
Abstract
Abstract
Purpose:
To evaluate the real-world experience with half-time photodynamic therapy (PDT) versus half-dose PDT for chronic central serous chorioretinopathy (CSC).
Methods:
This multicenter retrospective study enrolled patients who received half-time PDT (with irradiation time shortened to 42 s) or half-dose PDT (with the dosage of verteporfin reduced to 3 mg/m2) for chronic CSC and who were followed up for ≧12 months. The success rate, central subfield retinal thickness (CST), and best-corrected visual acuity (BCVA) were documented in each group of patients.
Results:
A total of 53 eyes from 49 patients were enrolled in this study. Seventeen eyes (15 patients) received half-time PDT and 36 eyes (34 patients) received half-dose PDT. The success rates in both groups were similar at 12 months (94.1% vs. 94.4%; P = 0.543). The mean CST at 1, 6, 12 months decreased significantly when compared with the baseline in both groups (all P < 0.001). The BCVA significantly improved at 6 and 12 months in both groups (all P < 0.05). There were no significant differences in changes of BCVA and changes of CST between the 2 groups at any time point.
Conclusions:
Half-time PDT is a feasible treatment for chronic CSC. It has success rates similar to half-dose PDT at 12 months. There were no significant differences in changes of BCVA and changes of CST between the 2 groups at 1, 6, and 12 months after treatment.
Introduction
C
Although standard photodynamic therapy (PDT) with verteporfin can effectively resolve SRF in chronic CSC,2,3 complications such as RPE atrophy, secondary choroidal neovascularization (CNV), choriocapillaris ischemia, and subsequent visual loss have been reported.4,5 Different modifications to the PDT protocol, such as reducing the dosage of verteportin,6–11 laser fluence,5,12–17 or both parameters at the same time, 18 have been discussed for enhancing the safety and ameliorating the side effects compared with those of standard PDT. Both half-dose PDT and half-fluence PDT have been effective in improving best-corrected visual acuity (BCVA), decreasing central retinal thickness, and resolving SRF. 19 However, the optimal regimen remains unclear.
Half-fluence PDT was shown to significantly decrease hypoxic damage when compared with full-fluence PDT. 5 In a survey among members of the Macula Society, it is the most commonly used alternative PDT protocol (48%) for chronic CSC after full-fluence PDT (49%). 4 Practically, half-fluence PDT could be performed by reducing either the irradiance power (from 600 to 300 mW/cm2) or the laser exposure time (from 83 to 42 s).5,12–17 Reducing the laser exposure time, called half-time PDT, has a potential advantage in treating patients with frequent involuntary movements or requiring multiple laser spots (such as those with bilateral disease or multiple leakage areas) by shortening the laser time for each spot.14,15,17
However, there have been very few studies reporting the efficacy of half-time PDT.14–17 These studies were limited by either the heterogeneity of subjects (enrolling both acute and chronic CSC in the same study)15,17 or short follow-up duration (between 3 and 6 months).14,16 A majority of the recurrent CSC occurred later than 6 months after PDT6,15; hence, long-term follow-up data are important for comparing the success rates of each protocol. The purpose of this study is to evaluate the real-world experience with safety and efficacy of half-time PDT at 1 year, and compare half-time PDT with half-dose PDT for treating chronic CSC.
Methods
This retrospective study reviewed the medical records and images of patients who received half-time PDT or half-dose PDT for chronic CSC between June 2011 and May 2014 at Keelung Chang Gung Memorial Hospital, Linkou Chang Gung Memorial Hospital, and Mackay Memorial Hospital. This study was approved by the Institutional Review Boards of Chang Gung Memorial Hospital and Mackay Memorial Hospital, respectively. The study followed the tenets of the Declaration of Helsinki.
Chronic CSC was defined as CSC with persistent visual symptom disturbance for 6 months or more, or the presence of any sign of long-standing SRF accumulation, such as RPE atrophy, descending atrophic tracts, or subretinal precipitates. The exclusion criteria were (1) absence of SRF on the baseline optical coherence tomography (OCT), (2) PDT performed with a protocol different from that of this study, (3) previous treatment with laser focal photocoagulation, intravitreal injection of antivascular endothelial growth factor drugs (anti-VEGF), or PDT within 6 months before enrollment, (4) presence of any evidence of CNV or polypoidal choroidal vasculopathy (PCV) at baseline, (5) current treatment with steroids for any other diseases, and (6) a follow-up period of <12 months after PDT treatment.
All patients received complete ocular examinations, BCVA, OCT [(Stratus OCT Model 3000; Carl Zeiss Meditec, Inc., Dublin, CA), or (RTVue-100; Optovue, Inc., Fremont, CA)], and simultaneous fluorescein angiography (FA) and indocyanine green angiography (ICGA) (Heidelberg Retina Angiography; Heidelberg Engineering, Heidelberg, Germany) at baseline. Spectral-domain OCT values were converted into time-domain-equivalent values for analysis as suggested in previous studies.20,21 Informed consent for PDT was obtained from all patients.
The PDT procedures are briefly described as follows. First, verteporfin (Visudyne; Novartis Ophthalmics, Basel, Switzerland) was infused for 10 min, followed by PDT application 5 min later. The laser was 689 nm with a standard light intensity of 600 mW/cm2. In the half-time PDT group, the standard dosage of verteporfin (6 mg/m2) was used and the irradiation time was shortened to 42 s. In the half-dose group, the dosage of verteporfin was reduced to half (3 mg/m2) and the standard irradiation time of 83 s was used. All PDT procedures were performed under ICGA guidance. The treatment spot size was the smallest circular area covering choroidal hyperpermeability and dilated vessels in ICGA, which was related to active FA leakage. In patients with >1 leakage area, the primary leakage area corresponding to the posterior pole SRF was treated first, followed by other leakage areas.
After PDT, patients were followed up at 1, 6, and 12 months. Both BCVA and OCT were obtained at every visit if possible. The presence or absence of SRF was documented. FA and ICGA may be repeated if recurrence was noted.
The primary endpoint was 12 months after PDT. The primary outcome measured the success rate in each group of patients. This study defined treatment success as complete resolution of SRF after PDT and no recurrence of SRF during follow-up. Treatment failure was defined as incomplete resolution of SRF after PDT or recurrence of SRF during follow-up. The timing of recurrence and post-treatment complications were recorded. The success rates of both groups were compared by the Fisher's exact test.
The secondary outcomes measured the changes in BCVA and changes in central subfield retinal thickness (CST) at 1, 6, and 12 months. BCVA was measured on the Snellen chart and converted to the logarithm of the minimum angle of resolution (logMAR) for calculation. The paired samples t-test was used to analyze the changes in BCVA and CST at 1, 6, and 12 months in comparison to baseline values in each group. Intergroup comparison was performed using independent samples t-test. We also compared the proportion of patients with BCVA loss ≧3 lines, stable (change <3 lines), and gain ≧3 lines between groups by the chi-square test.
A linear regression model was used to evaluate the factors related to BCVA at 12 months. A Cox regression model was utilized to determine the risk factors related to recurrence during follow-up. All data were analyzed using SPSS Program Package Version 17.0 (SPSS, Inc., Chicago, IL). A 2-tailed P value of <0.05 denotes statistical significance.
Results
There were 53 eyes from 49 patients enrolled in this study. Seventeen eyes (15 patients) received half-time PDT and 36 eyes (34 patients) received half-dose PDT. Table 1 shows the demographic data and clinical characteristics of patients in both groups. There were no significant differences in age, gender, duration of disease, baseline BCVA, baseline CST, PDT spot size, or follow-up duration between the 2 groups. All patients were followed up for 12 months or more. The mean follow-up times were 23.7 months in the half-time PDT group and 22 months in the half-dose PDT group (P = 0.936).
Consists of 15 patients in half-time PDT group and 34 patients in half-dose PDT group.
P values were calculated by independent samples t-test.
P values were calculated by Fisher's exact test.
BCVA, best-corrected visual acuity expressed in the logarithm of the minimal angle of resolution (logMAR); CST, central subfield retinal thickness; PDT, photodynamic therapy; SD, standard deviation.
Success rate
Table 2 compares the treatment outcomes between the half-time PDT and half-dose PDT groups. There was no difference between the 2 groups in success rates at any time point. At 1 month after PDT, all patients had decreased SRF. However, 1/17 eyes (5.9%) in the half-time PDT group and 10/36 eyes (27.8%) in the half-dose group had shallow residue SRF. Although there was a trend that the half-time group had faster complete resolution of SRF at 1 month, the difference was statistically insignificant (Fisher's exact test; P = 0.082). All eyes had complete resolution of SRF by 6 months after treatment.
P values were calculated by Fisher's exact test.
P values were calculated by independent samples t-test.
BCVA, best-corrected visual acuity; CST, central subfield retinal thickness; logMAR, logarithm of the minimal angle of resolution; PDT, photodynamic therapy; SD, standard deviation.
In the half-time PDT group, recurrent SRF was noted in 2 eyes at 9 and 13 months, respectively. In the half-dose PDT group, recurrent SRF was also found in 2 eyes at 11 and 13 months, respectively. Another 2 eyes in the half-dose group had recurrent macular edema due to secondary CNV and PCV at 19 and 35 months, respectively. Therefore, the 12-month success rates were 94.1% in the half-time PDT group and 94.4% in the half-dose PDT group. There were no differences in the success rate between the 2 groups at any time point (Table 2).
Visual acuity
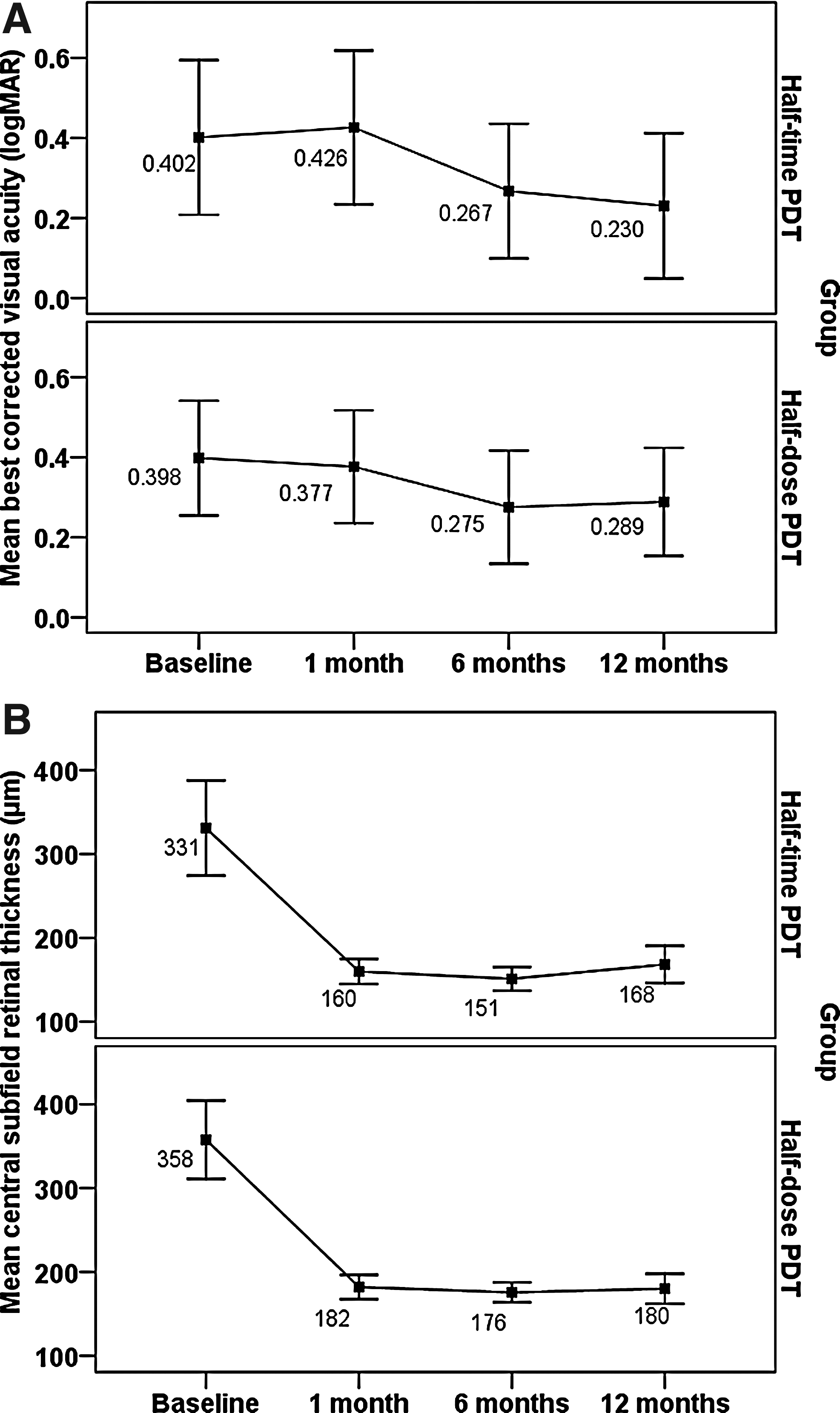
The mean BCVA (logMAR) at different time points is shown in Fig. 1A. At 1 month after treatment, the BCVA deteriorated slightly from 0.402 to 0.426 (P = 0.565) in the half-time PDT group and improved slightly from 0.398 to 0.377 (P = 0.655) in the half-dose PDT group. Both changes were statistically insignificant. Then, the BCVA improved significantly to 0.267 (P = 0.041) at 6 months and 0.230 (P = 0.009) at 12 months in the half-time PDT group. It also improved significantly to 0.275 (P = 0.010) at 6 months and 0.289 (P = 0.026) at 12 months in the half-dose PDT group. However, the intergroup comparison showed no significant differences in mean change of BCVA between the 2 groups at any time point (Table 2).
The distribution of best-corrected visual acuity
There was also no significant difference in the proportion of patients with their BCVA loss ≧3 lines, stable (change <3 lines), and gain ≧3 lines between the 2 groups (Fig. 2). In the linear regression model, better baseline BCVA and thicker baseline CST were associated with better BCVA at 12 months (Table 3). Gender, age, spot size, and different PDT protocols (half-time vs. half-dose) were not associated with the BCVA at 12 months.

The proportion of patients with best-corrected visual acuity loss ≧3 lines, stable (change <3 lines), and gain ≧3 lines in the 2 groups at 1, 6, and 12 months. P values were calculated by chi-square test. PDT, photodynamic therapy.
BCVA, best-corrected visual acuity expressed in the logarithm of the minimal angle of resolution (logMAR); CST, central subfield retinal thickness; PDT, photodynamic therapy.
Central subfield retinal thickness
The mean CST at different time points is shown in Fig. 1B. The mean CST rapidly improved at 1 month after PDT and remained stable thereafter in both groups. The improvement was statistically significant at 1, 6, and 12 months in both groups (all P < 0.001). Intergroup comparison showed no significant differences in mean changes of CST between the 2 groups at any time point (Table 2).
Recurrence
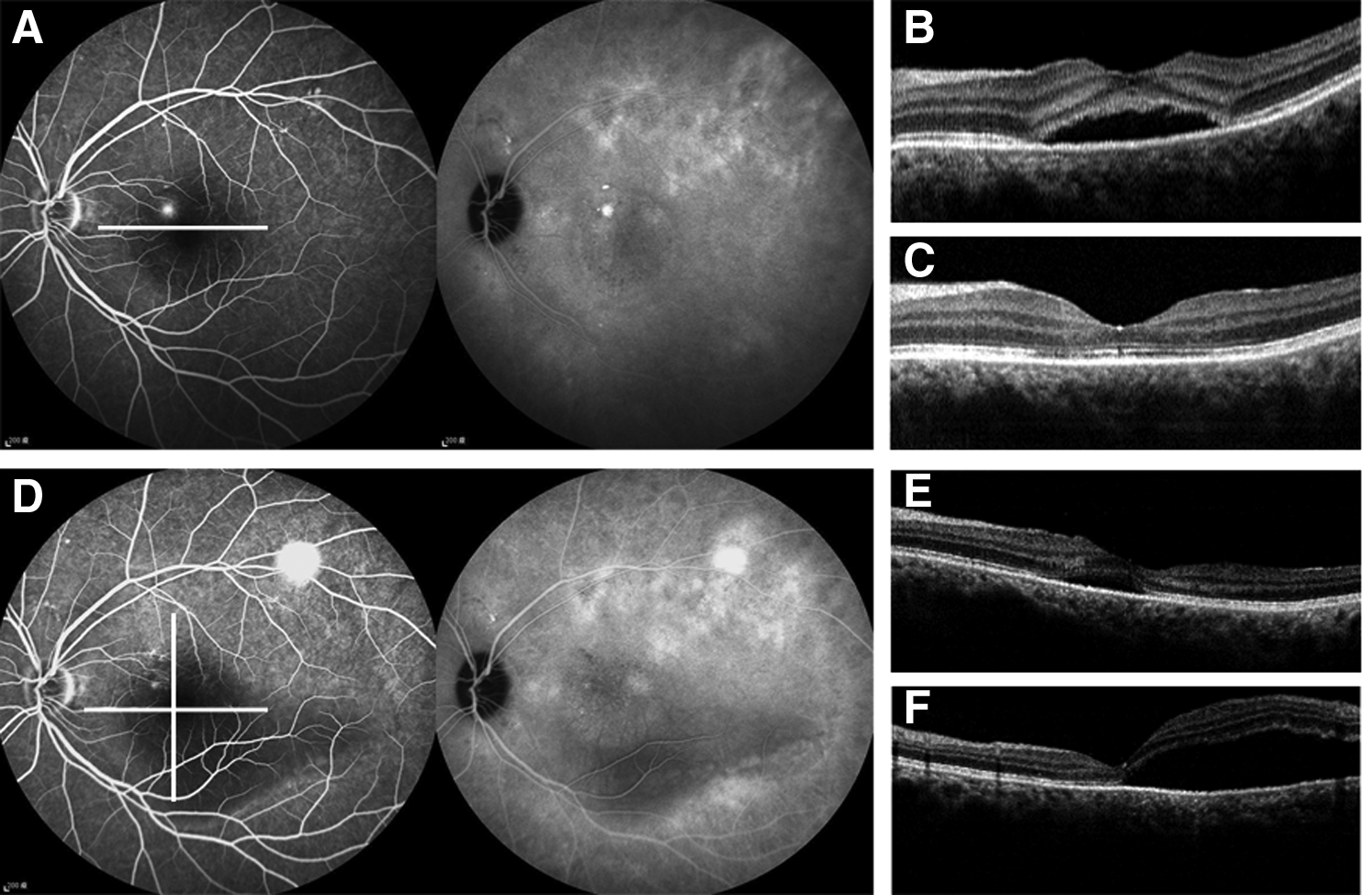
In the half-time PDT group, 1 eye had the recurrence at a location different from the previous PDT-treated area at 9 months (Fig. 3). The new leakage was extrafoveal and could be successfully treated by focal retinal photocoagulation. Another eye had 2 episodes of recurrence. The first recurrence at 13 months was at a different location. The second recurrence occurred at 17 months and had 2 leakage areas; 1 at the previous PDT-treated area and 1 at a different location. All recurrences were successfully treated by focal retinal photocoagulation. In the half-dose PDT group, all recurrences were noted at the same locations previously treated with PDT. The Cox regression model showed no association between any of the factors under evaluation (gender, age, baseline BCAV, baseline CST, spot size, PDT protocol) and recurrence during follow-up (all P > 0.1) (Table 4).
BCVA, best-corrected visual acuity expressed in the logarithm of the minimal angle of resolution (logMAR); CST, central subfield retinal thickness; PDT, photodynamic therapy.
Other complications
There were no immediate PDT-related complications such as RPE rip, retinal hemorrhage, or severe visual loss in the 2 groups. However, in the half-dose PDT group, one eye developed secondary CNV at 19 months and another eye developed secondary PCV at 35 months after PDT. Both patients were successfully treated with combined half-dose PDT and anti-VEGF.
Discussion
This study compared the efficacy of half-time PDT and half-dose PDT in the treatment of chronic CSC. Both treatment protocols had a similar high success rate at 12 months (94.1% vs. 94.4%; P = 0.543). The mean CST significantly decreased at 1 month in both groups and remained stable thereafter (Fig. 1B). There were no significant differences in changes of CST and changes of BCVA between the 2 groups at any time point.
There has been limited reported data on the half-time PDT for chronic CSC.15–17 Tsai and Hsieh reported FA-guided half-time PDT in 16 eyes with either acute CSC or chronic CSC. 17 All eyes had SRF completely resolved within 5 weeks and the mean logMAR BCVA significantly improved at 3 months. In another retrospective case series, Liu et al. compared half-dose and half-time FA-guided PDT for eyes with either acute CSC or chronic CSC. 15 They concluded that half-dose and half-time FA-guided PDT showed similar efficacy in visual improvement and SRF resolution. However, chronic CSC has different clinical courses and visual outcomes from acute CSC. 1 It may be more precise to study them separately.
Shiode et al. reported 3-month outcomes in half-dose versus half-time ICGA-guided PDT for chronic CSC (27 eyes received half-dose PDT and 18 eyes half-time PDT). 16 SRF completely resolved in 88.8% of eyes at 3 months in both groups. There was no difference in final BCVA. However, the long-term outcome was not reported.
A prospective randomized study conducted by Cheng et al. found that 20/20 (100%) patients in the half-dose PDT group and 19/20 (95%) patients in the half-time PDT group had complete absorption of subretinal fluid at 3 and 6 months. 14 There were no significant differences in BCVA and central retinal thickness between the 2 groups at baseline or at each follow-up time point within 6 months. 14 However, a majority of the recurrent CSC occurred later than 6 months after PDT6,15; hence, comparing the long-term outcome of these 2 PDT protocols is important but the data are still not available.
In this study, all patients were followed up for 12 months or more. Present findings indicate no difference in success rate, changes of BCVA, or changes of CST between half-dose PDT and half-time PDT at 12 months. The 2 PDT protocols also showed no difference in the proportion of patients with their BCVA loss ≧3 lines, stable (change <3 lines), and gain ≧3 lines (Fig. 2). Both treatment protocols are showed to be equally effective and safe for chronic CSC at 12 months.
When comparing the current results with previous studies, we can reveal several interesting trends. First, this study and that of Liu et al. observed a trend of faster resolution of SRF in the half-time PDT group, although the differences were not statistically significant. In this study, complete resolution of SRF was found in 16/17 eyes (94.1%) in the half-time PDT group and in 26/36 eyes (72.2%) in the half-dose group at 1 month (P = 0.082) (Table 2). Similar findings were obtained by Liu et al.; the proportion of complete SRF resolution within 1 month was 81% in the half-time group and 60% in the half-dose group (P = 0.10).
Second, VA improvement seems slightly slower in the half-time PDT group (Fig. 1A). The mean BCVA dropped slightly at the 1 month and then regained at 6 and 12 months in the half-time PDT group. On the contrary, the mean BCVA improved gradually at 1, 6, and 12 months in the half-dose PDT group. A similar trend could also be observed in the study from Shiode et al. and Liu et al.15,16 However, none of those studies was able to show a statistical difference in BCVA at 1 month between the 2 PDT protocols.
Third, recurrent SRF seemed more likely to come from new leaking points in the half-time PDT group but from the same leaking points in the half-dose PDT. In this study, a total of 3 recurrent SRF episodes occurred in the half-time PDT group. Only 1 of the 2 leakage areas in 1 episode involved the previous PDT-treated area. The others were all de novo leakage locations. On the contrary, leakages from previous PDT-treated area were found in the 2 eyes with SRF recurrence in the half-dose PDT group. Similar findings were reported by Liu et al. 15 Two eyes in the half-time PDT group had recurrent SRF and both of them had new leakage points in FA. However, all 3 eyes with recurrent SRF in the half-dose group had leakage points at the previous PDT-treated location.
Adding all these findings together, we speculate that half-time PDT might have a slightly larger PDT effect than half-dose PDT, thus leading to faster SRF resolution, little drop in BCVA at 1 month, and less recurrence at the original treated region. However, the difference might be sufficiently small that the current study was not powerful enough to show a statistical significance. There were also no differences in changes of BCVA and CST at long-term follow-up.
In the linear regression model, better baseline BCVA was associated with better BCVA at 12 months. This result is compatible with previous findings. 15 Larger baseline CST, that is, thicker subretinal fluid was found to be associated with better visual outcome. This is probably because some patients with very long-duration chronic CSC were characterized by persistent shallow SRF. Usually, these patients had worse visual outcomes due to diffuse RPE atrophy and severe photoreceptor damage.
This study enrolled patients with chronic CSC for 6 months or more; and the damage to the photoreceptor-RPE complex could be demonstrated by poor baseline BCVA (around 20/50) in both groups (Table 1). The chronicity of diseases also contributes to less obvious improvement in BCVA after treatment. 1 So, a majority (71%–75%) of our patients showed stable vision (change <3 lines) after treatment and only 22%–29% of patients had gained ≧3 lines in the long-term follow-up (Fig. 2).
There are several potential benefits for half-time PDT in selected cases. It is suggested that patients with old age, involuntary movements, or eye squeeze may be benefited by shortening the laser application time.17,18
In addition, it may also potentially benefit patients with multiple leakage areas or bilateral eye diseases, which are not uncommon in chronic CSC. Tseng and Chen performed half-dose PDT for 56 eyes with chronic CSC. 6 Four of the 17 (23.5%) eyes with multifocal leakage areas developed recurrent SRF; while none of the eyes with monofocal leakage area had recurrence. All the recurrent lesions were found at the second or third spot of previous PDT-treated area. They suspected that the recurrence was caused by low verteporfin concentration and suboptimal PDT effect during the second or third laser application. Thus, half-time PDT may benefit these patients by halving the laser application time at each spot.
Finally, half-time PDT does not require any modification in the reconstitution of verteporfin (necessary for half-dose PDT) or any adjustment in laser machine setting (necessary for half-fluence PDT with reducing the irradiance power). Hence, it will make it easier for assisting nurses or technicians to execute the doctor's commands, and less likely to cause unexpected errors during the preparation process.
There were no immediate PDT-related complications in the 2 groups. However, secondary CNV at 19 months and secondary PCV at 35 months were found after half-dose PDT. Secondary CNV and PCV were not uncommon in patients with chronic CSC.22–24 Therefore, it is difficult to determine whether the delayed CNV and PCV in this study were related to the natural course of chronic CSC or to the delayed complications of PDT. Moreover, since the development occurred long after our study ended, it is difficult to evaluate its incidence rate within each group. We provide these data as additional information to remind ophthalmologists that long-term follow-up in patients with chronic CSC is recommended.
There were some limitations in this study. First, it was limited by its small sample size. This is because CSC is a relatively benign disease and patients had low motivation for long-term follow-up once SRF was resolved. Second, it was a retrospective study. Nevertheless, this study depicts valuable real-world 12-month success rate and clinical course of 2 different PDT protocols for chronic CSC. It warrants further prospective randomized control trials to confirm these outcomes.
Third, time-domain OCT was used on some patients. There were 24 (11 in half-time PDT group and 13 in half-dose PDT group) eyes initially evaluated by time-domain OCT and 13 (5 in half-time PDT group and 8 in half-dose PDT group) of them later switched to spectral-domain OCT. It is not impossible that very subtle subretinal fluid could be missed on time-domain OCT. However, the subtle (“time-domain OCT undetectable”) subretinal fluid missed might not be clinically significant and may not require retreatment.
In conclusion, half-time PDT is feasible for treating chronic CSC. It has a success rate similar with half-dose PDT at 12 months. In both PDT protocols, the mean CST significantly decreased at 1 month and remained stable thereafter. There were no significant differences in changes of BCVA and changes of CST between the 2 groups at 1, 6, and 12 months after treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.