
Abstract
Abstract
Purpose:
Topical corticosteroids are widely used in the treatment of inflammation and pain after ocular surgery, but they possess several shortcomings, including frequent dosing and low patient adherence. We evaluated the efficacy and pharmacokinetics of ENV905 (difluprednate or DFBA) Ophthalmic Implant, a single-dose drug delivery system, compared with 0.05% Durezol.
Methods:
PRINT® technology was used to fabricate ENV905 implants for either intracameral (IC) or subconjunctival (SCJ) delivery of extended-release DFBA. A postoperative inflammation model and ocular pharmacokinetics studies of ENV905 or Durezol were conducted in albino rabbits for a maximum of 12 weeks.
Results:
Suppression of ocular inflammation was marked for both IC and SJC ENV905 compared with placebo, and it was superior or equivalent to that observed with QID Durezol. Concentrations of desacetyl difluprednate (DFB, active metabolite) peaked on day 1 and tapered over time for ENV905, with IC ENV905 delivering DFB to the target tissue at the time of greatest inflammation, whereas SJC produced a longer duration of exposure. Durezol eyes demonstrated consistent exposure over time with maximal exposure in the cornea. Although the pharmacokinetic profile differed for the two routes, efficacy was similar.
Conclusion:
ENV905 was well tolerated and demonstrated a robust reduction in ocular inflammation with targeted drug delivery. The results from these studies show that ENV905 provides a sustained therapeutic effect after a single dose. By resolving low patient compliance and eliminating the peaks and troughs in drug concentration, sustained drug delivery via ENV905 may further improve the overall control of postoperative inflammation and pain.
Introduction
C
Efficacy of topical corticosteroids currently available for postoperative inflammation and pain is dependent on ocular tissue distribution, as well as on patient compliance. After topical application of eye drops, more than 80% of the product is eliminated via the nasolacrimal drainage, thus limiting delivery to the target ocular tissues and increasing systemic exposure. 3 The majority of patients who are candidates for cataract surgery are of advanced age, which is often associated with compliance problems, particularly for topical steroids that require multiple-times-per-day dosing.3–6
As an alternative to topical therapies, an injectable corticosteroid ophthalmic implant administered once at the time of cataract surgery would likely provide improvement over topical therapies in the areas of patient convenience, compliance, and potentially overall control of postoperative inflammation and pain. In addition, targeted administration may decrease the total amount of corticosteroid required to suppress inflammation, resulting in a dose-sparing effect, decreased systemic exposure, and potentially decreased incidence of ocular adverse effects such as increased intraocular pressure (IOP) due to elimination of peaks and troughs in drug concentration.
Difluprednate (DFBA) is a synthetic difluorinated prednisolone derivative that was originally developed as an anti-inflammatory for dermatologic conditions, and it is administered as a prodrug that is quickly metabolized to the active metabolite, desacetyl difluprednate (DFB). DFBA has been formulated for topical ocular administration as an emulsion (0.05% Durezol), and studies have shown that metabolism occurs rapidly in ocular tissues. 7 In animal studies, 0.05% DFBA emulsion was shown to be effective in a rabbit model of postoperative inflammation (Kida, et al. Association for Research in Vision and Ophthalmology. Invest Ophthalmol Vis Sci, 2007; 48:E-Abstract 2655), and it was distributed within the eye and cleared rapidly.8,9 DFBA ocular topical emulsion is currently approved and marketed for the treatment of pain and inflammation associated with ocular surgery under the tradename Durezol® (Alcon Laboratories, Fort Worth, TX).
ENV905 (DFBA) Ophthalmic Implant is an injectable biodegradable DFBA implant formulation using a biocompatible polyethylene glycol (PEG)-based drug delivery system. The implant is designed for ophthalmic administration via subconjunctival (SCJ) or intracameral (IC) injection, with a single dose administered after ocular surgery targeting the duration of action of 4 weeks. ENV905 was designed to provide a treatment alternative to corticosteroid topical drops, eliminating compliance issues associated with eye drops, while providing targeted drug delivery to the structures in the eye most affected by surgical trauma. In these studies, we investigated in animal models the efficacy, ocular and systemic pharmacokinetics, and tolerability of ENV905 compared with the marketed product, Durezol.
Methods
ENV905 implant formulation development and manufacturing
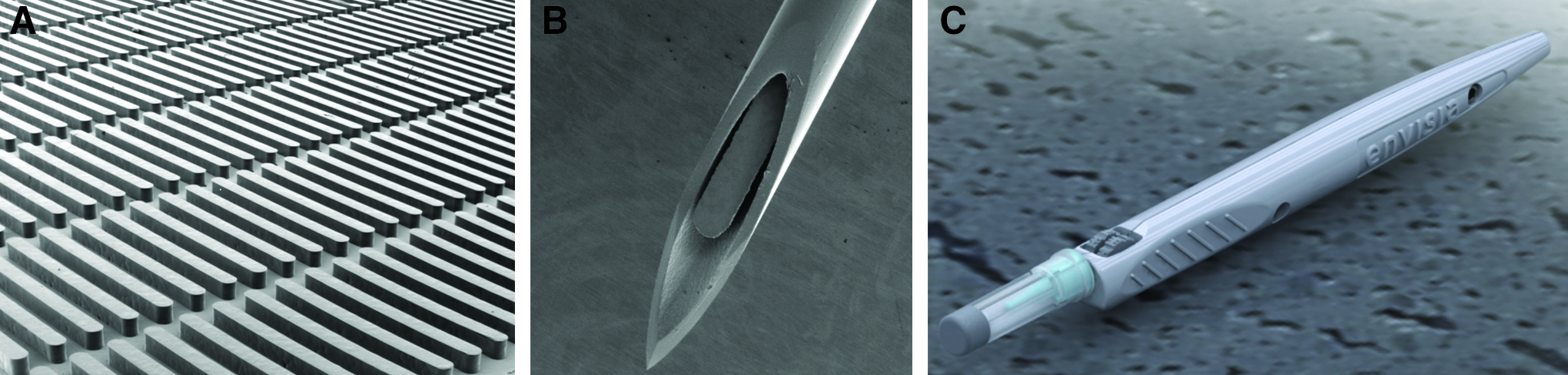
ENV905 (DFBA) Ophthalmic Implants were prepared by using the PRINT® technology, which has the ability to impart precise control over shape, size, and dose of solid dosage formulations. Briefly, micronized DFBA (Farmabios Spa, Italy) was compounded with PEG of two different molecular weights: 100,000 Da (PolySciences, Inc., USA) and 3,350 Da (Spectrum Chemical, USA). The blend was then heated to 130°C to allow for the PEGs to melt and to create a homogenous solid dispersion with the micronized DFBA on cooling back to room temperature. Flexible, mold templates, consisting of an array of cavities of uniform size and shape, were fabricated (Envisia Therapeutics).
Using these mold templates, the ENV905 (DFBA) Ophthalmic Implants were then formed by thermally molding the DFBA/PEGs blend into the cavities. The formed implants were then removed from cavities and packaged for terminal sterilization via gamma irradiation with a dose of 46 kGy (Steris Isomedix). The water-soluble PEGs function as both a diluent and a binder for the micronized DFBA to form an injectable, solid implant formulation (Fig. 1). ENV905 was designed for rapid dissolution of the implant and concurrent release of DFBA after administration, with the IC ENV905 implant containing ∼40 μg of DFBA, whereas the larger SCJ ENV905 implant contained ∼400 μg DFBA. The bioavailability and sustained therapeutic effect of ENV905 over 4 weeks is governed by multiple factors, including route of administration and the physicochemical properties of the drug substance DFBA.
Animals
New Zealand White rabbits were obtained from Covance Research Products (Denver, PA), identified by ear markings, and were singly housed and maintained under controlled conditions. The animals were given access to tap water ad libitum and were fed a daily ration of standard laboratory rabbit diet. Lighting was maintained at 12 h light and 12 h dark. All animal studies were approved and monitored by the Institutional Animal Care and Use Committee at Powered Research and conducted according to standard protocols and the guidelines of the Association for Research in Vision and Ophthalmology for the Use of Animals in Ophthalmic and Vision Research.
Postoperative inflammation model
New Zealand White rabbits (2–4 females per group) were administered a single bilateral IC (1 implant, 40 μg DFBA per eye) (Fig. 2) or SCJ (1 implant, 393 μg DFBA per eye) injection of ENV905 implant(s), placebo implant(s), or daily topical Durezol administered QID (2,400 μg DFBA per eye), and they were followed for 24 days (Table 1).

ENV905 intracameral implant being administered into the anterior chamber of the New Zealand White rabbit.
BID, twice daily; DFBA, difluprednate; NA, not applicable; QD, four times daily; QID, once daily.
IC injections were performed on day 1 by using a custom implant applicator and a 27G needle, which were inserted through the clear cornea near the limbus at the 12 O'clock position, delivering the implant into the anterior chamber where it proceeded to settle into the iridocorneal angle while commencing to erode. For SCJ delivery on day 1, a 1 to 2 mm conjunctival incision was made 2 mm posterior to the limbus with Stevens tenotomy scissors at the site intended for implant placement (superior temporal). A small SCJ tunnel was made parallel to the limbus with the scissors. A custom implant applicator with a 21G needle was inserted through the conjunctival incision into the SCJ pocket, and the implant was deposited subconjunctivally by depressing the syringe plunger while at the same time slowly retracting the needle from the pocket; surgical closure was not required. Negative control groups received a placebo implant either intracamerally or subconjunctivally, which contained the same polymers as the active implants, and they were also the same size and shape as the actives.
Each animal received a bilateral surgical 2.75 mm clear corneal incision on day 1 that was designed to mimic the incision during cataract surgery, followed by anterior chamber paracentesis using a 30G needle on days 9, 15, and 22; each of these procedures was designed to induce ocular inflammation. The eyes were examined at baseline and on days 2, 3, 4, 9, 10, 11, 15, 16, 17, 22, 23, and 24 by a board-certified veterinary ophthalmologist, and ocular inflammation was scored by using the Hackett-McDonald grading scale.
A two-tailed unpaired Student's t-test was performed by utilizing GraphPad Prism Software specifically for pairwise comparisons between the ophthalmic exam data for ENV905 and the respective control groups (placebo or Durezol) at each time point. Significant differences were determined (P < 0.05) and reported.
Ocular pharmacokinetics studies
Two ocular and systemic pharmacokinetic studies were conducted. Study 1 included IC ENV905 and Durezol with animals followed for a maximum of 42 days, whereas Study 2 included SCJ ENV905 with animals followed for a maximum of 84 days. New Zealand White rabbits (two males per group per terminal time point) were administered a single bilateral administration of ENV905 (DFBA) Ophthalmic Implants, either via IC (1 implant, 42.8 μg DFBA per eye) or SCJ (3 implants, 1207.5 μg DFBA per eye) delivery. ENV905 dose administration was conducted as described for the postoperative inflammation model. A separate group of animals received topical bilateral 0.05% Durezol according to the clinical standard-of-care paradigm for comparison purposes. Durezol dose administration was conducted as follows: QID on days 1–14, BID on days 15–21, and QD on days 22–28, resulting in a total dose of up to 1,925 μg DFBA per eye over the course of the study. Animals were followed for a maximum of 42 or 84 days, with regular clinical observations and external ocular assessments, and plasma and ocular matrices were collected to determine systemic and ocular pharmacokinetics (Table 1).
Plasma and ocular matrices were collected on day 1 (2 h postdose), day 2 (24 h postdose), days 4, 7, 14, 21, 28, and 42 (Study 1, IC ENV905 and Durezol), or days 14, 28, 42, 56, and 84 (Study 2, SCJ ENV905). Samples for animals in the Durezol group were collected at 30 min after the last dose administration on each designated collection day, so as to capture the peak exposure after topical administration. Aqueous humor was collected before enucleation and snap frozen; the globes were then enucleated and frozen in liquid nitrogen. Globes were dissected to obtain remaining aqueous humor, bulbar conjunctiva, cornea, trabecular meshwork, iris/ciliary body, and retina. During dissection, tissue was kept frozen by dissecting the globe over a dry ice and ethanol mixture; however, at times, sections of the eye were allowed to partially thaw to obtain certain tissues.
DFB (desacetyl difluprednate) and its internal standard DFB-d6 were extracted from 200 μL aliquot of rabbit (K2EDTA) plasma by liquid–liquid extraction with methyl-t-butyl ether (MTBE) after dilution with 0.5 M potassium phosphate buffer, pH7 buffer. After evaporation to dryness and reconstitution, the extracts were analyzed by liquid chromatography and tandem mass spectrometry (LC-MS/MS). Run times for the reversed-phase chromatography separation and Turbo IonSpray analysis were ∼5 min. The Lower Limit of Quantitation (LLOQ) was 0.0500 ng/mL and the calibration curve range was 0.0500–50 ng/mL for DFB.
DFBA and DFB and their internal standards DFB-d6 and BDP (Beclomethasone Dipropionate) were extracted from rabbit ocular tissue (conjunctiva, cornea, iris/ciliary body, and retina) by bead homogenization in 20:80 acetonitrile: 50 mM ammonium acetate, pH 3.5 buffer and protein precipitation extraction by using acetonitrile. An aliquot of the supernatant was diluted with 0.5 M potassium phosphate buffer, pH7 buffer and extracted further by liquid–liquid extraction with MTBE. After evaporation to dryness and reconstitution, the extracts were analyzed by LC-MS/MS. Run times for the reversed-phase chromatography separation and atmospheric pressure chemical ionization analysis were ∼5 min. The LLOQ was 0.0200 ng for DFBA and DFB. The calibration curve range was 0.0200–50 ng for DFBA and DFB. To reduce the use of rabbit ocular control tissues and to allow for samples from multiple tissue types to be assayed together in a single run, rabbit plasma with 1 mM phenylmethylsulfonyl fluoride/1% HOAc was used as a surrogate matrix for the preparation of calibration curve and analytical quality control samples (QCs). To represent tissue study samples, an additional set of QC samples were prepared directly in each rabbit ocular tissue (process QC samples).
Pharmacokinetic parameter estimates were derived by using WinNonlin software. A noncompartmental approach consistent with the route of administration was used for parameter estimation (i.e., extravascular input). Parameters included Cmax, Tmax, Clast, Tlast, T1/2, AUCall, AUClast, and MRTlast. When data permitted (R2 value ≥0.60), the slope of the terminal elimination phase was used to calculate half-life.
Results
Postoperative inflammation model
No test article-related adverse effects on body weight, food consumption, or daily clinical observations were noted in any group, and the animals remained in good health throughout the study.
Ocular inflammation was successfully induced after corneal incision on day 1 and after anterior chamber paracenteses on days 9, 15, and 22, as indicated by the assessment of inflammation in the placebo group. The inflammatory response after corneal incision was increased compared with the inflammation after the paracentesis, which was expected given the differing size of the lesions. Signs of inflammation observed during ophthalmic exams included conjunctival congestion and chemosis, aqueous cells and flare, altered pupillary light reflex, and iris hyperemia.
Durezol dampened the inflammation observed on day 2 (1 day postinitial Durezol dosing) induced by the corneal incision on day 1, but it was minimally effective after the paracenteses. One day postinitial Durezol dosing and corneal incision, the Durezol group showed signs of mild-to-moderate conjunctival congestion and mild chemosis. Other findings included mild aqueous cells and flare, altered pupillary light reflex, and mild-to-moderate iris hyperemia, with a cumulative mean Hackett-McDonald Ocular Examination (OE) score of 7.
Forty-eight hours postcorneal incision (day 3), all signs had diminished, with only mild ocular changes and a mean cumulative group OE score of 4. By day 9 (just before the first challenge), the only observation for Durezol was mild conjunctival congestion. One day after the paracentesis challenge (day 10), mild-to-moderate conjunctival congestion, chemosis, iris hyperemia, aqueous cells and flare, and pupillary light sensitivity were observed, resulting in a mean cumulative OE score of 5. These findings gradually decreased in frequency and severity to a mean cumulative OE score of 2 before the second paracentesis challenge on day 15. The second and third paracentesis induced similar results, with the second paracenteses having a slightly diminished inflammation response.
Dosing with the IC placebo implant resulted in moderate conjunctival congestion, mild-to-moderate chemosis, moderate-to-severe iris hyperemia, mild-to-moderate aqueous cells and flare, and mildly altered pupillary light reflex with a mean cumulative score of 10 at day 2 (P < 0.001 compared with Durezol). On day 3, the mean cumulative OE score reduced to 7 and all findings were reduced to mild effects, except for conjunctival congestion and iris hyperemia that remained moderate (P < 0.0001 compared with Durezol). By day 9, findings were mild and the mean OE score was reduced to 3 (P < 0.0001 compared with Durezol). The aqueous centesis challenges resulted in similar inflammatory effects but to a lesser degree than the corneal incision. Each sequential centesis resulted in a milder inflammatory response (days 16 and 17 ranged from P < 0.05 to P < 0.01 compared with Durezol). The IC placebo OE scores were generally equal to or greater than the Durezol group.
After IC administration of ENV905 (1 implant, 40 μg DFBA per eye) and corneal incision on day 1, the eyes displayed mild-to-moderate signs of inflammation, including conjunctival congestion, chemosis, iris hyperemia, and aqueous cells and flare on day 2. OE scores peaked on day 2 with a mean score of 4 (P < 0.001 compared with Durezol, P < 0.0001 compared with placebo). By day 3, the pupillary light sensitivity was no longer observed, and other symptoms decreased in frequency (not statistically different compared with Durezol, P < 0.0001 compared with placebo). The rabbits had nearly recovered by day 9, just before the first paracentesis challenge (not statistically different compared with Durezol, P < 0.01 compared with placebo).
After the first paracentesis on day 9, ophthalmic exam scores rose to a group mean of two on day 10 (P < 0.001 compared with Durezol, P < 0.01 compared with placebo). All findings were considered mild. The eyes returned to baseline by day 15 (P < 0.0001 compared with Durezol, P < 0.001 compared with placebo). The second and third paracenteses induced mild ocular inflammation, with no mean OE scores rising above 3 and eyes returning to baseline within 2 days after challenge. Overall, the IC ENV905 groups had inflammatory observations that trended below the Durezol group, and they were equal to Durezol on several occasions (for the second and third paracenteses, days 15, 16, 17, 23, and 24 ranged from P < 0.01 to P < 0.0001 compared with Durezol). All eyes showed reduced inflammation throughout the duration of the study when compared with the IC placebo group (Fig. 3) (for the second and third paracenteses, days 15, 16, 17, 22, and 23 ranged from P < 0.05 to P < 0.0001 compared with placebo).

Total Hackett-McDonald ocular exam score (mean ± standard error of the mean) after induction of postoperative inflammation via corneal incision and paracentesis (one ENV905 intracameral implant, 40 μg difluprednate per eye).
The SCJ placebo implant produced similar results to the IC placebo, although the level of inflammation was decreased or equal to the IC placebo on all days except day 24. OE scores peaked at day 2 with a mean score of 8 (not statistically different compare to Durezol). None of the findings related to the corneal incision were considered severe. The SCJ placebo had a lower mean OE score than Durezol on day 15. Otherwise, values were equal to or greater than those seen with Durezol (days 3, 4, 9, 15, and 24 ranged from P < 0.05 to P < 0.0001 compared with Durezol). In general, inflammation displayed in the placebo groups tended to be lower than would be expected for a negative control group in this model, compared with previous studies conducted with this model. However, statistical differences were still observed when compared with groups that received an active implant.
After administration of SCJ ENV905 (1 implant, 393 μg DFBA per eye) and corneal incision on day 1, mild conjunctival congestion, iris hyperemia, and aqueous cells and flare were observed on day 2 (P < 0.0001 compared with Durezol, P < 0.001 compared with placebo). The peak mean OE score of 3 occurred on days 2 and 3, which were among the lowest mean peak scores in the study (day 3 not statistically different compared with Durezol, P < 0.0001 compared with placebo). Inflammation was substantially reduced when compared with the SCJ placebo on day 2 with an OE score of 8. OE scores returned to baseline by day 9 before the first paracentesis challenge (not statistically different compared with Durezol, P < 0.01 compared with placebo).
This challenge induced an inflammatory response where the OE scores increased to a mean of two on day 10 (P < 0.0001 compared with Durezol and P < 0.01 compared with placebo), and the animals were completely recovered by day 11 (P < 0.01 compared with Durezol, P < 0.05 compared with placebo). The second and third paracentesis resulted in mild inflammatory responses with mean OE scores of 2 and 1 that quickly dissipated to one or below. When compared with both the Durezol and placebo groups, SCJ ENV905 was able to markedly reduce the inflammatory effects of each of the paracentesis challenges (Fig. 4) (days 15, 16, 17, 23, and 24 ranged from P < 0.0001 to P < 0.01 compared with Durezol; days 16, 17, 23, and 24 ranged from P < 0.0001 to P < 0.05 compared with placebo).
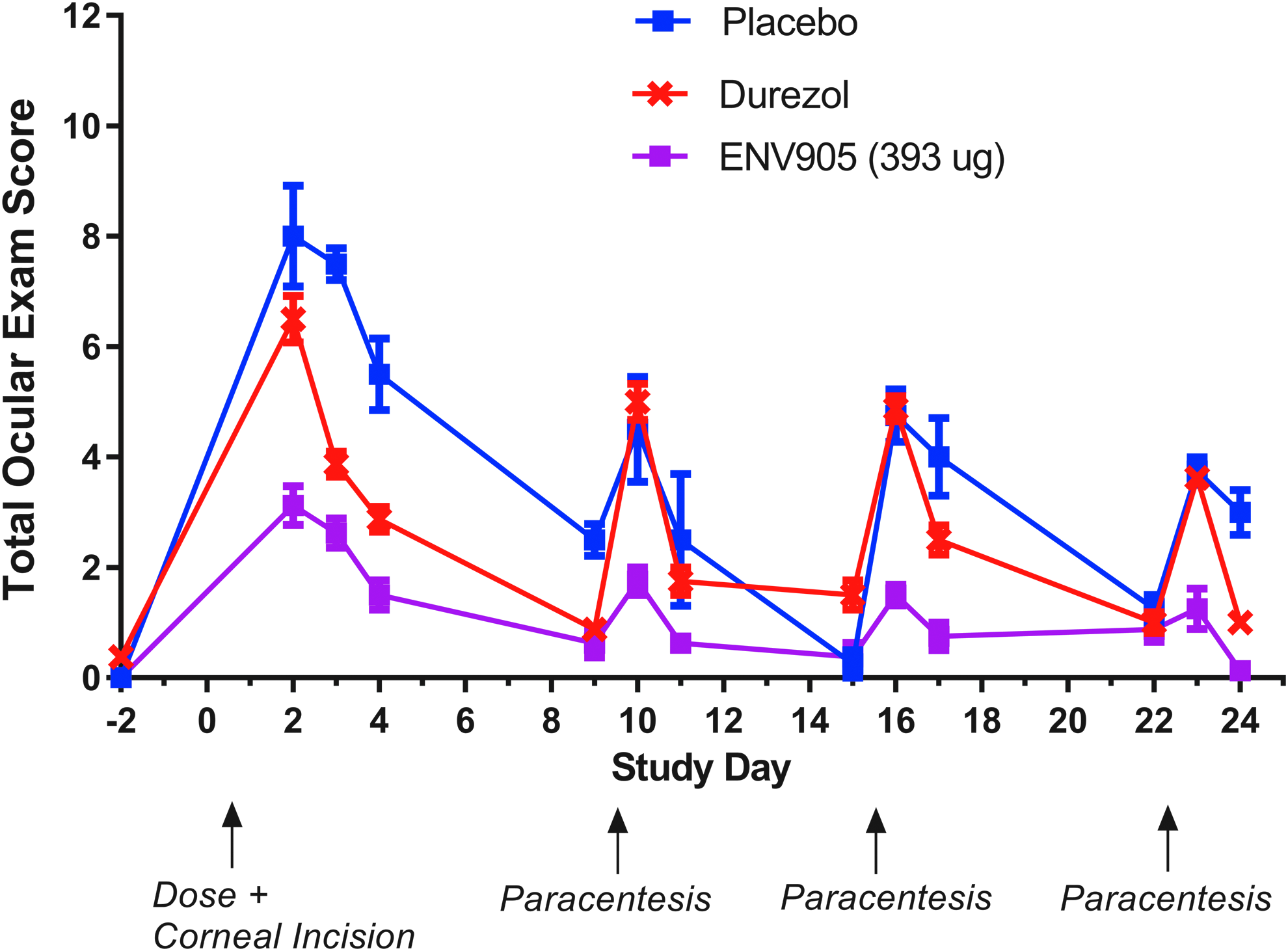
Total Hackett-McDonald ocular exam score (mean ± standard error of the mean) after induction of postoperative inflammation via corneal incision and paracentesis (1 ENV905 subconjunctival implant, 393 μg difluprednate per eye).
Ocular pharmacokinetics
For all formulations assessed in the pharmacokinetic (PK) studies, the parent DFBA was readily metabolized to the active metabolite DFB, and concentrations of DFB were generally higher in all matrices when compared with DFBA.
During the Durezol dosing period, concentrations of DFBA in ocular matrices generally remained consistent over the dosing period (Cmax = cornea>retina>trabecular meshwork>conjunctiva>aqueous humor>iris/ciliary body), were considerably lower than DFB in all matrices, and were not quantifiable at 2 weeks after the completion of the dosing period on day 28. For DFB in ocular samples, concentrations generally remained consistent over the dosing period, with some variability in the cornea and conjunctiva samples (Cmax = cornea>trabecular meshwork>conjunctiva>iris/ciliary body>retina>aqueous humor), and they were not quantifiable after the completion of the dosing period, with the exception of one out of four samples each in the cornea and bulbar conjunctiva on day 42 (2 weeks after the last dose).
These data demonstrate that exposure over time (AUClast) to the active metabolite DFB after topical Durezol administration was greatest in the cornea, trabecular meshwork, and conjunctiva, with lower exposure in the iris/ciliary body, aqueous humor, and retina, and with minimal exposure in the plasma; that sample concentrations remained consistent in all matrices over the 28-day dosing period as measured at 30 min postdose without noticeable accumulation; and that DFB was not quantifiable in most matrices at 2 weeks after cessation of topical dosing (day 42).
Mean plasma concentrations of DFB at 30 min after the final dose of the day ranged from 0.208 to 0.412 ng/mL, were generally consistent in concentration on days 1 through 28, and were not quantifiable after the cessation of dosing, demonstrating that systemic exposure after topical dosing was minimal but consistent and did not seem to accumulate over time (Fig. 5). Mean plasma Cmax was 0.41 ng/mL on day 2, and exposure over time calculated as AUClast was 8.83 d*ng/mL (Table 2).

Concentration of DFB in New Zealand White rabbit plasma after administration of either intracameral ENV905 (80 μg DFBA per animal) or Durezol (3,850 μg DFBA per animal). DFB, desacetyl difluprednate; DFBA, difluprednate; LLOQ, Lower Limit of Quantitation.
DFB, desacetyl difluprednate; DFBA, difluprednate; NA, not applicable; NC, not calculable.
After a single IC administration of one ENV905 implant (42.8 μg DFBA per eye, 85.6 μg DFBA per animal), DFBA concentrations in ocular matrices peaked on day 1 (Cmax = iris/ciliary body > aqueous humor > cornea > trabecular meshwork > retina > conjunctiva); Cmax values were considerably lower than DFB in all matrices with the exception of aqueous humor for which DFBA and DFB were similar; and samples were not quantifiable after days 2 or 4 (cornea only). For DFB in ocular samples, concentrations peaked on day 1 (Cmax = iris/ciliary body>cornea>trabecular meshwork>aqueous humor>conjunctiva>retina); were markedly decreased in concentration by days 4 or 7; and were not quantifiable in most samples after days 7 or 14 (cornea only), with the exception of one quantifiable sample out of four in either conjunctiva or trabecular meshwork (day 14). These data demonstrate that exposure over time (AUClast) to the active metabolite DFB after a single administration of one ENV905 IC implant per eye was greatest in the iris/ciliary body, cornea, and trabecular meshwork (Figs. 6–8), with lower exposure in the aqueous humor, conjunctiva, and retina, and with very minimal exposure in the plasma; that exposure peaked on day 1 and remained above physiologically relevant concentrations through days 7 or 14; and that DFB was not quantifiable in any matrices after day 14 (Table 2).
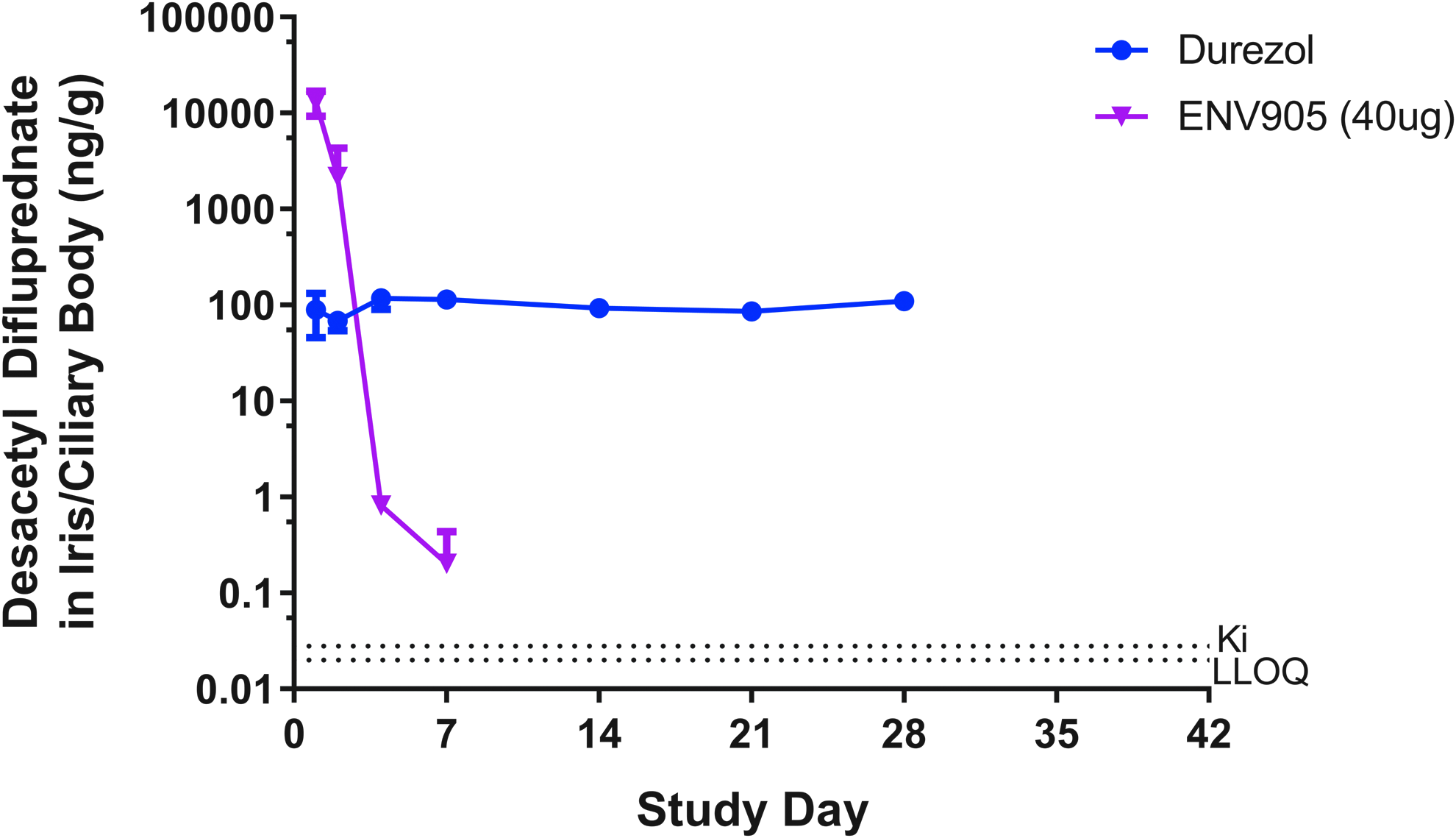
Concentration of DFB in New Zealand White rabbit iris/ciliary body after administration of either intracameral ENV905 (40 μg DFBA per eye) or Durezol (1,925 μg DFBA per eye). DFB, desacetyl difluprednate; DFBA, difluprednate; LLOQ, Lower Limit of Quantitation.
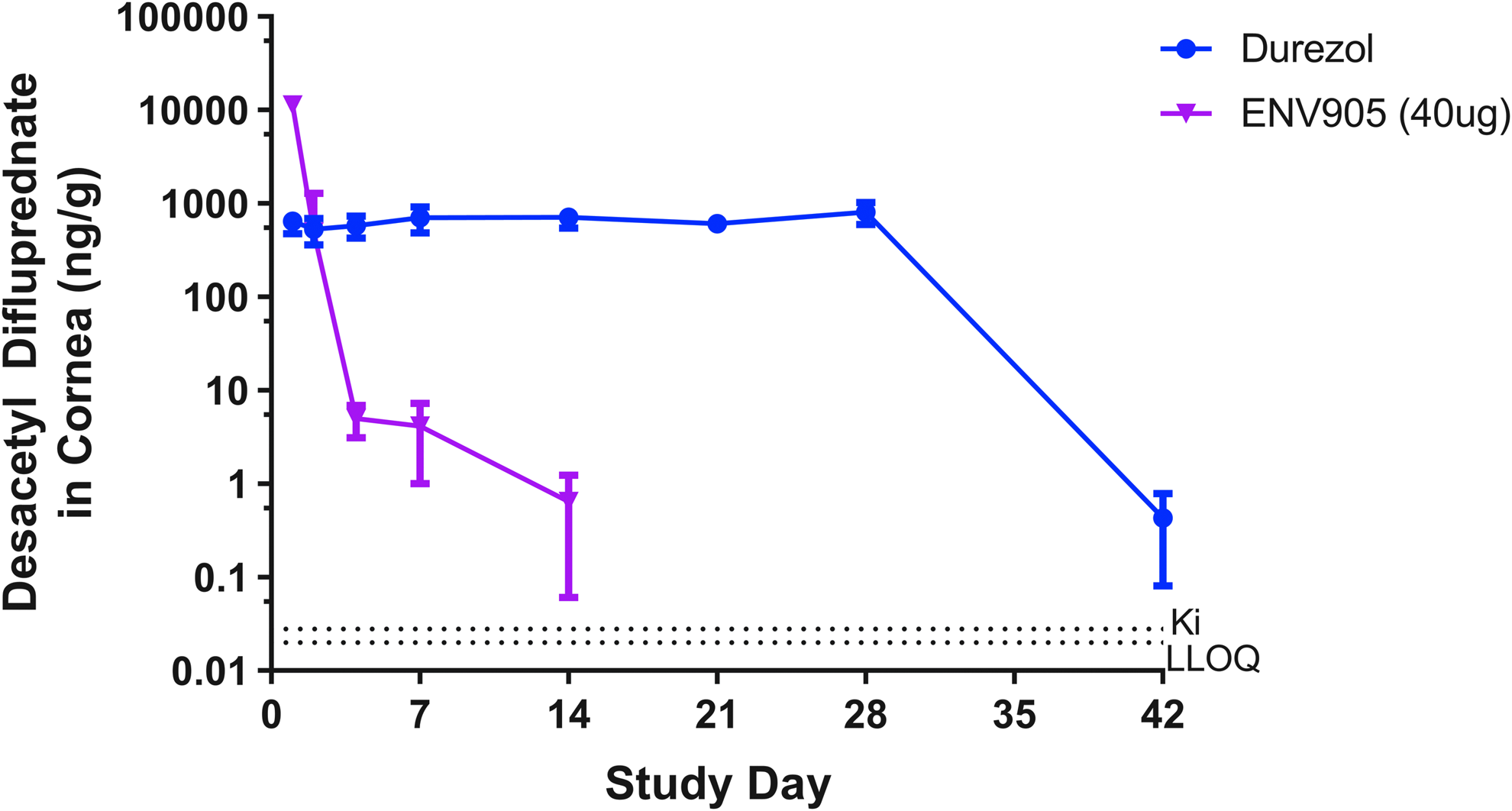
Concentration of DFB in New Zealand White rabbit cornea after administration of either intracameral ENV905 (40 μg DFBA per animal) or Durezol (1,925 μg DFBA per eye). DFB, desacetyl difluprednate; DFBA, difluprednate; LLOQ, Lower Limit of Quantitation.

Concentration of DFB in New Zealand White rabbit trabecular meshwork after administration of either intracameral ENV905 (40 μg DFBA per animal) or Durezol (1,925 μg DFBA per eye). DFB, desacetyl difluprednate; DFBA, difluprednate; LLOQ, Lower Limit of Quantitation.
Plasma concentrations of DFB were quantifiable on day 1 (2 h postdose) and were not quantifiable from days 2 through 42, demonstrating that systemic exposure was limited to the first few hours postdose. Mean plasma Cmax was 0.99 ng/mL on day 1, and further PK analysis could not be conducted.
SCJ delivery of ENV905 resulted in measurable DFBA and DFB at the dose site (sclera/conjunctiva at the area of implant placement) that was quantifiable through day 84. DFB was also quantifiable through day 84 in the cornea, through day 56 in the bulbar conjunctiva, and through day 42 in the iris/ciliary body. Retina samples were quantifiable on days 14 and 28, and they were generally below the limit of quantitation (BLQ) on days 42 through 84. Two out of four aqueous humor samples were quantifiable on day 28, and all other samples were BLQ. Plasma samples peaked on day 1 at 3.85 ng/mL, were quantifiable at decreasing concentrations through day 14, and all later samples were BLQ (Table 3). As the pharmacokinetic profile for SCJ ENV905 showed a longer duration of ocular exposure than was planned for in the target product profile of ENV905, further assessments of this formulation were discontinued.
BLQ, below the limit of quantitation; DFB, desacetyl difluprednate; DFBA, difluprednate; NA, not applicable; NC, not calculable.
Discussion
We investigated the efficacy, ocular pharmacokinetics, and tolerability of a single bilateral administration of SCJ or IC ENV905 (DFBA) Ophthalmic Implant. As the tolerability of PEG-based ophthalmic implants is not fully documented, we wanted to ensure that ocular tolerability was assessed before administration in a toxicology study. Studies in New Zealand White rabbits demonstrated that ENV905 was well tolerated regardless of administration route for a maximum of 4 weeks (data from non-Good Laboratory Practice [GLP] tolerability studies not shown, Verhoeven 2015). Observations conducted after administration of the IC ENV905 implant showed that the implant bio-eroded within the first few days after dosing, with the implant nestling into the iridocorneal angle immediately on injection, and no visible implant fragments were observed after 24–48 h postdose. A GLP toxicology study was conducted for IC ENV905, which demonstrated a no-adverse-effect level of the high dose of three ENV905 implants per eye (132 μg DFBA per eye) (Robeson, et al. Association for Research in Vision and Ophthalmology. Invest Ophthalmol Vis Sci, 2016; 57:E-Abstract 4013).
The ENV905 IC implant demonstrated a superior anti-inflammatory profile in an animal model of postoperative inflammation when compared with the marketed product Durezol, while incorporating significant dose sparing. Even at later time points during weeks 3 and 4, when the pharmacokinetics indicated that most of the DFB had cleared the eye, IC ENV905 still induced a superior decrease in inflammation after repeat paracentesis. The pharmacokinetic profile showed a burst release of DFBA from the implant at early time points, thereby delivering the highest concentration of corticosteroid at the time of greatest inflammation postsurgery. The implant then continued to release and distribute the corticosteroid to the target tissue of iris/ciliary body and cornea in a self-tapering manner. Importantly, plasma exposure was minimal and limited to the early time points, resulting in decreased systemic exposure when compared with Durezol.
SCJ delivery of ENV905, while requiring a higher dose per eye compared with IC delivery to suppress induced postoperative inflammation (earlier data with decreased dose per eye not shown, Verhoeven, 2015), produced quantifiable DFB concentrations in ocular structures for a maximum of 84 days, but with lower concentrations in the anterior chamber compared with IC ENV905 and Durezol. Of interest was the balance between efficacy and the concentration in ocular matrices, demonstrating that high concentrations of DFB in ocular tissue for a sustained period, as seen with Durezol, were not required to effectively suppress inflammation in a model of postoperative inflammation. The SCJ location of delivery, though a viable therapeutic administration technique, provided a longer duration of exposure than was warranted for this indication.
As the target product profile for ENV905 mandated a shorter duration of action, and input from key opinion leaders in the cataract surgery field showed a preference for IC administration during cataract surgery for this product, the SCJ implant was discontinued from further development at Envisia. However, the SCJ delivery system of PRINT implants may be a useful platform for other indications and active pharmaceutical ingredients such as anti-infectives or antihistamines.
Interestingly, the pharmacokinetics of Durezol in this study showed the highest exposure in the cornea and the trabecular meshwork (Table 2). As Durezol (like other corticosteroids) is known to induce IOP spikes in some susceptible patients, perhaps decreasing the exposure in the trabecular meshwork as seen with ENV905 and limiting the peaks and troughs associated with daily topical dosing could mitigate the risk of these IOP elevations.
The standard of care for Durezol requires a total dose of ∼1,925 μg DFBA per eye over the course of 4 weeks, for a total of 77 dosing occasions, each requiring the patient to remember to take the drop and to have the manual dexterity to administer the drop correctly. Conversely, a single administration of IC ENV905 supplies only 40 μg of DFBA per eye, with no additional dosing occasions required. The IC implant rapidly moves to rest in the iridocorneal angle postdose, and degrades over time, causing no obstruction of vision.
In conclusion, ENV905 was well tolerated, suppressed inflammation in a postoperative inflammation model, and delivered therapeutically relevant concentrations of DFBA to the target tissue with an appropriate pharmacokinetic profile. IC delivery and the optimized IC implant formulation of ENV905 were chosen for continued drug product development due to the preferred PK profile as well as physician preference for location of drug delivery during cataract surgery. SCJ delivery of the ENV905 implant, while producing a duration of exposure that was deemed to be in excess of the requirements for corticosteroid drug delivery in ocular surgery, could be utilized for other therapeutic areas of interest in future programs. A single administration of ENV905 during ocular surgery could replace daily topical corticosteroid eye drops, thereby removing the burden of treatment from patients and into the hands of the physicians, limiting the impact of non-compliance on therapeutic outcomes.
Footnotes
Acknowledgments
The authors thank Melissa Hernandez and Jeremy Hansen of Envisia Therapeutics for their support of this project.
Author Disclosure Statement
R.S.V., A.G., R.R., T.N., and B.Y. are employees and equity holders of Envisia Therapeutics. B.C.G. is a consultant to Envisia Therapeutics. D.C., C.S., and L.H. have no financial interests to disclose.