
Abstract

Neurodegenerative Diseases—Next-Generation Challenges
Since 1950, global average life expectancy has been steadily increasing at a rate of more than 3 years per decade (with the exception of the 1990s), 1 with accompanying growth in age-related neurodegenerative diseases, such as Alzheimer's (AD), Parkinson's (PD), amyotrophic lateral sclerosis (ALS), multiple sclerosis (MS), and stroke. The limited capacity of self-repair of the adult mammalian central nervous system (CNS) and the general lack of preventive and restorative treatments for these conditions lead to progressive debilitation and eventually death. Not only does this result in a diminished quality of life for patients (and their families) but also impacts society by placing tremendous demands on social welfare and health systems. How to “ensure healthy lives and promote well-being for all at all ages,” one of the Sustainable Development Goals for 2030, adopted by the United Nations General Assembly, is thus a challenge to be tackled by the next generation of researchers, clinicians, and policy makers.
Despite decades of intensive research, diagnosis and treatment remain challenging for neurodegenerative diseases. This treatment gap is believed to be the result of our still incomplete understanding of the complex interplay of pathological processes that underlie these conditions. In addition, many of them, most notoriously AD and PD, have a long prodromal phase, and by the time symptoms suggestive of a clinical diagnosis appear, neurodegeneration may have led to damage too extensive to repair. Early diagnosis during the asymptomatic stages of the disease could therefore open a therapeutic window, during which therapies that act to delay or prevent neurodegeneration can be effective.
Although modern brain imaging techniques (eg, magnetic resonance imaging, positron emission tomography, and single photon emission computed tomography) and blood/cerebrospinal fluid sampling have become most valuable tools in differentiating manifestations of healthy aging from pathological conditions, their high cost, necessity of using radioactive tracers, limited resolution, and/or invasiveness prevent their use for population-wide screening of preclinical signs and for longitudinal follow-up of patients.
Accumulating evidence now suggests that, rather than trying to access information about the disease state of the CNS in the brain, one could exploit the unique properties of the eye. In vivo assessments of retinal integrity and perfusion, electrophysiological function, and performance of vision-driven tasks have revealed signs of deterioration in many neurodegenerative diseases, notably AD, PD, ALS, and MS. Techniques such as optical coherence tomography, confocal scanning laser ophthalmoscopy, electroretinograms, and oximetry, which are becoming increasingly available at low cost, could therefore represent a novel means for identifying patients at risk that need further neurological examinations or for longitudinal follow-up of disease progression.
Common Disease Processes in the CNS—The Eye as a Research Tool
The renewed interest in the occurrence of retinal symptoms in subjects with neurodegenerative diseases seems to have finally launched the eye as a “window to the brain”, enabling diagnosis and monitoring of disease. We believe, however, that the eye has even more to offer. As an integral part of the CNS, the retina is strikingly similar to the brain and spinal cord with respect to its anatomy, functionality, response to insult, and immunology, and cellular and molecular mechanisms underlying neurodegeneration appear to be conserved. Indeed, many ocular diseases share characteristics typical of neurodegenerative disorders. This leads us to advocate the use of the eye as a model organ to study common disease mechanisms, including the following: vascular abnormalities, inflammation, mitochondrial dysfunction, aggregation of misfolded proteins, blood–brain/retina barrier disruption, and changes in fluid (aqueous humor/cerebrospinal fluid) dynamics (Fig. 1). 2
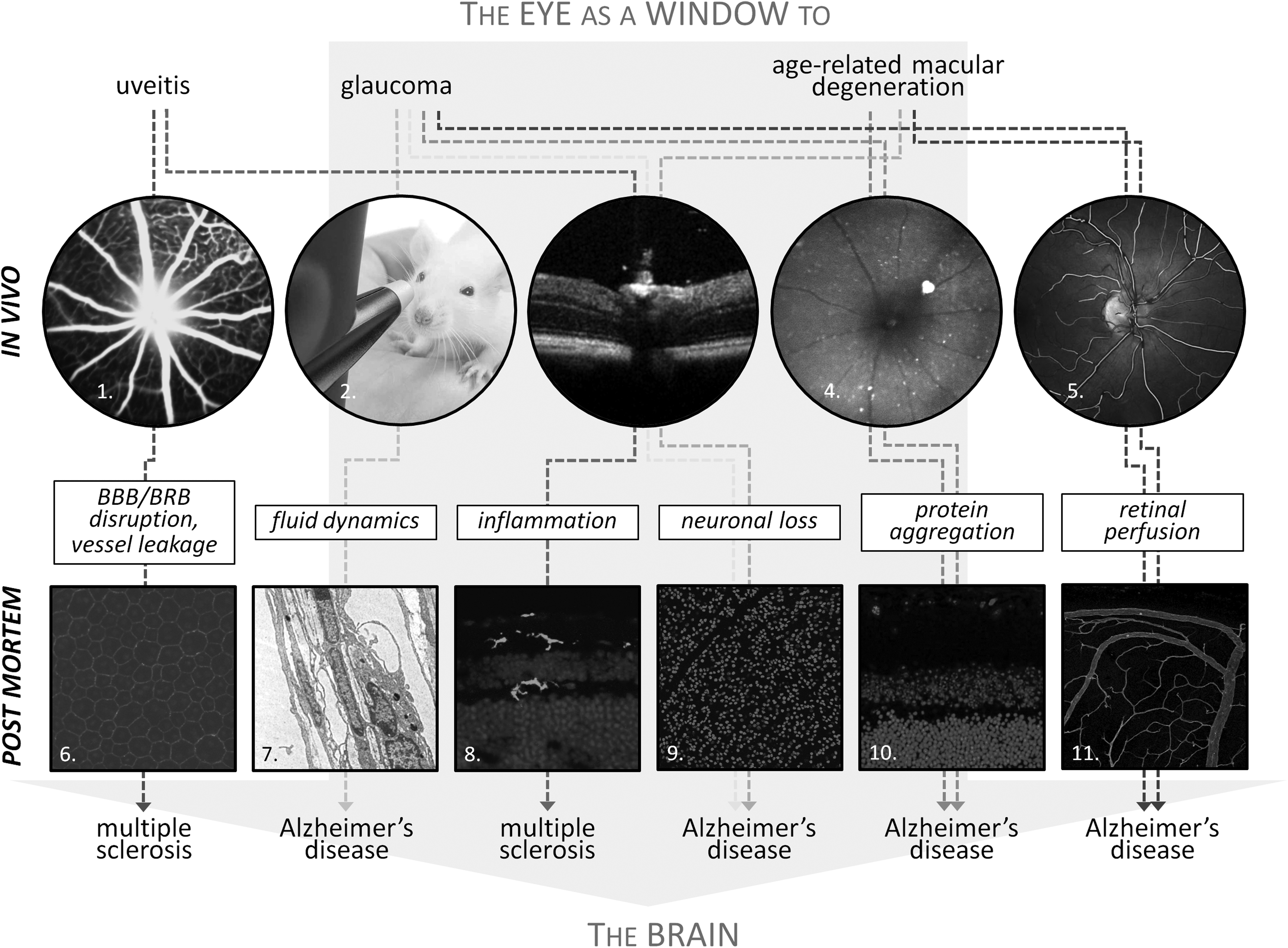
Compilation of examples to illustrate the concept “the eye as a window to the brain”. Typical ocular diseases, such as uveitis, glaucoma, and AMD, have in common several pathological mechanisms with CNS diseases, for example, MS and AD. Both in vivo and post mortem examinations of the eye can therefore be used to study the disease mechanisms underlying these pathologies in the eye ànd brain.
A first example to illustrate this concept comes from the striking similarities between AD, glaucoma, and age-related macular degeneration (AMD). All three are neurodegenerative diseases with age as the primary risk factor, although AD and glaucoma also have in common vascular dysregulation3–6 and decreased cerebrospinal fluid/aqueous humor turnover7,8—the latter leading to ocular hypertension, the sole modifiable risk factor and current therapeutic target for glaucoma—as potential elicitors of disease. Accumulating deposition of aggregated amyloid β and hyperphosphorylated Tau protein has been observed by histopathologic study in all three diseases, 9 and especially for AD and AMD, there are striking similarities in the protein composition of senile plaques and drusen, respectively.10,11 Furthermore, the deficits in axonal transport that have been proposed to result from Tau hyperphosphorylation are a common theme in the etiology of both AD and glaucoma.12,13 Also, the chronic neuroinflammatory response—characterized by activated microglia, complement activation, secretion of cytokines, and creation of oxidative and nitrosative stress, and elicited by amyloid β—is a recurrent theme in all three diseases.9,14–16 Strikingly, AD and AMD even share a genetic connection, with APOE alleles (apolipoprotein A) being associated with both.17,18
As a second example, we present Leber's hereditary optic neuropathy, the first human disease to be associated with mitochondrial DNA defects,19,20 which may provide a window on mitochondrial neurodegenerative diseases. The eye appears to be particularly vulnerable to mitochondrial disease, as optic nerve atrophy appears to be a common hallmark of multisystemic mitochondrial diseases.21,22 Retinal ganglion cells and their axons can therefore be used as model system to gain insight into mitochondrial network dynamics, fusion and fission, and mitophagy. Intriguingly, mitochondrial neurodegenerative diseases are associated with a characteristic pattern of retinal nerve fiber loss that predominantly affects the papillomacular bundle.22,23 Corroborating abnormal mitochondrial dynamics/distribution as a key feature of PD, this typical pattern of axonal loss is also seen in PD patients,20,21,23 but not in AD patients, in which the pattern of neurodegeneration more closely resembles that in glaucoma. 21 Indeed, Leber's hereditary optic neuropathy and PD are both associated with a complex I defect, leading to increased production of reactive oxygen species and subsequently neuronal apoptosis.23–25
These examples suggest that besides studying retinal changes in “classical” animal models of neurodegenerative disease (ie, models with an original focus on the brain), one could also make use of the vast array of well-characterized and validated models of ocular diseases to gain novel insights into the processes driving CNS disease. In the end, key pathophysiological processes such as angiogenesis, inflammation, or protein aggregation are driven by conserved mechanisms and molecules. Revisiting the examples described above, animal models for AMD can be used to explore disease mechanisms such as protein aggregation, immune system dysregulation, and oxidative stress, and thereby advance our understanding of both AMD and AD, 26 while extensive phenotyping of the retina/optic nerve in animal models of Leber's hereditary optic neuropathy could, for instance, unveil biomarkers of diseases that are also applicable to other diseases associated with mitochondrial dysfunction (eg, PD). 27
In addition, repurposing existing drugs or following common approaches for related retina/brain diseases seems a valuable strategy for developing new neuroprotective therapies, and a breakthrough in the retina may promote advances in the development of therapies for the brain and vice versa. In the case of AD/glaucoma/AMD, early successes with neuroprotective treatments for AD in the brain, for example, delivery of ciliary neurotrophic factor through a cell encapsulation approach, have added to the application of this therapy in the eye of AMD patients;9,28 and amyloid targeting therapies originally tested/developed in the AD brain have shown promising neuroprotective effects in animal models of ocular hypertension and drusen formation.29,30 Conversely, given the implication of complement activation in AD, the results from ongoing clinical trials with therapeutic approaches targeting the complement cascade in AMD could advance their use in AD as well.31–33 Other examples of common therapeutic strategies for both eye and CNS diseases, either under development or in clinical trials, include neurotrophin supplementation (eg, for AD, ALS, Huntington's disease, retinitis pigmentosa, and geographic atrophy),34–36 memantine (approved for AD, disappointingly failed for glaucoma), 37 and anti-tumor necrosis factor (TNF) therapeutics (eg, for AD, PD, stroke, glaucoma, and uveitis).38–41
However, why would one want to use the eye as a model organ? First, the availability of state-of-the-art technologies for ocular imaging, retinal electrophysiology, and behavioral testing of visual function generates an objective and quantifiable comprehensive dataset about a specific disease. Although at present this wealth of information cannot be gathered in any other part of the CNS, findings are likely to be translatable to the entire CNS. As these noninvasive techniques allow longitudinal and simultaneous follow-up of multiple processes in vivo, they substantially lower the number of animals used, which is cost saving, but also ethically important, and revolutionize the quantity and quality of experimental data. Second, the fact that identical readouts/equipment can be used for patients and laboratory animals confers high clinical relevance to these endpoint measures and unique possibilities in terms of translatability to the clinic. Finally, adding to its strength as a preclinical research tool, the eye is easily accessible and manipulable, in contrast to the brain and spinal cord that are both protected by bony structures. The anterior chamber and vitreous cavity can furthermore be considered local drug reservoirs, allowing administration of substances in small doses and with less systemic side effects. The latter is illustrated by the success of, for example, ciliary neurotrophic factor delivery through intraocular encapsulated cell technology implants in patients with retinitis pigmentosa and geographic atrophy, 42 intravitreal injections of steroids and anti-vascular endothelial growth factor (VEGF) therapeutics for a variety of indications (eg, AMD and diabetic retinopathy),43,44 gene therapy for Leber's hereditary optic neuropathy, Leber's congenital amaurosis, and Usher syndrome,45–47 and the ongoing development of cell transplantations to provide trophic support, repair, and replacement of retinal neurons. 48
Outlook
Although the idea of using the retina as a model organ to study the CNS as a whole or employing the eye as a means of assessing the pathophysiological state of the brain has increasingly gained momentum, it has only had a limited impact on neurodegenerative disease research. Implementation of the concept of “the eye as a window to the brain” may, however, lead to multiple applications providing unique opportunities for researchers, clinicians, and patients.
First, there is increasing research into brain and eye diseases, highlighting the use of in vivo retinal imaging as a tool for early diagnosis and follow-up of treatment/disease progression. Therefore, low-cost, noninvasive imaging of the retina could revolutionize clinical practice and open up a new time window for treatment. Furthermore, applying the same in vivo measures of disease progression (eg, optical coherence tomography, confocal scanning laser ophthalmoscopy, and electroretinograms) in preclinical and clinical disease, validates the use of clinically relevant endpoints, making the eye particularly attractive for preclinical development as well as fundamental research. In addition, evidence for common disease mechanisms in the retina and the brain continues to emerge, with animal models of ocular disease providing valuable research tools to gather new insights that can be translated to the CNS.49–51
Altogether, studies of retinal degenerative diseases have opened up new insights into the pathophysiology of, and potential therapies for, neurodegenerative diseases of the brain and spinal cord. Nevertheless, at the same time, many diseases are still waiting to be approached in this way. Motor neuron diseases, progressive supranuclear palsy, Leigh disease, and systemic lupus erythematosus, just to name a few, have been intensively studied with respect to the pathological manifestations in the brain, yet are nevertheless still poorly understood and untreatable. Studies of the eye, retina, and vision in these disorders would be “eye-opening” and may lead to breakthroughs in the management of these diseases.
Footnotes
Acknowledgment
Lies De Groef is a FWO (Fonds Wetenschappelijk Onderzoek, Research Foundation Flanders) postdoctoral fellow.
Author Disclosure Statement
No competing financial interests exist.