical PEA (Defluxa) was effective in increasing the Schirmer test (P < 0.05) and the tear film breakup time (T-BUT) (P < 0.0001), and improving the conjunctival hyperemia (P < 0.0001) by day 30, compared to baseline. Compared to control, by day 15, the conjunctival hyperemia score was significantly decreased in the PEA (Defluxa) group (P < 0.01), while the T-BUT and the Schirmer Test achieved a significant improvement by day 30 (P < 0.05; P < 0.01).
Discussion:
Our data suggests that topical PEA (Defluxa) is a safe, effective, and generally well-tolerated treatment to prevent or suppress ocular surface inflammation attributable to chronic glaucoma treatment.
Introduction
G
Palmitoylethanolamide (PEA) is an endocannabinoid mimetic amide with a well-known anti-inflammatory and analgesic activity. The anti-inflammatory action is caused by a reduction of inducible nitric oxide synthase, inducible cyclooxygenase, and several anti-inflammatory cytokines such as IL-1β, prostaglandin E2, and TNF-α by inhibiting the transcription of the proinflammatory nuclear factor NF-κβ. 25 The analgesic effect occurs by stimulation of peroxisome proliferator-activated receptor (PPAR)α, and indirectly by cannabinoid receptor 1 (CB1).26–29 Furthermore, several authors have demonstrated that oral administration of PEA increases the aqueous humor outflow.30–32 The aim of this study was to evaluate if PEA eye drops, when combined with hypotensive drugs, can reduce the inflammatory clinical signs of ocular surface disease (OSD) due to the chronic use of hypotensive eye drops.
Methods
In a pilot single masked prospective cohort study, we evaluated the effect on the ocular surface of topical application of PEA eye drops (Defluxa©) in patients under glaucoma treatment.
Therefore, 30 subjects were consecutively included from a continuous cohort of patients with chronic glaucoma who visited the glaucoma clinic at University Campus Bio-Medico of Rome, seeking consultation.
Glaucoma was defined as the presence of a repeatable visual field (VF) defect, corresponding with optic nerve damage. A glaucomatous VF change was defined as (1) a consistent presence of a cluster of 3 or more nonedge points on the pattern deviation plot, with a probability of occurring in <5% of the normal population, and with one of these points having the probability of occurring in <1% of the normal population, (2) a pattern standard deviation with P < 5%, and (3) a glaucoma hemifield test result outside normal limits. VF defects had to be reliable (false positive <15%; fixation losses and false-negative responses <25%) and confirmed in at least 2 tests, no more recent than 1 month.
The patients were enrolled into the 2 arms of the study, in a 1:1 ratio. Group 1, the study-drug group, received 1 eye drop of PEA (Defluxa) twice a day on both eyes during the study period in addition to their current glaucoma treatment, while the patients enrolled into the control group, group 2, had no additional treatment. Preservative-free 0.5 hyaluronic acid eye drops was prescribed to all patients enrolled in the control group, according to usual therapeutic schedule.
All the patients were committed to maintain their practices and therapeutic plan during the investigational period and within the 90 days preceding the screening visit.
Eligible patients were 18 years or older, with a diagnosis of glaucoma, and complaining about 2 of the following symptoms for at least 6 months before the screening visit: burning sensation, dry eye, photophobia, and foreign body sensation.
Furthermore, the inclusion criteria required Schirmer test <8 mm/5 min and a tear film break up time (T-BUT) <10 s.33,34 The presence/history of ocular infection or allergies as well as allergic rhinitis, active corneal stromal ulcer, and any history of eyelid infections within 3 months preceding screening visit were criteria for exclusion from the study. Moreover, patients with reported allergy to the components of the study drug were also excluded from the study.
Study approval was obtained from Human Studies Committee of the Campus Bio-Medico University of Rome. Informed consent was obtained from all the patients after providing a description of the nature and possible consequences of the treatment. Research was conducted in accord with the requirements of the tenets of the Declaration of Helsinki and the study drug was provided by Medivis as a solubilized formulation of PEA containing hyaluronic acid and cyclodextrin in unidose preservative-free vials (Defluxa).
Each visit, planned on days 0, 15, and 30, included assessment of best corrected visual acuity (BCVA), slit-lamp biomicroscopy, applanation tonometry, hyperemia conjunctival scoring, T-BUT, and Schirmer test type I. The mean conjuctival hyperemia score was assessed according to the Silk-Hu conjuctival redness grading (Cermedi Ltd.©), while the Schirmer test was performed without anesthesia by placing a narrow filter-paper strip (5 × 35 mm strip of Whatman #41 filter paper) in the inferior cul-de-sac. The patients gently closed their eyes until 5 min have elapsed and the strips were removed. Moreover, a standard T-BUT measurement was performed by instilling a fluorescein drop with anesthetic to the inferior fornix. After several blinks, the tear film was examined using a broad beam of the slit lamp with cobalt blue illumination. The time lapse between the last blink and the appearance of the first randomly distributed dark discontinuity in the fluorescein-stained tear film was measured thrice, and the mean value of the measurements was calculated. Adverse events related to the use of the study drug were also assessed. Finally, during the screening visit, the OSD Index (OSDI) questionnaire was also administered. OSDI is a 12-item validated questionnaire designed to provide a rapid assessment of symptoms related to ocular surface irritation and their impact on vision-related functioning in patients with dry eye disease (13–22 mild, 23–32 moderate, and over 33 severe). 35
The primary endpoint, measured after 30 days of treatment, was to evaluate the efficacy of the study drug to improve the mean T-BUT, to increase the mean Schirmer test type I score, and to reduce the mean conjunctival hyperemia score in patients under glaucoma treatments and complaining of ocular surface discomfort symptoms. Safety endpoints were measured as ocular and systemic adverse events related to the use of study drug. The effect of the study drug on the intraocular pressure (IOP) was a secondary endpoint of this study.
At the beginning of the study, the local clinicians were informed with a standardized letter introducing the study, the anticipated start date, and referral requests of potential patients.
All patients' scores for all outcome variables were calculated by averaging the data from both eyes in each group, with 95% confidence interval for each outcome measure (Table 1). The differences between mean values during the different time points were assessed with 1-way Anova nonparametric test, while the differences between mean values between the groups were assessed with paired samples t test. A P value of 0.05 was chosen as the limit of statistical significance.
BCVA, best-corrected visual acuity; IOP, intraocular pressure; T-BUT, tear breakup time.
Results
A total of 30 patients were consequentially assigned to either of the 2 groups as they access the glaucoma clinic. Baseline demographic and ocular characteristics among study groups were balanced, except for a significant higher discomfort perception (mean ± SD: 42.4 ± 26.7; 22 ± 7, P = 0.018) detected in the study drug group by OSDI questionnaire (Table 2).
OSDI, ocular surface disease index; SD, standard deviation.
Questionnaire (score 0–100).
Tear breakup time
On day 0, nonsignificant starting difference of T-BUT was evident between the 2 groups. However by day 15, T-BUT was significantly increased by 19% in group 1, and by day 30, the increase reached 29.7% compared to the baseline (Fig. 1a). No relevant difference has been found for different time points (day 15 and day 30) in group 2 compared to the baseline. By day 30, a significant improvement was evident in group 1 compared to group 2 (Figs. 1b and 4a; Table 3).
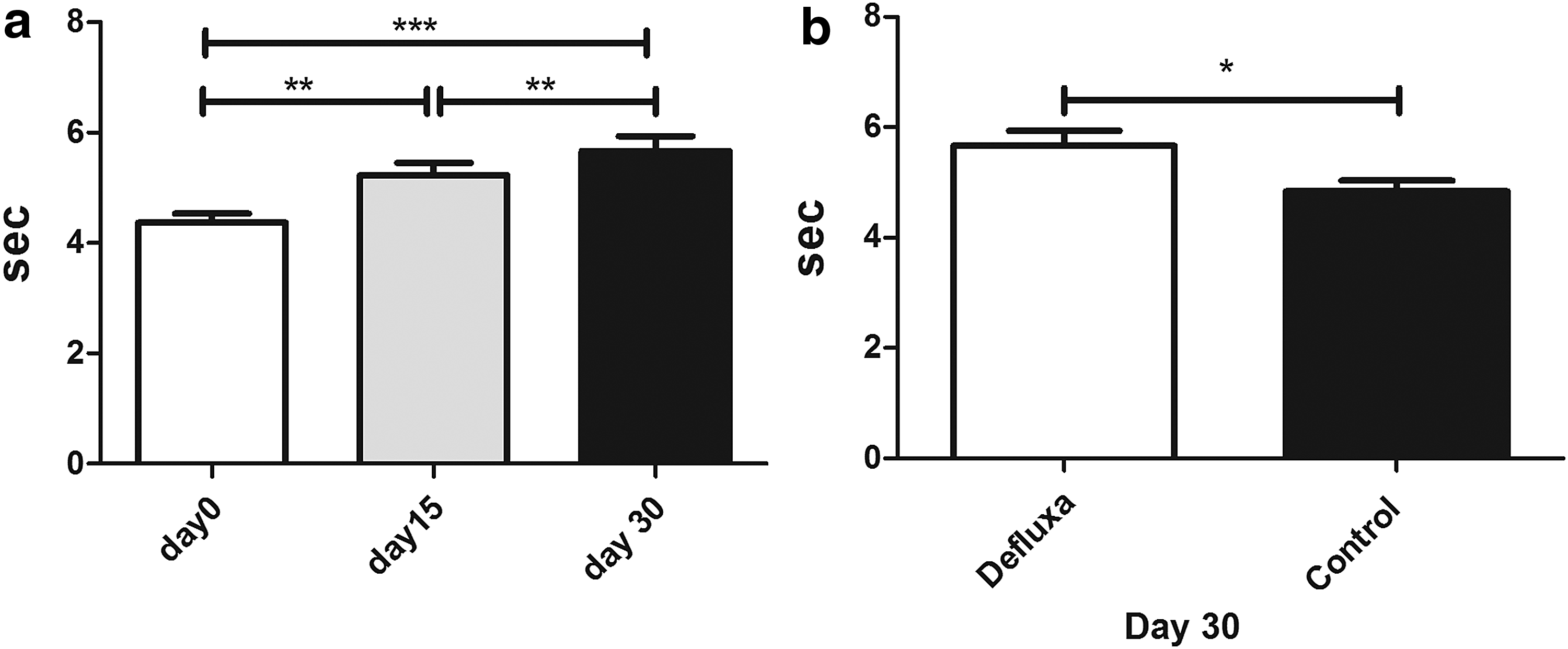
T-BUT. In the study drug group (group 1_Defluxa), a significant increase of T-BUT was noted at each time point compared to the baseline
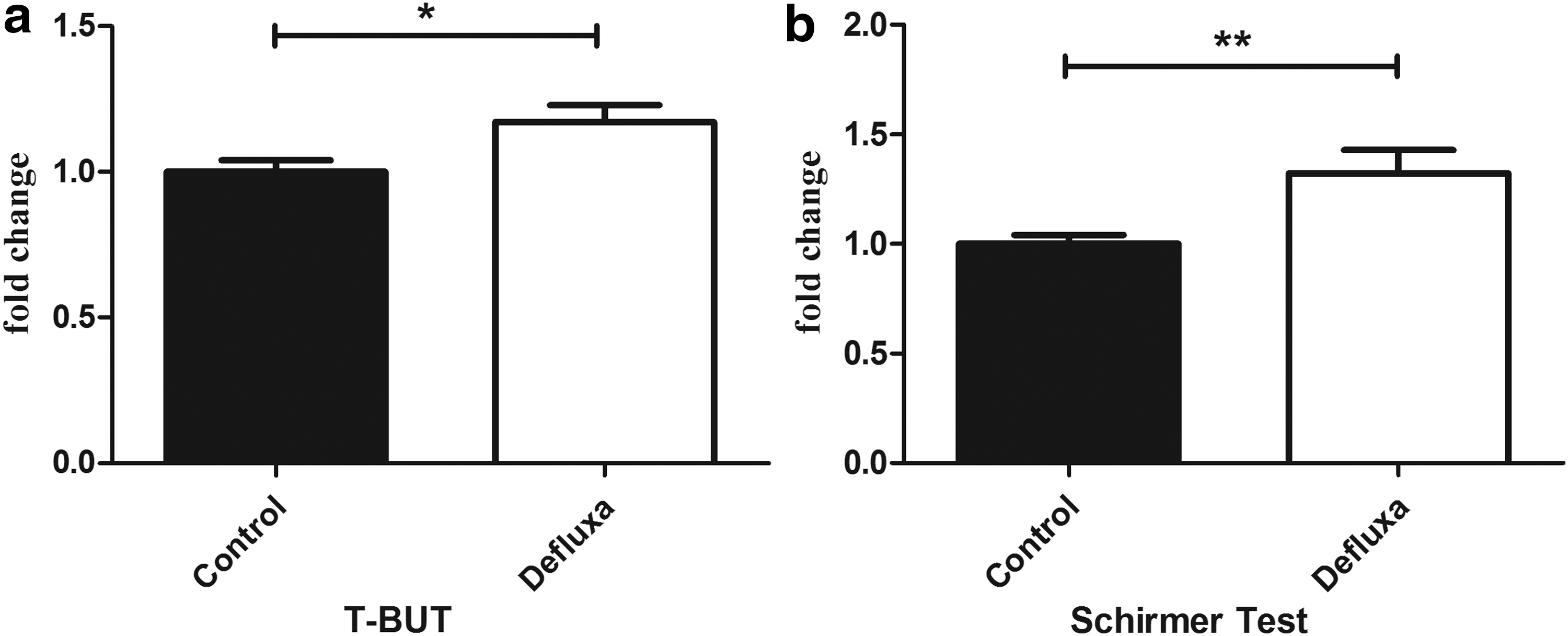
T-BUT and Schirmer Test values fold changes. At 30 days of treatment, the comparison of group 1 and group 2, expressed as fold changes form the control, showed a significant improvement of the T-BUT
In section A are reported data of Group 1, study drug group, at each time point. In section B are compared data of Group 1, study drug group, and Group 2, control group, at last time point.
CI, confidence interval.
Schirmer test type I
Overall improvement in mean Schirmer test score has been shown in group 1. By day 15, a not-significant improvement of 17% was detected, while a significant improvement of 26.9% was achieved by day 30 when compared to baseline in group 1. In group 2, no difference could be detected at the different time points compared to baseline (Fig. 2a). In addition, at the last time point, the Schirmer test was significantly increased in group 1 when compared to group 2.

Schirmer test values. In the study drug group (group 1_Defluxa), a trend of improvement of Schirmer test values was noted, which achieved significance by day 30 when compared to baseline. In addition, at the last time point, the Schirmer test was significantly increased in group 1 when compared to group 2
Patients in group 1 were subsequently divided in 2 subgroups based on the glaucoma treatments currently administered. Patients in single-drug glaucoma treatment (group A) showed a Schirmer test score difference at each time point, not significant compared to the baseline, while patients under multiple-drug glaucoma (group B) had a significant Schirmer test score improvement by day 30 compared to baseline. In addition, on day 30, group B showed a significant increase of Schirmer test compared with group A (Figs. 2b and 4b; Table 3).
Conjunctival hyperemia
At baseline, a significant difference in the conjuctival hyperemia scoring (mean ± SD: 2.2 ± 0.6; 1.8 ± 0.4, P = 0.007) has been underlined between group 1 and 2. In fact, an improvement in the ocular surface condition was detected in group 1 with a significant decrease in conjunctival hyperemia score estimated about 33.3% on day 15 and 36.6% on day 30 (Fig. 3a). In opposite, in the control group, no difference was observed between the different time points. Moreover, at each time point, a significant difference in conjuctival hyperemia scoring reduction was evident between group 1 and 2 (Fig. 3b, c; Table 3).

Conjunctival hyperemia scores. In group 1, a significant decrease in conjunctival hyperemia score was seen, which was estimated to be about 33.3% on day 15 and 36.6% on day 30
Nonprimary endpoints
At any time point, the study drug (group 1) did not show any significant increase of IOP compared to the control group. In addition, it was noted that the patients in the multidrug glaucoma treatment of group 1 showed a minimal IOP fluctuation rate, about 0.3% of difference in the different time points, while the patients in the multidrug glaucoma treatment enrolled in group 2 had a higher IOP fluctuation rate, about 4.7% (Fig. 5). Finally, the BCVA did not show any difference between the 2 groups.

Intraocular pressure fluctuation. Patients in multidrug glaucoma treatment in group 1 showed a minimal IOP fluctuation rate at different time points, compared to the higher IOP fluctuation in the multidrug glaucoma treatment patients enrolled in group 2. *P < 0.05; **P < 0.01; ***P < 0.001. IOP, intraocular pressure fluctuation.
Adverse events
No serious ocular and systemic adverse events attributable to the treatment occurred in either group during the study. All the patients enrolled completed the study without any major or minor adverse event. In addition to the principal ocular surface assessments during the treatment, participants were asked about discomfort and unpleasant sensation related to the drop installation. None of the participants reported any discomfort during the period of the study.
Discussion
In this open labeled, pilot, prospective cohort study, we assessed the effect of PEA (Defluxa) on ocular surface inflammation related to the long-term use of hypotensive eyedrops in patients with a previous diagnosis of glaucoma. We found a significant increase of tear stability, measured by T-BUT, in the study drug group when compared to both baseline and control group.
In addition, when the study group was compared to the baseline and the control group at the last time point, it showed a significant improvement in tear secretion. This increase is even greater when a higher number of medications were administered to the same eye. This is expected since a higher risk of OSD is attributable to the active component as well as to the preservatives of the antiglaucoma drugs, which induces allergic, toxic, and proinflammatory side effects.14,17 Finally, the significant reduction of hyperemia in those treated patients represents an important effect of the drug, since redness is an OSD sign that glaucoma treating patients mostly complain about. 10
PEA is well known for its anti-inflammatory properties. In fact, the activation of PPARs exerts anti-inflammatory activity by inhibiting the expression of proinflammatory genes, thereby reducing cytokines and metalloproteases, 36 and by stimulating the catabolism of proinflammatory eicosanoids. 37 A direct action in stimulating the cannabinoid receptors by a so-called “entourage effect” is also reported.38–40 Therefore, PEA (Defluxa) could improve the lacrimal glands functional impairment, typically related to the ocular surface inflammatory disease by directly inhibiting the NF-κB pathway by PPARα,36,41 inducing a documented increase in tear production.
This anti-inflammatory activity also enhances the quality and stability of the tear film. In fact, it has been reported that a decrease of inflammation induces an increase of mucin secretion by Goblet cells, and an improvement of the lipid secretion by the meibomian and accessory glands with an improved stability, and indirectly a reduction of osmolarity of the tear fluid, which is well-known sustaining factor of the positive feedback circle in DED. 42 Therefore the improvement of T-BUT is a relevant achievement in the study since the decreased tear stability is a critical sign of antiglaucoma drug-related OSD. The severity of the damage is directly dependent on the number of daily drops instilled and the duration of treatment. 14 In addition, T-BUT evaluation represents a noninvasive and simply available clinical examination, which could be an effective and early predictor of OSD in these patients, 8 since they usually present with repeated fluctuation on T-BUT scores and late onset of symptoms due to a reported decrease in corneal sensitivity.43,44
It is also well known that the endocannabinoid receptor stimulation inhibits cytokine production 45 and modulates immune cell migration 46 ; therefore, it directly affects the conjunctival vasodilatation, as showed by the reduced hyperemia in our patients, but could avoid the long-term effect of the chronic inflammation of the ocular surface, which can severely affect further glaucoma management by also increasing the failure rate of antiglaucoma surgical procedures.
Moreover, the fibrotic and scarring changes related to the chronic inflammation may have induced a functional or anatomical impairment of the glands and ocular surface, leading to a persistent and irreversible reduction of tear secretion and stability. Therefore, the chronic use of PEA on patients treated with antiglaucoma medications could not only reduce the risk of failure of a subsequent antiglaucoma surgical approach but also decrease the risk of an irreversible dry eye disease secondary to topical medication use.
Besides its anti-inflammatory effect, PEA also exerts a direct modulation of pain,36,47 thereby it has been studied extensively for its analgesic and neuroprotective effects, mainly in models of peripheral neuropathies.48,49 These data could explain its ocular tolerability and open an important debate about its use to reduce the discomfort associated with OSD in glaucoma treating patients, therefore it may increase patients' compliance to the antiglaucoma medications. In addition, the neuroprotective effect could explain the early increase in tear secretion, due to a more responsive nervous reflex. We can also speculate a prophylactic effect by PEA in preventing the reported anatomical damage of the corneal nerves, as a result of the chronic inflammation that occurred in dry eye disease.50–52
Endocannabinoids may also provide a tonic regulation of IOP.53,54 Several studies have shown that topical synthetic CB1 agonist lowers IOP in glaucomatous patients.55,56 In addition, Chen et al. 57 have detected lower PEA levels in ciliary body and choroid of glaucomatous eyes. Other authors have also reported a reduction of IOP in glaucomatous patients by administrating oral PEA 32 as direct effect on humor outflow.31,32,58 In this study, we did not note any significant variation in IOP in our patients by instillation of PEA; however, we could underline that group 1 showed lower mean IOP fluctuation compared with the control group between different time points in the patients in polytherapy (data not shown). We can speculate that this finding could be explained by the “entourage effect” of PEA enhancing the endocannabinoid effect on IOP.
However, the small sample size and the lack of a control group treated with a placebo limit the results of our study. An additional limitation is related to the lack of a systematic enrollment of patients with the same duration of antiglaucoma treatment. Therefore, a systematic controlled randomized clinical trial is needed to better evaluate the impact of PEA on ocular surface.
In this pilot study, the preinterventional and postinterventional evaluation of patient ocular discomfort and quality of life by standardized and approved questionnaires would have also been interesting.
In conclusion, glaucoma patients exhibit a chronic and predictable OSD, habitually underestimated in comparison to the potential blinding risk of the disease. However, the hypotensive eyedrops associated OSD, dramatically affects patients' daily quality of life, influences the adherence to the therapy, and impairs the surgical glaucoma treatment outcomes.59,60 Adding PEA (Defluxa) to the current glaucoma therapy could be an option that does not affect the IOP, improves the ocular surface signs of inflammation, probably enhances neuroprotection and analgesia, and finally increases the patients' compliance to antiglaucoma medications and thereafter the success rate of any further surgical intervention. Nevertheless, further studies are needed to describe the therapeutic or/and prophylactic indications of this novel selective anti-inflammatory medicine.
Footnotes
Acknowledgments
The contribution of the Fondazione Bietti in this article was supported by Ministry of Health and Fondazione Roma.
Authors' Contributions
A.D.Z. and S.B. contributed to the conception and design of the work; A.D.Z., S.B., and G.R. contributed to writing the article; G.R. and D.P. contributed to the acquisition; and A.M. and T.B.A. contributed to analysis, or interpretation of data for the work.
Author Disclosure Statement
No competing financial interests exist.