
Abstract
Abstract
Purpose:
Topical administration of the anti-inflammatory agent cyclosporin A (CsA) is recommended for long-term management of dry eye syndrome (DES), yet standard ophthalmic CsA preparations have been reported to be unstable. In this trial, the efficacy and safety of Clacier™ (based on a phase 3 study developed by Huons Co. Ltd.), a novel 0.05% CsA nanoemulsion formulation, are compared with those of the conventional Restasis® emulsion.
Methods:
Patients with moderate-to-severe DES were randomly assigned to receive topical 0.05% CsA in the form of Clacier or Restasis, to be administered twice daily for 12 weeks. The primary efficacy outcome was the change from baseline in corneal fluorescein staining scores at week 12; changes at weeks 4 and 8 were secondary endpoints. Additional endpoints included score changes from baseline in nonanesthetic Schirmer's test I, tear breakup time, ocular surface disease index, and conjunctival staining.
Results:
At week 12, corneal staining scores were improved in patients treated with Clacier and Restasis, with no significant difference between treatments (P = 0.41). Temporal conjunctival surface damage was significantly more ameliorated with Clacier treatment than with Restasis treatment (P = 0.034). Notably, tear film stability was improved more rapidly in Clacier patients at week 4 (P = 0.005) than in Restasis patients (P = 0.36). Improvements in tear production were comparable with both Clacier and Restasis treatments. Clacier did not increase the risk of adverse events as compared with Restasis.
Conclusion:
Treatment with Clacier alleviated clinical signs and symptoms of DES comparably to the commercially available Restasis, resulting in improved quality of life for patients. Clacier is an effective and safe therapeutic agent for DES.
Introduction
D
The principal lacrimal gland, ocular surface, meibomian glands, and connecting innervations function as an integrated unit to maintain ocular surface health, and any or all of its structures can be affected in DES, resulting in changes in tear film composition (hyperosmolarity). 2 The hyperosmolarity that is characteristic of DES triggers the secretion of inflammatory cytokines that activate T lymphocytes, allowing for their infiltration of the ocular surface. 3 This inflammatory environment gives rise to apoptosis of corneal and conjunctival cells, including the mucin-producing goblet cells responsible for tear film stability. 4 Inflammation also affects the function of tear-producing cells, 5 aggravating and unbalancing the composition of the tear film, and leading to tear film instability. An instable tear film leads to exposure and further damage of cells on the ocular surface, in effect maintaining a vicious cycle of inflammation and ocular surface damage. As such, DES can be considered a chronic disorder necessitating long-term therapy.
Disease severity is determined by both a subjective evaluation of symptoms and an objective measure of clinical signs that do not always correlate. 6 Verified symptom-oriented questionnaires, such as the Ocular Surface Disease Index (OSDI), are used to obtain an evaluation of dry eye condition. Diagnostic clinical tests provide objective evaluations of the ocular surface damage (e.g., fluorescein-based staining of the cornea and conjunctiva), tear film instability [e.g., tear breakup time (TBUT)], and tear secretion (e.g., nonanesthetic Schirmer's test I). As a consequence of the pathogenetic role of inflammation in DES, topical anti-inflammatory therapy is recommended for patients exhibiting moderate to severe dry eyes, even in the absence of clinically relevant signs of inflammation.5–7
Long-term use of ophthalmic drops containing the immunosuppressant cyclosporin A (CsA) has long been reported to be a safe therapy for DES, and has been approved by the FDA since 2003. 8 Various clinical trials have shown that topical application of the 0.05% CsA-containing eyedrops Restasis® (Allergan, Irvine, CA) can alleviate the clinical manifestations of DES, such as improving blurred vision and increasing tear secretion. 9 This is associated with a reduction of inflammation and less visible ocular surface damage.9,10 Nonetheless, the preparation of an aqueous ophthalmic solution of CsA remains a challenge because of its low solubility in water (20–30 μg/mL). 11 Emulsion preparations are one way to circumvent this problem, yet microemulsions (dispersed particle size 50–500 nm) are turbid and tend to separate over time through flocculation, creaming, coalescence, or Ostwald ripening processes. Ostwald ripening is characterized by molecular exchange from smaller to larger droplets through the continuous phase, resulting in a temporal increase of the average droplet size and a reduction of the interfacial area of the emulsion. 12 Reducing the dispersed phase particle size is one way to enhance emulsion stability, yet high-pressure emulsification methods currently exploited make it difficult to ensure long-term uniform product quality. High-pressure homogenizers reduce the thermal stability of the emulsion and limit the incorporation of temperature-sensitive components such as phospholipids. The resulting nanoemulsion has a large particle size distribution in the dispersed phase, which renders it more vulnerable to flocculation and creaming, lowering its long-term physicochemical stability. Consequently, the CsAs that are currently commercialized require the patient to shake them well before use to ensure the uniform application of the drug on the ocular surface. Clacier™ (Huons, Korea) is prepared without the use of high-pressure homogenization and displays enhanced emulsion stability, in terms of both dispersed particle size and pH, and can be stored for a long time. In addition, Clacier technology generates a transparent nanoemulsion with a homogeneous particle size of 50 nm or less, such that no preuse shaking is necessary and blurred vision or irritation is minimized upon topical application. The smaller particle size of Clacier nanoemulsion technology should provide an advantage for long-term ocular tolerance, CsA bioavailability, and emulsion stability, which have been reported as limitations to long-term Restasis use. 13
In this randomized clinical trial, the effectiveness and tolerance of Clacier, a novel Ministry of Food and Drug Safety (MFDS)-approved 0.05% CsA nanoemulsion, were compared with those of commercially available Restasis in patients suffering from moderate-to-severe DES. Changes in ocular surface damage, tear production, tear film stability, and general symptom severity were analyzed after 12 weeks of treatment.
Methods
Study population and procedure
This multicenter (6 study centers) double-masked study was conducted in accordance with the Declaration of Helsinki and was approved by the Kangbuk Samsung medical center institutional review board (IRB No. KBSMC201607-073).
To be considered eligible, patients had to be 21 years or older, have a best-corrected Snellen visual acuity ≥0.2 for both eyes at screening, and present clinical symptoms and signs of moderate-to-severe DES, categorized by a corneal fluorescein staining score ≥2 (Oxford grading) in at least 1 eye, a nonanesthetic Schirmer's test I score ≤10 mm/5 min for at least 1 eye [or if 0 mm/5 min (e.g., no tears), a nasal-stimulated Schirmer's test I ≥ 3 mm/5 min for the same eye], and a TBUT ≤10 s. In addition, patients had to have persisting dry eye symptoms despite conventional treatments (e.g., artificial tears). Women of childbearing age had to be nonpregnant and nonlactating at the start and for the duration of the trial.
Exclusion criteria included current or recent use of systemic drugs liable to affect dry eyes, use of contact lenses within 2 weeks before screening visit and during the study, use of punctal plugs within 1 month before screening visit and during the study, use of CsA within 3 months or topical ophthalmic CsA within 3 weeks before the screening visit, and current treatment with immunosuppressive or systemic steroids. Patients were also excluded if they had a presence or history of ocular disorders, including high intraocular pressure (>25 mmHg), abnormal eyelid function, ocular allergies (untreated or currently undergoing treatment), end-stage (irreversible advanced) lacrimal gland disease, conjunctival scars, or active ocular infections. Patients who had undergone other eye surgeries within 3 months before the screening visit were proscribed from the trial.
Other key exclusion criteria included a history of malignant tumors, renal or hepatic impairment, a known history of alcohol or drug use, participation in another clinical trial within the 3 months before screening, and hypersensitivity to the investigational drug. Patients could also be excluded at the investigators' discretion for other reasons that could affect the interpretation of the study.
In this trial, we sought to demonstrate that the study treatment was noninferior to the control drug in alleviating clinical signs and symptoms of DES, as measured by the change from baseline in corneal staining scores. We designed the study to have 80% power to detect a change of 0.289 in corneal staining scores, assuming an overall standard deviation of the treatment and control groups to be 0.43 (conservatively determined based on our review of previous studies and the current literature). The level of significance was set at α = 0.025 (one-sided). Based on these assumptions, 35 patients were required for each group, for a total of 70 patients overall. Taking into consideration a dropout rate of 20%, we aimed to register 44 patients for each group such that a minimum of 35 patients would have analyzable data.
After the initial screening visit, 101 patients were found to meet the eligibility criteria. Screening was followed by a 2-week run-in period during which patients were allowed to administer 1–2 drops of artificial tears (0.5% carboxymethylcellulose sodium; Hi-Eye Fresh eye drops, Huons, Korea) to both the eyes as needed. After run-in completion, a total of 48 patients were treated with Clacier (experimental drug) and 52 patients were given Restasis (active control drug), at the dosage of 1 drop per eye twice daily (12 h interval) for 12 weeks (Fig. 1). Study participants were assigned to treatment groups in a 1:1 ratio using a random number table generated using SAS v9.2 (block size = 4 or 8).
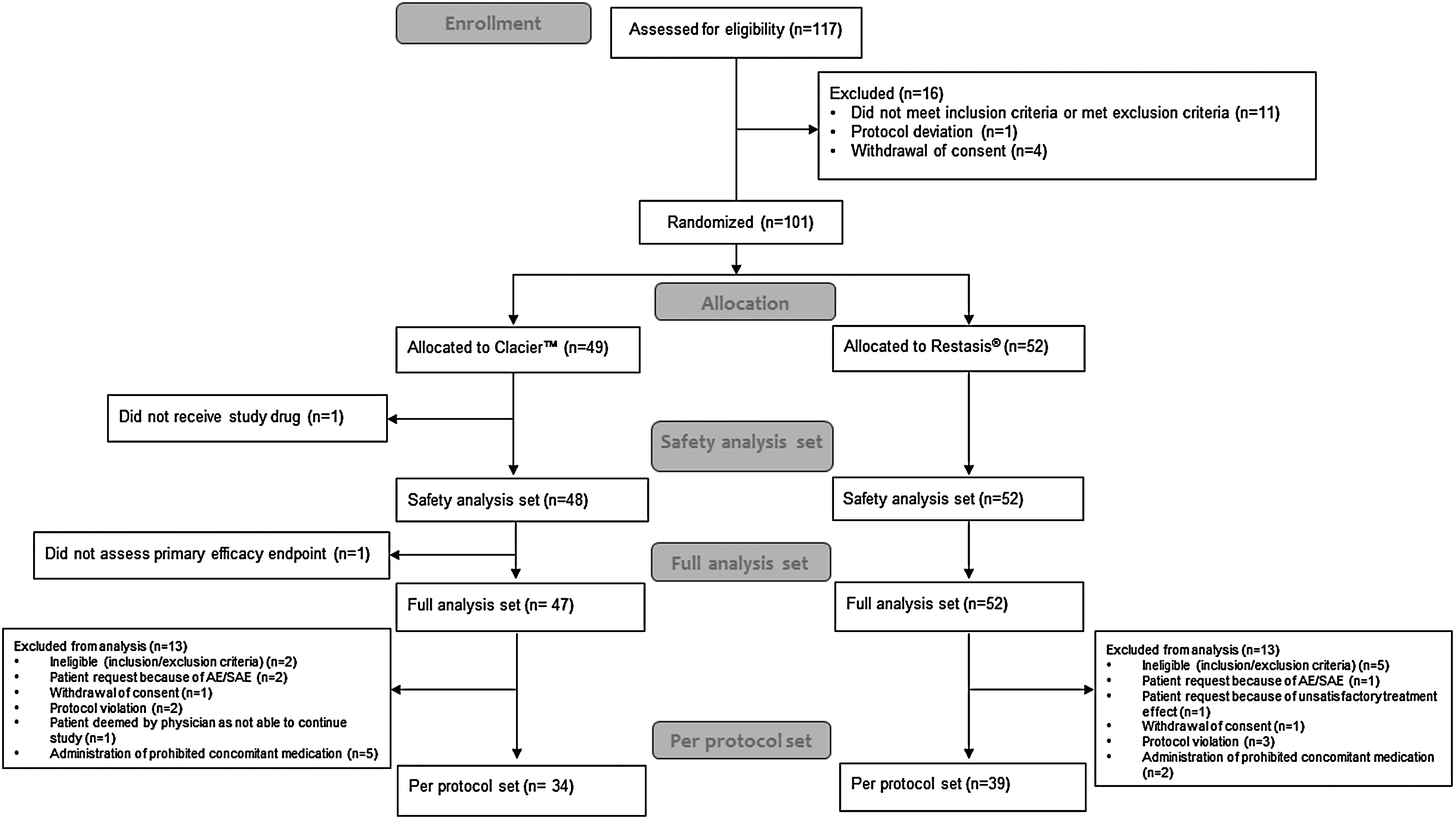
Patient disposition. AE, adverse event; SAE, serious adverse event.
Masking was maintained by packaging the study drug and control drug in indistinguishable boxes. Each institution had a nonmasked pharmacist and nurse responsible for storing/handling the drugs, but were not involved in any other aspect of the trial. Patients who received at least 1 dose of the investigational drug were included in the safety analysis set (total of 100 patients). One patient whose primary endpoint was not assessed was excluded from the full analysis set (FAS), which consequently consisted of 99 patients. A total of 26 patients were excluded from the FAS, such that the per protocol set (PPS) consisted of 73 patients (Fig. 1).
At day 0 of drug administration, pretreatment baseline scores were determined in patients for standard eye diagnostic tests. Tests were performed in the recommended practical sequence, starting with TBUT scores, followed by fluorescein corneal and conjunctival staining, and lastly, the nonanesthetic Schirmer's test I. 7 Patients' OSDI baseline scores were also determined. Patients were reassessed at weeks 4, 8, and 12 of treatment to measure any changes from baseline scores in the symptomatic eyes only. These measurements were used to determine efficacy endpoints of the trial. Throughout the trial, patients were allowed concomitant use of artificial tear medication (0.5% carboxymethylcellulose sodium; Hi-Eye Fresh eye drops) to be administered to the symptomatic eye as needed, and usage was documented.
Efficacy and safety endpoints
The change from baseline in corneal staining scores at week 12 of treatment with Clacier or Restasis served as the primary efficacy endpoint of the trial; the changes from baseline at weeks 4 and 8 were reported as secondary efficacy endpoints. Other key endpoints included changes from baseline in TBUT, conjunctival staining scores, nonanesthetic Schirmer's test I, and OSDI scores at weeks 4, 8, and 12. At all treatment time points, dry eye tests were performed in the recommended diagnostic sequence. 6 Patients' usage of concomitant artificial tears was recorded throughout the trial, and frequency of use was included as another efficacy endpoint.
The primary safety endpoint was the incidence of adverse events (AEs) in patients who had received at least 1 dose of trial drugs. Other safety endpoints were changes in best-corrected visual acuity and intraocular pressure as compared with results obtained during the screening visit. Clinical laboratory tests, a vital sign check, and a physical examination were also repeated at the end of the trial, or when patients dropped out, to evaluate changes in general health status as compared with those at screening. Drug tolerance was also included in the safety analysis.
Results
Patients
Baseline clinical characteristics were well balanced between both treatment groups, with similarities in duration of DES, past medical and surgical histories, and concomitant medication usage. The 2 treatment groups were also well matched with respect to demographic characteristics such as age, gender, weight, and height. General health status was consistent across patients as established by physical examinations, electrocardiogram, and clinical laboratory tests. A total of 26 patients who had received at least 1 dose of treatment did not complete the trial (Fig. 1) and were excluded from the PPS analysis; however, the patients' drop-out rate was equivalent between both treatment groups.
Primary efficacy endpoint
A significant improvement in corneal staining scores was observed in both Clacier and Restasis treatment groups at week 12. At trial commencement, baseline corneal staining scores were well matched between both drug groups, with a mean of 2.79 ± 0.73 for Clacier patients and 2.74 ± 0.59 for Restasis patients (P = 0.75) in the PPS. The mean corneal staining score was reduced by 1.74 ± 0.96 (P < 0.0001) in the Clacier-treated group as compared with a reduction of 1.56 ± 0.82 (P < 0.0001) in the Restasis group, demonstrating a significant reduction in corneal surface damage after 12 weeks of drug administration (Table 1). There was no significant difference in score reduction between treatment groups (P = 0.41).
P values for paired t-test.
For the primary endpoint evaluated on the PPS, the lower bound of a one-sided 97.5% confidence interval (CI) (−0.25) was determined to be greater than the clinical noninferiority margin (−0.289), establishing that Clacier was comparable with the active control Restasis (Table 2). This result was confirmed by repeating the analysis on the FAS by adopting the last observation carried forward (LOCF) method. Based on the FAS, the lower bound 97.5% CI (−0.23) was also found to be greater than the clinical noninferiority margin (−0.289), and Clacier was reconfirmed to be comparable with Restasis in reducing corneal staining scores (Table 2).
CI, confidence interval; FAS, full analysis set; PPS, per protocol set.
Secondary efficacy endpoints
Changes in corneal staining were also monitored throughout the trial period. At week 4, Clacier and Restasis patients exhibited corneal staining score reductions of 1.03 ± 0.87 (P < 0.0001) and 0.67 ± 0.70 (P < 0.0001), respectively. At week 8, scores were lowered by 1.41 ± 0.89 (P < 0.0001) in the Clacier group and by 1.08 ± 0.87 (P < 0.0001) in the Restasis group (Table 1). At both these time points, the score reduction was comparable between treatment groups (P = 0.05, P = 0.11, respectively).
A significant improvement in OSDI scores was reported at the end of the trial in both patient groups. Before treatment, Clacier and Restasis patients exhibited comparable baseline OSDI scores (28.80 ± 22.63 and 29.22 ± 19.17, P = 0.94). The mean OSDI scores of Clacier patients were significantly decreased by 0.80 ± 18.51 (P = 0.80, week 4), 5.09 ± 18.74 (P = 0.12, week 8), and 6.74 ± 18.85 (P = 0.045, week 12) (Table 3). In the Restasis group, OSDI scores were lowered by 3.58 ± 10.70 (P = 0.043, week 4), 8.28 ± 17.34 (P = 0.0050, week 8), and 9.88 ± 17.68 (P = 0.0012, week 12). There was no significant difference in the improvement of OSDI scores between both treatment groups at any time point (P = 0.44, P = 0.45, P = 0.47, respectively).
OSDI score = [total of all items answered × 100]/[total number of questions answered × 4].
P values for paired t-test.
OSDI, Ocular Surface Disease Index.
An improvement in tear film stability was observed in both treatment groups. In Clacier patients, TBUT was significantly increased by 0.66 ± 1.28 (P = 0.005, week 4), 1.29 ± 1.38 (P < 0.0001, week 8), and 1.88 ± 1.76 (P < 0.0001, week 12) (Table 4). Restasis patients were slower to exhibit significantly improved TBUT scores, and scores increased by 0.26 ± 1.76 (P = 0.36, week 4), 0.77 ± 1.60 (P = 0.0047, week 8), and 1.23 ± 1.50 (P < 0.0001, week 12). At all time points, changes in TBUT scores did not differ between treatment groups (P = 0.28, P = 0.14, P = 0.097, respectively).
TBUT = mean value of 3 repeated measurements.
P values for paired t-test.
TBUT, tear breakup time.
Tear production was gradually improved by both Clacier and Restasis administration, as evaluated by a nonanesthetic Schirmer's test I. Baseline scores were augmented by 1.03 ± 2.82 (P = 0.041, week 4), 1.21 ± 2.52 (P = 0.0087, week 8), and 2.26 ± 3.66 (P = 0.0010, week 12) in the Clacier group (Table 5). Restasis patients showed similarly improved scores with increases of 1.64 ± 2.28 (P < 0.0001, week 4), 1.28 ± 2.27 (P = 0.0011, week 8), and 1.90 ± 3.23 (P = 0.0008, week 12). Score changes were not significantly different between both treatment groups at all time points (P = 0.31, P = 0.89, P = 0.65, respectively).
Schirmer's test I = mm/5 min.
P values for paired t-test.
Changes to surface damage were evaluated for the temporal and nasal conjunctiva separately, as well as for the whole conjunctiva. Both Clacier patients and Restasis patients showed an improvement in temporal conjunctival staining scores and nasal conjunctiva staining scores at weeks 4, 8, and 12 (Table 6). The changes in temporal conjunctiva staining were significantly more pronounced in the Clacier group than in the Restasis group at weeks 8 and 12 (P = 0.0012, P = 0.034, respectively), whereas score improvements in nasal conjunctival staining did not differ significantly between Clacier and Restasis patients (P = 0.46, P = 0.21, P = 0.38) (Table 6).
P values for paired t-test.
Overall conjunctival staining was significantly reduced at weeks 4, 8, and 12 in both the Clacier group and the Restasis group (Table 6). By week 12 of treatment, changes in staining scores were not significantly different between both treatment groups (P = 0.99, P = 0.0067, P = 0.076).
Patients in both groups were allowed the concomitant use of artificial tear medication (0.5% carboxymethylcellulose sodium; Hi-Eye Fresh eye drops) as needed throughout the trial. Usage frequency (total number of eye drop applications during the trial) was used as an indicator of patient discomfort because of DES, and defined as a secondary efficacy endpoint. Clacier-treated patients used artificial tears for an average of 333.65 ± 140.02 times during the trial compared with 439.31 ± 312.51 times for Restasis patients, showing no significant difference in usage frequency between both treatment groups (P = 0.065).
The LOCF method was adopted to assess the FAS, yielding results similar to the PPS analysis.
Safety endpoints
The safety analysis set comprised 100 patients who received at least 1 dose of investigational product. During the trial period, there were 17 occurrences of AEs in 14 patients receiving Clacier (29.17%) and 18 in 15 patients taking Restasis (18.85%), showing a similar incidence rate of AEs between both treatment groups (P = 0.97) (Table 7). The Clacier group presented 12 incidences of mild AEs (70.59%) and 5 incidences of moderate AEs (29.41%), whereas all Restasis AEs were rated as mild. Most AEs (Clacier group, 76.47%; Restasis group, 88.89%) resolved with no sequelae. One patient receiving Restasis permanently terminated the treatment owing to an AE, but otherwise treatment was continued at the prescribed dosage in all patients. Two serious AEs were reported. A Clacier patient developed a cystocele (classified as definitely not related to treatment) and 1 Restasis patient experienced positional vertigo (probably not related to treatment). Both patients recovered with no sequelae. Five Clacier patients (10.42%) suffered an adverse drug reaction (ADR) compared with 4 patients (7.69%) in the Restasis group (Table 7). No serious ADRs were reported in either treatment group (Table 7). No clinically significant changes in vital signs were observed in either group, and reported changes in blood chemistry (Table 8) were not considered clinically significant between treatment groups. Best corrected visual acuity and intraocular pressure remained stable during the trial, and did not differ between the 2 groups. Drug tolerability was also assessed, and at week 12 of treatment, Clacier patients reported significantly less blurred vision than Restasis patients in both the right and left eyes (Table 9). However, the change in blurred vision from baseline scores did not differ between both treatment groups, and it was concluded that Clacier and Restasis showed similar endpoints regarding safety.
P value for χ2-test.
P value for Fisher's exact test.
ADR, adverse drug reaction; AE, adverse event; NA, not available.
Discussion
In this study, the novel MFDS-approved 0.05% CsA nanoemulsion Clacier was evaluated against the widely prescribed Restasis formulation for efficacy and tolerance in DES patients. Emulsion instability, low bioavailability, and poor ocular tolerance have been associated with Restasis, a conventional anionic oil-in-water CsA emulsion.9,13,14 Clacier is a transparent topical nanoemulsion formulation with a uniform dispersed particle size of 50 nm or less, which enhances emulsion stability and drug penetration. 15 Moreover, in vitro tests have shown that Clacier remains a transparent emulsion even in contact with large quantities of tear substitute (saline solution), which should minimize adverse effects, such as blurred vision, and improve patient acceptability (patent data on file). It is thought that the hydrophilic agent (ethylene oxide), which is used in Clacier to establish the small particle size of the homogeneous nanoemulsion, may be responsible for reducing irritation and blurring.
Fluorescein staining is a well-established method for evaluating ocular surface health. The highly hydrophilic fluorescein poorly penetrates healthy epithelial lipid layers but readily stains damaged corneal and conjunctival surfaces presenting disrupted cell-to-cell junctions. 16 In line with previously published data on topical CsA use in DES, 9 patients receiving Clacier exhibited a significant reduction in corneal and conjunctival staining, which indicates an attenuation of ocular surface damage. In agreement with previously published data on topical CsA use in DES, 9 treatment with the active control Restasis resulted in a significant reduction in corneal staining, indicating improved epithelial integrity of the cornea. Corneal staining scores improved as early as 4 weeks into treatment and continued to improve as the trial progressed. A comparable reduction of corneal staining was reported in Clacier-treated patients, and it was demonstrated that Clacier was no less efficient than Restasis in alleviating the clinical signs of corneal damage.
Conjunctival surface damage has been reported to precede corneal damage in DES and to be more severe. 17 Fluorescein-stained conjunctival surface damage was comparably reduced by either drug, although Clacier treatment was significantly more effective than Restasis in the temporal conjunctiva. The clinical relevance of this result is unclear, but it has been suggested that the distribution pattern of conjunctival staining can be used as a diagnostic tool. Specific staining of the temporal conjunctiva with Rose Bengal (RB), a derivative of fluorescein that stains the ocular surface inadequately protected by the tear film, 16 has been shown to differentiate Sjögren syndrome from DES. 18 In addition, the conjunctival staining pattern can indicate the progression of dry eye severity levels. In the early stage of the disease, RB staining is absent or limited to the nasal conjunctiva, but progresses to the temporal conjunctiva and eventually the cornea as disease evolves. 16 This staining pattern has also been reported using Lissamine green, a synthetic dye with a staining profile similar to RB.19,20 It is possible that the differences in conjunctival staining patterns observed with Clacier treatment as compared with those with Restasis are indicative of a more effective repair to the conjunctival surface. It can also be speculated that the integrity of the temporal conjunctival surface was more significantly improved with Clacier than with Restasis because the smaller dispersed particle size allowed for better diffusion of the drug.
The anesthetic Schirmer's test I is a measure of baseline tear production, whereas the nonanesthetic Schirmer's test I combines baseline tearing with reflexive tearing, which more fully reflects lacrimal gland function.9,21 To better gauge the benefits of Clacier treatment, it is best to consider the ocular surface and lacrimal gland as an integrated functional unit. Nonanesthetic Schirmer's test I scores were improved after Clacier administration in a manner comparable with Restasis, and in accordance with previously reported trials.8,9 Taken together with the ocular surface staining results, this suggests that Clacier treatment improves the epithelial quality of the ocular surface, which results in better sensory-stimulated reflex tearing. 8 These ameliorations of the ocular surface and tearing reflex were associated with greater tear film stability. Tear film stability progressively increased, and TBUT score amelioration was comparable between both treatment groups at the end of the trial. Notably, Clacier patients exhibited significantly improved TBUT scores more rapidly than the Restasis group, suggesting that Clacier is a faster acting treatment. It can be speculated that the rapid improvement of TBUT scores is a result of greater bioavailability of the drug because of the smaller particle size (50 nm or less) in the Clacier nanoemulsion.
Several mechanisms of action have been proposed to account for the therapeutic benefits exerted by topical CsA application. Local inhibition of cytokine production by activated T lymphocytes is one of the potential mechanisms. 22 T cell infiltrations and upregulation of inflammation markers on the ocular surface are readily observed in patients with DES. 10 Clinical improvement after CsA treatment is associated not only with a reduction in activated T lymphocyte numbers but also with a reduction of inflammatory mediators. 10 As previously reported, inflammation leads to apoptosis of ocular surface cells, and a decrease in mucin-producing goblet cell density is an early sign of ocular surface disease. 4 In turn, a decline in mucin-producing cells may contribute to the inflammatory component of DES. Exposure to topical CsA has been shown to augment goblet cell density. 23 Although this could simply be a reflection of a healthier lacrimal functional unit post-treatment, it may also be a direct effect of reduced inflammation levels. 23 Moreover, mucin helps establish the interface between the ocular surface and aqueous tear, which could explain improvements in tear film stability. 8 Through a mechanism that is not fully understood, topical application of CsA appears to accelerate tear secretion by releasing neurotransmitters from sensory nerves that interact with the parasympathetic component of the lacrimal functional unit. 24 It is evidently probable that the beneficial effects of CsA are not limited to its immunomodulating properties. Improved TBUT means functionally improved tear film from basement membrane and it applied patient's subjective symptoms. Further studies should be established to understand the exact correlation between improved TBUT and clinical symptoms.
The novel nanoemulsion Clacier is shown to improve clinical symptoms of DES, as well as to reduce patient discomfort, thus helping to regain a better quality of life. The efficacy of Clacier treatment is generally comparable with that of Restasis, with the added benefit of a more effective repair of temporal conjunctival surface damage with Clacier. Since many of the diagnostic test scores had not yet stabilized after 12 weeks of treatment, it will be interesting to see how Clacier compares with Restasis in a longer clinical trial. DES is a chronic condition that requires long-term treatment, and the stable, homogeneous, and transparent nature of Clacier makes it an easy-to-use ophthalmic preparation that ensures better patient compliance in the long term. Moreover, anti-inflammatory treatment is also salutary for the management of other dry eye conditions, such as after cataract surgery, 25 post-LASIK surgery, 26 and host-versus-graft disease. 27 Clacier could potentially provide a less irritable, easy-to-use topical alternative to systemic immunosuppressive therapies for a much wider range of inflammation-associated eye disorders.
Footnotes
Acknowledgments
All authors contributed to the generation of data and critically reviewed the article for intellectual content. The article processing charge was paid for by Alcon. This study was funded by Huons Co., Ltd.
Author Disclosure Statement
No competing financial interests exist.