
Abstract
Abstract
Purpose:
To evaluate the effect of epiretinal membranes (ERMs), detected with spectral-domain optical coherence tomography (SD-OCT), on the outcome of antivascular endothelial growth factor (VEGF) treatment for neovascular age-related macular degeneration (nAMD).
Methods:
A total of 434 eyes with treatment-naive nAMD were retrospectively included and analyzed. All patients were administered an initial series of 3 monthly loading injections of ranibizumab or aflibercept, followed by further injections as required. The visual and anatomical outcomes were compared between the eyes with ERMs and those without. Features of ERMs at baseline assessed with SD-OCT were evaluated and correlated with visual outcomes.
Results:
Sixty-eight eyes (15.7%) with nAMD presented ERMs at baseline. The mean best-corrected visual acuity (BCVA) of these eyes, expressed as the logarithm of the minimum angle of resolution, improved from 0.75 ± 0.48 (Snellen equivalent: 20/112) to 0.59 ± 0.44 (20/77) after 12 months of treatment (P = 0.021). Central foveal thickness also decreased from 381 ± 191 μm to 294 ± 167 μm (P < 0.001). Compared to the eyes without ERMs (366 eyes), the eyes with ERMs had a significantly thicker central fovea after treatment (P = 0.020). However, the intergroup differences in BCVA improvement were not significant. No significant association was found between visual outcome after treatment and ERM features on OCT at baseline.
Conclusions:
In eyes with nAMD, ERMs were infrequent. Central foveal thickness was significantly greater after anti-VEGF treatment in eyes with nAMD and ERMs. However, the presence of ERMs in eyes with nAMD did not affect visual outcome.
Introduction
A
To date, several studies have investigated the role of the vitreomacular interface status in the pathophysiological features and treatment response of neovascular age-related macular degeneration (nAMD). Vitreomacular adhesion (VMA) is more frequently reported in eyes with nAMD than in normal eyes, 2 and studies have shown that VMA could influence treatment and outcome in nAMD. The presence of VMA has also been associated with poor visual acuity.3,4 A recent study suggested that VMA or vitreomacular traction (VMT) was not associated with visual outcome, but was associated with the need for more frequent antivascular endothelial growth factor (VEGF) injections. 5
The process of ERM formation includes inherent inflammation 6 and the development of inflammation due to the tractional force exerted on the inner retina. 7 In addition, the ERM could be a physiological barrier for drug penetration into the macula, which could influence the therapeutic effect of anti-VEGF. However, unlike other vitreomacular interface diseases such as VMA or VMT, little is known about the association between ERM and nAMD.
The purpose of this study was to assess the therapeutic responses of patients with nAMD and ERMs after anti-VEGF treatment during a 12-month period, and to identify the optical coherence tomography (OCT) findings of ERMs that are predictive of good visual acuity after treatment.
Methods
We performed a computerized search and medical record review for patients who were newly diagnosed with nAMD and treated with anti-VEGF (ranibizumab [Lucentis®, Genentech, Inc., South San Francisco, CA] or aflibercept [Eylea®, Bayer HealthCare, Berlin, Germany]) injections between August 2013 and March 2015. All patients were examined and treated at the Retina Center of Kim's Eye Hospital at Konyang University College of Medicine. This study was approved by the Institutional Review Board of Kim's Eye Hospital, Konyang University College of Medicine. The entire study conduct adhered to the tenets of the Declaration of Helsinki (IRB No.: A-2016-011).
Subjects
The inclusion criteria were as follows: (1) age >50 years; (2) confirmation of nAMD with fundoscopy, spectral-domain OCT (SD-OCT, Spectralis; Heidelberg Engineering, Heidelberg, Germany), fluorescein angiography (FA), and indocyanine green angiography (ICGA) performed using a confocal laser scanning system (Spectralis HRA+OCT; Heidelberg Engineering) at the first visit; (3) no previous treatment; (4) treatment with anti-VEGF agents (aflibercept or ranibizumab); and (5) a minimum follow-up period of 12 months.
Differential diagnoses of nAMD subtypes, including typical nAMD, polypoidal choroidal vasculopathy (PCV), and retinal angiomatous proliferation (RAP), were made at baseline. PCV was diagnosed when ICGA revealed the presence of a characteristic polypoidal structure at the border of the branching vascular networks. RAP was diagnosed when the presence of a retinal anastomotic lesion or “hot spot” lesion was detected on ICGA. In addition, characteristic OCT features, such as intraretinal hemorrhage, intraretinal vascular anastomoses, and pigment epithelial detachment (PED) with overlying cystic retinal edema, had to be detected for a diagnosis of RAP.
The exclusion criteria were as follows: (1) evidence of end-stage AMD, such as central geographic atrophy or disciform scarring at baseline; (2) use of both aflibercept and ranibizumab (in cases of switching from ranibizumab to aflibercept, or vice versa); (3) other secondary choroidal neovascularization (CNV); (4) other concomitant ocular diseases, such as diabetic retinopathy, high myopia (spherical equivalent >6 diopters), vein or artery occlusion, and other ocular diseases that could affect visual acuity; (5) previous vitreoretinal surgery or surgery during the follow-up period; and (6) suspicious condition associated with the development of secondary ERMs, such as peripheral retinal breaks or inflammatory disorders of the retina and choroid.
Patient assessment and outcome measures
ERMs are thin membranes of fibrous tissue on the surface of the macula. In color photographs, ERMs appear as patches of irregular or increased reflection from the inner surface of the retina and are associated with fine traction lines and vascular tortuosity. 1 However, identifying minute ERMs such as cellophane maculopathy with fundus photography alone is difficult in cases of nAMD because the macula is deformed with CNV, retinal hemorrhage, or PED. Therefore, SD-OCT was used for detecting and evaluating ERMs in this study. SD-OCT scans were performed horizontally over the macular area (consisting of 19 or 31 horizontal lines [6 × 6-mm area]), and the diagnosis of an ERM was confirmed by the presence of hyperreflectivity of the membrane along the surface of the internal limiting membrane (ILM). Other vitreomacular interface abnormalities concurrent with ERMs, including VMA, VMT, and lamellar holes, were also evaluated.
VMA was defined as vitreous attachment and focal separation from the inner retina within a 3-mm-diameter center in the middle of the fovea. Whether straight up into the vitreous or pulled tangentially up and away from its original location or VMA was associated with deformation of the central 1 mm of the macula, defined as the presence of VMT. 8 Because the OCT image acquisition protocol used at our institution did not routinely include an optic nerve scan or B-scan ultrasonography, it was not possible to assess PVD when VMA was found. A lamellar hole (also called partial-thickness holes or pseudoholes) was defined as a concave foveal contour that dips lower and wider than the normal foveal depression.
When an ERM was detected at baseline, its OCT findings were evaluated for the presence of characteristic features, such as foveal involvement, concurrent corrugation (ridges and grooves) of the retinal surface, concurrent lamellar hole, or concurrent VMA or VMT (Fig. 1). In addition, central foveal thickness, defined as the vertical distance from the hyperreflective line of Bruch's membrane to the inner limiting membrane on fovea-centered SD-OCT images, was measured. Each measurement on SD-OCT images was performed with the Eye Explorer software (v. 5.6.4.0; Heidelberg Engineering Co, Heidelberg, Germany). The assessment of OCT images was performed by 2 retinal specialists (H.J.C. and H.S.K.) who were blinded to the patient information.

Examples of spectral-domain optical coherence tomographic findings of neovascular age-related macular degeneration combined with an epiretinal membrane (ERM). The ERM is confirmed by the presence of a hyperreflectivity of the membrane along the surface of the internal limiting membrane (white arrowhead), and it could involve the foveal area (gray arrowhead). The ERM could induce corrugation of the retinal surface (arrow) or a lamellar hole (gray asterisk). Concurrent vitreomacular adhesion or vitreomacular traction (asterisk) may be visible.
Intravitreal anti-VEGF treatment
All patients were administered a loading dose of 3 intravitreal anti-VEGF (ranibizumab [0.5 mg/0.05 mL] or aflibercept [2 mg/0.05 mL]) injections, with a 1-month interval between treatments. After the loading injections, additional injections were performed on an “as-needed” basis if any of the following conditions were observed: (1) if OCT revealed persistent fluid or hemorrhage involving the macula for 1 month following the previous injection and (2) an active CNV lesion was detected on FA, ICGA, or OCT examinations. All patients were followed up for 12 months on a monthly basis after initial treatment. Follow-up examinations, including best-corrected visual acuity (BCVA) measurement, fundus photography, and SD-OCT, were performed 3, 6, 9, and 12 months after the initial treatment visit. Additional FA, ICGA, and SD-OCT examinations were performed whenever recurrence was suspected. In accordance with previous studies that aflibercept was injected every 8 weeks during the maintenance,9,10 additional aflibercept was injected at 2-month intervals, while ranibizumab was injected at 1-month intervals after the loading injection.
Statistical analyses
SPSS version 13.0 (SPSS, Inc., Chicago, IL) was used for all statistical analyses. Frequencies were compared between groups by using chi-square or Fisher's exact tests. Analysis for changes in continuous variables was performed using paired t-tests. To investigate the baseline OCT findings related to good visual outcome after anti-VEGF treatment, multivariate logistic regression analysis was performed. Forward and backward stepwise regressions were performed using the likelihood ratio model, in which changes in the likelihood ratio statistic based on the maximum partial likelihood estimates for the covariate were used for variable selection. All tests were 2-sided, and a P-value less than 0.05 was considered statistically significant.
Results
Baseline characteristics
A total of 576 eyes (549 patients) were diagnosed with nAMD and treated at our institution during the study period. Among them, 142 eyes were excluded for the following reasons: follow-up loss within 12 months (120 eyes), vitreoretinal surgery because of severe ERM or concurrent complete macular hole during the study period (3 eyes), history of barrier laser use for peripheral retinal break or uveitis (3 eyes), or previous treatment with both ranibizumab and aflibercept (16 eyes). Finally, 434 eyes with nAMD were enrolled for analysis. All patients were South Korean, and the average age for the entire study group was 71.2 ± 6.9 years. Among the included eyes, 68 (15.7%) presented with ERMs at baseline. The patients' clinical details are listed in Table 1.
BCVA, best-corrected visual acuity; ERM, epiretinal membrane; logMAR, logarithm of the minimum angle of resolution; nAMD, neovascular age-related macular degeneration; PCV, polypoidal choroidal vasculopathy; RAP, retinal angiomatous proliferation; VEGF, vascular endothelial growth factor.
With regard to the various ERM features detected on OCT at baseline, foveal involvement of the ERM was most frequently found in 27 eyes (39.1%). Corrugation of the inner retinal surface due to an ERM was found in 26 eyes (37.7%); concurrent VMA and VMT were found in 12 eyes (17.3%) and 3 eyes (4.3%), respectively; and concurrent lamellar hole was found in 5 eyes (7.4%). No spontaneous resolution of ERM, VMT, or VMA was found during the 12-month follow-up.
At baseline, there were no significant differences between the eyes without ERMs (366 eyes) and the eyes with ERMs (68 eyes) with regard to age, sex, baseline BCVA, central foveal thickness, and mean lesion size. However, the eyes with ERMs showed significant infrequency of PCV than did the eyes without ERMs (P = 0.028; Table 1).
The mean number of intravitreal injections received by the patient group within 12 months was 4.86 ± 1.35 (range: 3–11 injections). Complications associated with injections, including endophthalmitis, traumatic lens injury, or retinal detachment, were not observed. In addition, none of the patients developed systemic complications, such as cerebrovascular accident, because of the intravitreal anti-VEGF injections.
Visual and anatomical outcomes
The mean BCVA of all subjects improved from 0.72 ± 0.44 logarithm of the minimum angle of resolution (logMAR [Snellen equivalent: 20/104]) to 0.53 ± 0.36 (20/67) after 12 months of treatment (P = 0.014). When comparing between the eyes without ERMs and eyes with ERMs, the mean BCVA of both groups showed significant improvements from baseline after 3, 6, 9, and 12 months (Fig. 2). In the eyes without ERMs, the mean BCVA (logMAR [Snellen equivalent]) improved from 0.69 ± 0.40 (20/97) to 0.52 ± 0.37 (20/66) after 12 months (P = 0.011). Similarly, in the eyes with ERMs, the BCVA improved from 0.75 ± 0.48 (20/112) to 0.59 ± 0.44 (20/77) after 12 months of treatment (P = 0.021). However, there was no significant difference between the 2 groups in terms of BCVA improvement (Table 2). The anti-VEGF injections tended to be more frequently required in the eyes with ERMs than in those without ERMs (mean injection numbers: 5.28 ± 1.44 vs. 4.67 ± 1.39), and the result showed a trend toward but did not reach statistical significance (P = 0.086; Table 2). Twelve months after treatment, good visual acuity (improvement of more than 3 lines after treatment) was observed in 22.1% (15/68) of patients with ERMs and in 32.2% (118/366) of patients without ERMs. However, the proportion of patients who showed improved visual acuity was not statistically significant (P = 0.178; Table 2).
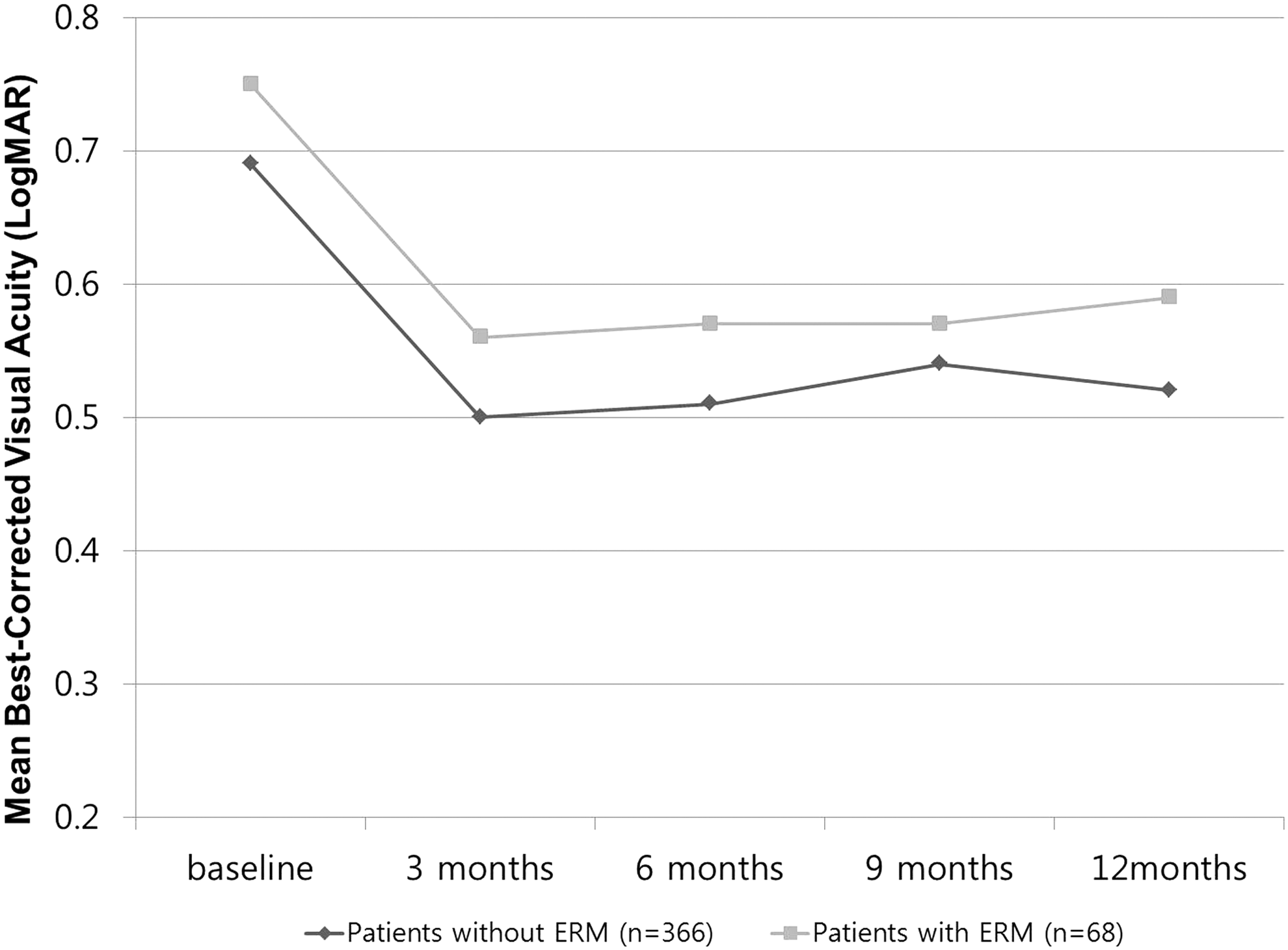
Changes in mean best-corrected visual acuity (BCVA), expressed as the logarithm of the minimal angle of resolution (logMAR), during a 12-month follow-up of patients with neovascular age-related macular degeneration treated using antivascular endothelial growth factor agents. In both eyes with ERMs (68 eyes) and without ERMs (366 eyes), significant visual improvement was achieved and maintained over 12 months. However, there was no significant difference between the groups in terms of BCVA improvement.
In both groups, the mean central foveal thickness also decreased gradually and significantly during the 12-month follow-up period (Fig. 3): from 351 ± 164 μm to 245 ± 183 μm in the eyes without ERMs, and from 381 ± 191 μm to 294 ± 167 μm in the eyes with ERMs (P < 0.001 in both cases). Central foveal thickness was significantly larger at 12 months after anti-VEGF treatment in the eyes with ERMs (294 ± 167 μm) than in the eyes without ERMs (245 ± 183 μm) (P = 0.020; Table 2). However, the changes in central foveal thickness 12 months after treatment were also not significantly different between the 2 groups, with a decrease of 107 μm from baseline in the eyes without ERMs and of 87 μm from baseline in the eyes with ERMs (P = 0.368; Table 2).
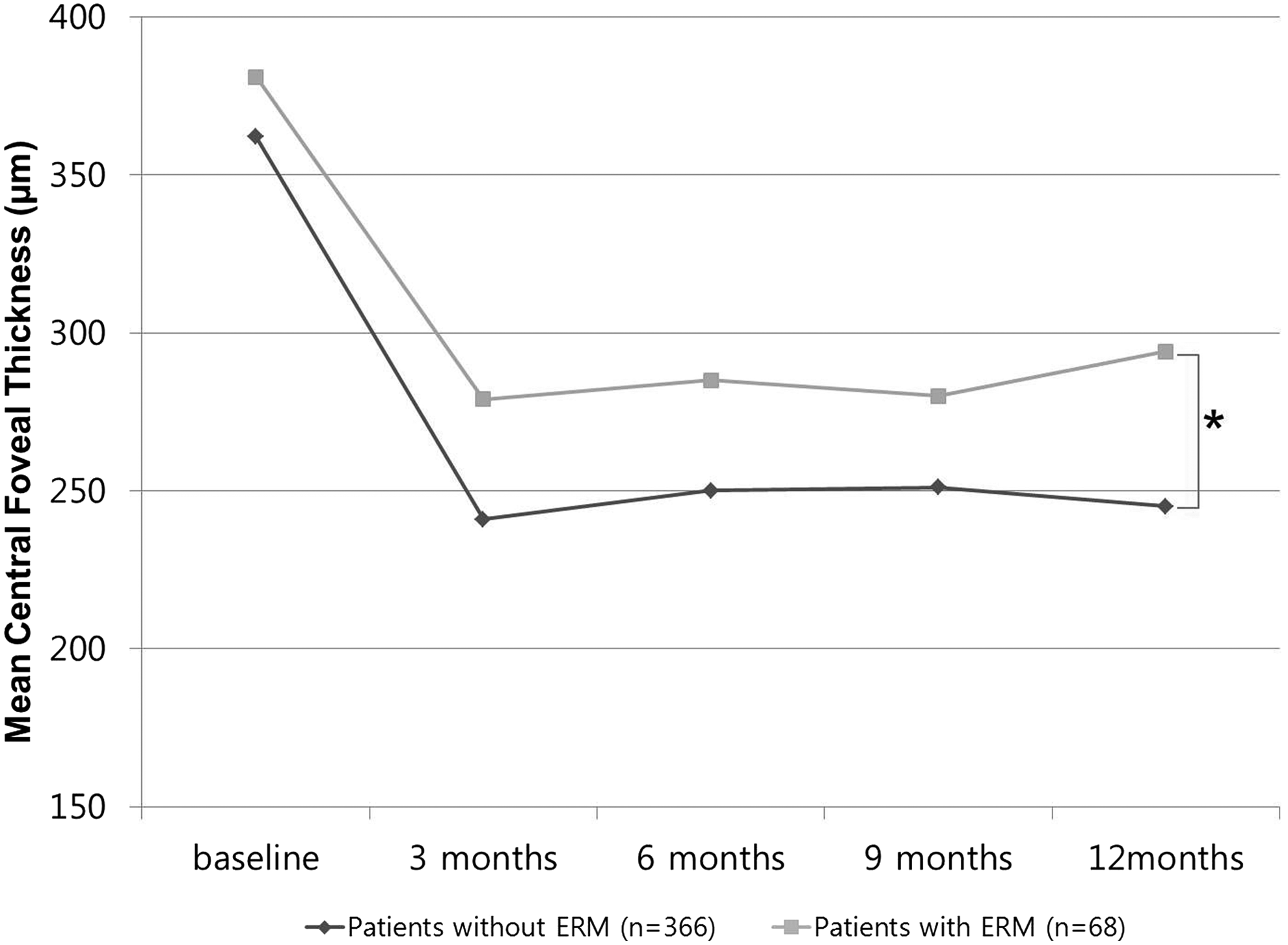
Changes in mean central foveal thickness during a 12-month follow-up of patients with neovascular age-related macular degeneration treated using antivascular endothelial growth factor agents. In both eyes with ERMs (68 eyes) and without ERMs (366 eyes), the mean central foveal thickness significantly decreased throughout the 12 months. The central foveal thickness of the eyes with ERMs was significantly larger than that of eyes without ERMs (*P < 0.05).
Predictive factors of good visual acuity and baseline OCT findings of ERM
The univariate logistic regression analysis showed that the presence of a concurrent lamellar hole in the eyes with ERMs was associated with good visual acuity (improvement of more than 3 lines) after anti-VEGF treatment (Table 3). However, when the data were analyzed using multivariate logistic regression (adjusting for age, sex, baseline BCVA, baseline central foveal thickness, lesion size, and injection number), no OCT finding was associated with good visual acuity after treatment (Table 3).
All variables are categorical variables.
Adjusted for age, sex, baseline BCVA, baseline central foveal thickness, lesion size, and number of injections.
CI, confidence interval; OCT, optical coherence tomography; OR, odds ratio; VMA, vitreomacular adhesion; VMT, vitreomacular traction.
Discussion
Similar to other age-related disorders, including nAMD, ERMs increase in frequency with age.11,12 The associations between ERMs and nAMD have not been sufficiently explored; however, several investigations suggest possible associations. One of the important pathophysiological mechanisms underlying ERM formation involves retinal glial cells, hyalocytes, and their transdifferentiation into fibroblasts/myofibroblasts. 1 A recent study showed that preretinal glial cells were more frequently found in eyes with nAMD than in age-matched control eyes. 13 Although these structures may be benign, they may exert traction on the retina as they spread along the vitreoretinal interface and develop into true ERMs. Indeed, retinal changes such as inflammation may also stimulate glial cell proliferation and/or migration along the vitreoretinal surface. 14 In addition, inflammation is one of the important pathophysiological components for nAMD development. 15 Hence, it could be assumed that the probability of ERMs is higher in patients with nAMD than in those without nAMD.
In the current study, 15.7% of patients with nAMD (all South Korean) presented ERMs at baseline. Previous studies have documented ERM prevalence rates of 8.4% among 2044 Chinese subjects aged 50 years or more, 16 and of 5.7% among 1,758 Japanese subjects. Although a direct comparison could not be made to these studies, our findings suggested a higher frequency of ERMs in patients with nAMD than in the normal population. Various ethnic- and population-based studies have reported wide variations in ERM prevalence rates (ranging from 2.2% to 18.5%).1,8 Therefore, population-based cross-sectional studies should be conducted in the future to determine the exact prevalence of ERMs in patients with nAMD.
To date, ERM is not considered at baseline because most clinicians concentrate on other parameters, such as hemorrhage, presence of fluid, and PED, in the setting of nAMD. However, we hypothesized that ERMs, owing to their peculiar characteristics, could affect the therapeutic effect of anti-VEGF agents. First, an ERM is a sheet of fibrotic tissue that varies in thickness from a single layer of collagen with interspersed cells to a thicker, multilayered fibrocellular proliferation, 17 which could act as a physiologic barrier for drug penetration into the macula. In addition, astrocytes and activated Müller cells are important components in ERM formation, 1 and they both express VEGF 13 that may prevent drugs from reaching their target in the outer retina. Another possible factor is the inflammation caused by ERMs. Previous studies have shown that VMA could affect visual outcome after anti-VEGF treatment in patients with nAMD, and one of the proposed mechanisms is the inflammation caused by VMA.7,18 The process of ERM formation includes inherent inflammatory changes, 6 as well as the development of inflammation due to the tractional force exerted on the inner retina. 7
However, in the current study, the presence of ERMs did not affect visual outcome after anti-VEGF treatment for nAMD, and the proportion of patients with a good prognosis after treatment (improvement of visual acuity by more than 3 lines) showed no significant difference between the groups with and without ERMs. In addition, we failed to identify specific OCT findings of ERMs that could be associated with good visual acuity after treatment. Our results suggest that clinicians need not consider ERMs as significant prognostic factors for nAMD or while deciding the therapeutic plan when they perform anti-VEGF treatment. However, a long-term follow-up study and monitoring for ERMs would be required, because in most cases, ERMs progress slowly over several years. 19
The number of injections tended to be higher in the eyes with ERM than in eyes without ERM in our study, even though there was no statistical significance. It could be speculated that more frequent injections were needed in the eyes with ERM because of decreased drug penetration due to the ERM. Another possibility is the presence of ERM-related cystoid changes in the macula. In a study that used an as-needed reinjection protocol for nAMD, the cystoid changes on OCT were considered to indicate recurrent or remnant CNV activity, which necessitated additional injections. 20 However, intraretinal cystoid changes were frequently concurrent with the ERM itself, 21 and not only with nAMD. Also, whether cystoid changes originated from CNV activity or from ERMs could not be easily distinguished. Hence, more frequent injections may be required because of the presence of cystoid changes due to ERMs.
Unlike visual outcome, central foveal thickness of the eyes with ERMs was significantly larger than that of the eyes without ERMs after anti-VEGF treatment in the study. Considering the changes in central foveal thickness from baseline to 12 months after treatment were similar between the eyes with and without ERMs in this study, the result could be associated with a thickened retina due to ERMs rather than a difference in the therapeutic effect of anti-VEGF agents. Therefore, clinicians should be aware that central foveal thickness would not always be correlated with visual outcome in the eyes with nAMD and ERMs.
Pars plana vitrectomy is often indicated in patients with ERMs who have a decrease in visual acuity, metamorphopsia, double vision, or difficulty using their eyes together.1,22 Visual acuity gains after vitrectomy for ERMs have been reported to be relatively modest, and visual acuity changes may not fully reflect symptomatic relief.23,24 The visual outcomes after vitrectomy are highly variable; while some patients do show a gain in visual acuity, 10% to 20% of the patients have unchanged or worse vision following surgery.1,23,24 Vitrectomy is also well known to improve metamorphopsia in patients with ERMs. Kimura et al. 25 recently reported that 6 patients with nAMD and concurrent ERMs or VMT, which was resistant to anti-VEGF therapy, showed improved visual acuity after vitrectomy, including ERM and ILM peeling. However, it remains unclear whether additional vitrectomy for nAMD and concurrent ERMs could improve visual acuity in terms of therapeutic efficacy. Future studies on the therapeutic effect of vitrectomy in patients with nAMD and concurrent ERMs are warranted.
Interestingly, eyes with PCV showed a significantly low incidence of ERMs in this study. Previous studies have shown that the proportion of PVD was higher and the frequency of VMA was lesser in eyes with PCV than in eyes with typical nAMD. 26 In addition, VMA would not have affected therapeutic efficiency after anti-VEGF treatment in the eyes with PCV. 27 These results suggested that the vitreomacular interface status might have a lesser association with PCV than with typical nAMD in terms of pathophysiology or anti-VEGF therapeutic effect. The exact association between nAMD subtypes and vitreomacular interface disorders also needs to be explored in the future.
To the best of our knowledge, the current study represents the largest published cohort series to date comprising patients with nAMD and concurrent ERMs, despite the relative infrequency of such a condition. However, it has several limitations, including its retrospective nature. First, we could not exactly evaluate ERM severity because of various reasons. The severity of traction, fibrosis, size of the ERM area, and so on could not be measured as the macula was already deformed because of nAMD, which caused retinal hemorrhage, PED, and distortion of the macula. Moreover, it was almost impossible to make a traditional classification of ERM, for example, cellophane maculopathy or macular pucker, 28 because most cellophane maculopathies could not be detected on fundus photography, and some macular puckers (preretinal macular fibrosis) were only detected on OCT. Therefore, we had no choice but to evaluate the baseline OCT features of ERM for our analysis. Second, ranibizumab and aflibercept were not strictly differentiated in the current study. In a previous study, the 2 agents have been shown to have therapeutic equivalence in patients with nAMD during 96 weeks. 10 However, the penetration of these drugs through the ERM could be different because of the differences in their molecular weights and the presence of the Fc portion of human immunoglobulin G1 in aflibercept. 29 Hence, we conducted our study after confirming that there was no significant difference in therapeutic efficacy between ranibizumab and aflibercept in patients with ERMs (data not shown); therefore, in our opinion, the result would not be biased because of the type of anti-VEGF agent used.
In conclusion, 15.7% of patients with nAMD presented ERMs at baseline. Central foveal thickness was significantly larger after anti-VEGF treatment in the eyes with nAMD and ERMs than in the eyes without ERMs; nevertheless, compared to eyes without ERMs, the presence of ERMs in eyes with nAMD did not affect visual outcome. Further studies are necessary to better understand the exact association between ERMs and nAMD, and the effect of ERMs on anti-VEGF therapy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.