
Abstract
Abstract
Purpose:
The purpose of this study was to develop and evaluate a novel dexamethasone- and tobramycin-loaded microemulsion for its potential for treating anterior segment eye infections.
Methods:
The microemulsion was evaluated for pH, particle size, zeta potential, light transmittance, morphology, and in vitro drug release. Sterility of the microemulsion was evaluated by direct as well as plate inoculation methods. Anti-inflammatory activity of dexamethasone, bactericidal activity of tobramycin, and cytotoxicity of the microemulsion were assessed and compared to that of the marketed eye drop suspension (Tobradex®). Histological evaluation was performed in bovine corneas to assess the safety of microemulsion in comparison to Tobradex suspension. In addition, the stability of the microemulsion was studied at 4°C, 25°C, and 40°C.
Results:
The pH of the microemulsion was close to the pH of tear fluid. The microemulsion displayed an average globule size under 20 nm, with light transmittance around 95%–100%. The aseptically prepared microemulsion remained sterile for up to 14 days. The cytotoxicity of the microemulsion in bovine corneal endothelial cells was comparable to that of the Tobradex suspension. The anti-inflammatory activity of dexamethasone and the antibacterial activity of tobramycin from the microemulsion were significantly higher than those of the Tobradex suspension (P < 0.05). Histological evaluation showed an intact corneal epithelium without any signs of toxicity, and the developed microemulsion was found to be stable at 4°C and 25°C for 3 months.
Conclusion:
In conclusion, the developed microemulsion could be explored as a suitable alternative to the marketed suspension for treating anterior segment eye infections.
Introduction
D
Ocular infections are mostly chronic in nature and are characterized by inflammation of the cornea, conjunctiva, and eyelids. Common ophthalmic infections include conjunctivitis, blepharitis, keratitis, keratoconjunctivitis, and sty. The management of anterior segment ocular infection and inflammation requires prompt diagnosis and treatment to avoid any serious visual complications. 7 Bacterial infections are commonly treated using a combination of antibiotic and steroidal drugs. The antibiotic reduces the infection, while the corticosteroid treats the inflammation associated with the infection. 8
Dexamethasone is a steroidal anti-inflammatory drug with low aqueous solubility (0.16 mg/mL) and is moderately lipophilic in nature (logP = 1.8). 9 Dexamethasone inhibits phospholipase A2 activity, required for the release of arachidonic acid, thereby preventing the release of prostaglandins, thromboxanes, and leukotrienes. 10 Tobramycin is an aminoglycoside antibiotic used for treating various types of bacterial infections. Tobramycin irreversibly binds to the bacterial 30S and 50S ribosomal subunits, preventing the formation of 70S complex, which eventually inhibits mRNA translation, leading to cell death. 11
Currently, dexamethasone and tobramycin are marketed in combination by Alcon Laboratories, Inc. as suspension eye drops (Tobradex® and Tobradex ST®) and ointment (Tobradex). The usual dose of Tobradex suspension for treating mild-to-moderate infection is 1 or 2 drops in the affected eye(s) every 4 h, whereas in the case of severe infection, the dose is increased to 2 drops every hour until the condition subsides. Similarly, a 1.25 cm ribbon of Tobradex ointment is applied to the conjunctival sac 2–3 times a day in mild-to-moderate infection, whereas in the case of severe infection, the same dose is applied every 3–4 h. 12
The administration of drugs by a DROP-TAINER bottle (in the case of solutions and suspensions) or ointment tube is highly challenging in both adults and young children due to the lack of acuity and inability to aim effectively. 13 Moreover, drug absorption from a suspension dosage form is highly varied. This erratic drug absorption is attributed to the clearance of a larger percentage of drug particles from the precorneal area before drug dissolution and absorption can take place. Furthermore, the intrinsic drug dissolution rate fluctuates with the constant in and out flow of the lacrimal fluids. 7
An ointment, on the contrary, provides improved ocular retention time. However, the drug binds to the ointment base and limits its penetration into the eye. 14 In addition, suspension and ointment formulations interfere with the vision and cause ocular side effects such as irritation and redness of the eye. 15 Therefore, to overcome these drawbacks and enhance patient acceptance, the current research is focused on exploring a novel microemulsion system for delivering dexamethasone and tobramycin.
An ideal ocular carrier system should improve the precorneal residence time, provide better bioavailability, and decrease the dosing frequency. 16 Microemulsions are colloidal oil-in-water (o/w) or water-in-oil (w/o) nanodispersions, stabilized by a surfactant and cosurfactant system. They are prepared by mixing an oil phase containing oil, surfactant, and cosurfactant with an aqueous phase. 17 Microemulsions have emerged as promising systems for ocular drug delivery. They are advantageous over other delivery systems due to their ease of manufacture and sterilization and their ability to deliver both hydrophilic and lipophilic drugs. Microemulsions are thermodynamically stable systems that enable higher levels of drug in ocular tissues. They also help in reducing the dosing frequency. 17 Ocular microemulsions of several drugs such as ofloxacin, 3 timolol, 18 prednisolone, 19 and pilocarpine 20 showed sustained release with improved bioavailability.
Ricinoleic acid is known for its antibacterial properties.7,21 Topical application of ricinoleic acid has shown analgesic and anti-inflammatory effects in several animal models with acute and subchronic inflammation. 22 It also has an ability to spread readily over the aqueous compartment of the tear film, thereby reducing the evaporation and increasing the stability of tear film. 23 Therefore, we hypothesize that a microemulsion made up of ricinoleic acid as oil phase could work synergistically with dexamethasone and tobramycin in reducing inflammation and infection. In addition, this unique thermodynamically stable system could prolong the residence time, improve the corneal permeability of both drugs, and decrease the dosing frequency. The objective of this study was to develop and characterize an o/w microemulsion system composed of ricinoleic acid (oil phase), cremophor and 1-butanol (surfactant and cosurfactant), and water (aqueous phase), loaded with dexamethasone and tobramycin for treating anterior segment eye infections.
Methods
Materials
Dexamethasone (Lot C163997) and tobramycin (Lot C164877) were procured from PCCA (Houston, TX). Kolliphor® EL (Lot BCBQ5632V), lipopolysaccharides (LPS) from Escherichia coli 055:B5 (Lot 105M4134V), N-(1-naphthyl) ethylenediamine dihydrochloride (Lot SZBF1190V), and sulfanilamide (Lot SLBN9189V) were purchased from Sigma Aldrich (St. Louis, MO). Ricinoleic acid (Lot XUWOODD) was procured from TCI (Portland, OR). 1-butanol (Lot A0317960) and 2, 4-dinitroflurobenzene (Lot A0351447) were purchased from ACROS (Fair Lawn, NJ). 3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyl tetrazolium bromide (MTT) powder (Lot 2626103) was procured from Millipore (Billerica, MA). Dulbecco's modified Eagle's medium (DMEM, Lot 10092157), 0.25% trypsin, and 2.21 mM ethylenediaminetetraaceticacid (EDTA) 1 × (Lot 25053365) and 1× trypsin-EDTA solution (Lot C2030) were purchased from Corning (Manassas, VA). Polysorbate 80 (Lot 120589), potassium phosphate monobasic (Lot 123304), sodium hydroxide (Lot 101166), sodium bicarbonate (Lot 116734), and hydrochloric acid (Lot 091256) were supplied from Fisher Scientific (Fair Lawn, NJ). Ethanol (Lot 223512) was purchased from Decon Laboratories, Inc. (King of Prussia, PA). Benzalkonium chloride (BAK, Lot Y52651G15) was supplied by Ruger (Irvington, NJ). EDTA disodium salt dihydrate (Lot B0136110A) was procured by ACROS. Tryptic soy broth (soybean casein digest medium-BactoTM, Lot 2030828), Mueller–Hinton (MH) broth (Lot 108187B), and dimethyl sulfoxide (DMSO, Lot 104549) were purchased from Fisher Scientific (Pittsburgh, PA). Taxo™ blank paper discs (Lot 232189) were procured from Becton Dickinson and Company (Sparks, MD). Tobramycin standard 10 μg discs (Lot 1750529) were purchased from Oxoid (Hants, United Kingdom). Transmission electron microscopy (TEM) grids were purchased from Ted Pella, Inc. (Redding, CA). High-performance liquid chromatography (HPLC) solvents, including acetonitrile (Lot 157773) and methanol (Lot 162124), were supplied by Fisher Scientific (Pittsburgh, PA). Distilled deionized water was used for the preparation of microemulsions.
Construction of pseudoternary phase diagrams
Pseudoternary phase diagrams of oil phase (ricinoleic acid), surfactant (cremophor EL), cosurfactant (1-butanol), and aqueous phase (water) were developed to determine the regions of microemulsion formation. Four phase diagrams were constructed with surfactant to cosurfactant ratios of 1:4, 2:3, 3:2, and 4:1 using the conventional water titration method at room temperature. The final compositions of clear, single-phase formulations were converted to weight percentages and were plotted as points in the ternary diagrams. The areas covered by these points representing the regions of microemulsion formation were plotted using TernPlot-Excel Plotting program.
Preparation of blank microemulsion
From the ternary phase diagrams, a composition of ricinoleic acid (2.5% w/w), cremophor EL (9.3% w/w), 1-butanol (6.2% w/w), and deionized water (82% w/w) was selected for further characterization and evaluation. The ratio of surfactant to cosurfactant was kept at 3:2. The microemulsion was prepared by a spontaneous emulsification technique. It involves the mixing of cremophor EL and 1-butanol for a few seconds, using a fixed speed vortex mixer (Fisher Scientific, Pittsburgh, PA) to produce a homogenous mixture. The oil phase (ricinoleic acid) was then added to the surfactant mixture and vortexed to form a self-nanoemulsifying mixture. Finally, increasing amounts of deionized water were gradually added to the mixture with gentle stirring until a clear microemulsion system was obtained.
Preparation of dexamethasone- and tobramycin-loaded microemulsion
Dexamethasone- and tobramycin-loaded microemulsion was prepared by adding 0.1% of dexamethasone to self-nanoemulsifying mixture and vortexed until a homogenous mixture was obtained. Tobramycin (0.3%) was dissolved in distilled deionized water (82% w/w), and this was gradually added to the self-nanoemulsifying mixture with gentle stirring, which resulted in the formation of clear and transparent microemulsion. In addition, EDTA disodium dihydrate (0.1%) was added to the formulation as an antioxidant, and BAK (0.01%) was added for its preservative property. The composition of the microemulsion is detailed in Table 1.
HPLC analysis of dexamethasone
Dexamethasone was analyzed using HPLC (Waters Alliance e2695 separation module; Milford, MA) equipped with a 2998 PDA detector and a reverse-phase C8 column (5 μm, 100 Å; Luna, Torrance, CA). Mobile phase composed of water and acetonitrile (50:50) was pumped at a flow rate of 1.0 mL/min. The absorbance of dexamethasone was measured at 242 nm, and the drug content in the samples was determined by plotting a calibration curve. A stock solution of 1,000 μg/mL of dexamethasone was prepared using methanol. The calibration standards, ranging from 0.39 to 50 μg/mL, were prepared in the mobile phase. Each calibration standard was analyzed in triplicate, and the average peak area was plotted against the amount of dexamethasone to obtain the calibration curve.
UV analysis of tobramycin
Tobramycin was analyzed using a UV-Vis spectrophotometer (Agilent 8453, UV-Vis Spectroscopy System). Calibration standards (5 mL) ranging from 50 to 250 μg/mL were taken in 10 mL glass tubes, to which 1 mL of 2% sodium bicarbonate solution was added and mixed. Then, 2 mL of freshly prepared 95% ethanolic solution of 2, 4-dinitroflurobenzene was added (0.25 mL/100 mL) and mixed thoroughly. After 20 min, the solution was neutralized by adding 0.5 mL of 1 M HCl. The glass tubes were tapped gently to remove any carbon dioxide bubbles, and the absorbance was determined at 415 nm using distilled water as a blank. 24 Each standard was analyzed in triplicate, and the absorbance was plotted against the concentration of tobramycin to obtain the calibration curve.
Droplet size
The droplet size was measured by the dynamic light scattering (DLS) technique using Nicomp 380 ZLS (Particle Sizing Systems, Santa Barbara, CA). Samples of microemulsion were placed into 6 × 50 mm borosilicate glass tubes (Kimble Chase, Vineland, NJ) and positioned in the path of 100 mW He–Ne laser with a wavelength of 658 nm. The neutral density filter was adjusted until the scattered intensity fluctuated around 300 kHz. The light scattered was collected at 90° and detected using a photodiode array detector. The software automatically tuned the channel width and baseline, and Nicomp distribution was considered for chi square values >3. 25 Each sample was analyzed 3 times, and the mean volume-weighted diameter was determined.
Zeta potential
Zeta potential was measured using Nicomp 380 in electrophoretic light scattering mode. Samples of the microemulsion were placed in a plastic cuvette and positioned in the path of He–Ne laser. The light scattered was collected at 14.8° and detected using a photomultiplier tube. Each sample was analyzed 3 times, and the zeta potential was determined from the average of the runs.
pH
The pH of the samples was measured using Accumet® Excel XL 25 pH meter (Fisher Scientific, Pittsburgh, PA). Before every use, the pH meter was calibrated using standard buffer solutions of pH 4.00, 7.00, and 10.00. All measurements were done in triplicate at 25 ± 2°C, and the data are expressed as mean ± standard deviation (SD).
Clarity
The clarity of the samples was measured using UV-Vis spectrophotometer at 400 nm. Deionized water was used as a blank for the analysis. All measurements were done in triplicate, and the clarity was expressed as percent transmittance.
Differential scanning calorimetry
Thermal and physical state properties of dexamethasone, tobramycin, blank microemulsion, and drug-loaded microemulsion were determined using a differential scanning calorimeter (DSC; 822e Mettler Toledo) equipped with a TS0801RO sample robot and TS0800GCI gas flow system. Samples of 5–12 mg were weighed using Mettler MT5 microbalance into a 100 μL aluminum pan, covered with a lid, and quickly sealed using a mechanical crimper. The study was performed at a heating rate of 10°C/min over a range of 10–300°C. Nitrogen was used as a standard purging gas at 20 mL/min to prevent oxidation of the samples. Star-e software V8.10 was used to obtain the DSC scans.
Transmission electron microscopy
The morphology of the microemulsion was studied using TEM (HITACHI HD-2300 A, Ultrathin Film Evaluation System by Hitachi High Technologies America, Pleasanton, CA). A small drop of the formulation was placed on a holey carbon 400 mesh copper grid (Ted Pella, Redding, CA) and then negatively stained using 2% phosphotungstic acid solution (Fisher Scientific, Pittsburgh, PA). The copper grids were dried overnight, and TEM images were captured using Quartz PCI version 8 software.
In vitro drug release study
The in vitro release of dexamethasone from the microemulsion was performed using the dialysis bag method. A dialysis membrane (Spectrum/Por®) of molecular weight cutoff 12,000–14,000 Da and pore size of 0.45 μm was used for the study. One milliliter of the formulation was placed in the dialysis bag, sealed, and then introduced into glass bottles containing 200 mL of phosphate buffer (pH 7.4) and 0.025% (w/v) Tween 80. The bottles were placed into a shaker bath maintained at 34 ± 0.5°C and 60 rpm. At predetermined time intervals, a 1 mL sample was withdrawn from each bottle, and an equal volume of fresh buffer was replaced. The study was conducted in triplicate, and samples withdrawn were analyzed using HPLC.
Sterility test
The microemulsion was evaluated for sterility to assess whether the preparation was free from microorganisms. Formulation sterility was tested using plate and direct/tube inoculation methods. The study was carried out under aseptic conditions, as per our published protocol.26,27 All the glassware used for the study was autoclaved, and nonautoclavable materials were thoroughly wiped with isopropyl alcohol. The formulation was sterilized by passing the microemulsion through a Millex® sterile nylon syringe filter (0.22 μm). Liquid culture of Staphylococcus aureus (Rosenbach ATCC® 6538) was grown in trypsin soy broth at 37°C for 24 h. The concentration of bacteria was determined using Spectronic 20 Genesys spectrophotometer (Spectronic Instruments) at 625 nm. By using sterile water as blank, absorbance of the culture was compared to 0.5 McFarland standard of concentration 1.5 × 108 colony forming unit (CFU)/mL. The final concentration of the liquid culture was adjusted to 102 CFU/mL by serial dilution with sterile deionized water. Four sets of controls and a sample were prepared. The compositions are summarized in Table 2. All the tubes were tested in duplicate and were incubated at 37°C for 2 weeks. For the plate inoculation method, MH agar plates were prepared by pouring molten agar into presterilized monoplates. One hundred microliters of sample was withdrawn from the tubes tested for direct inoculation method and uniformly spread on MH agar plates on days 0, 7, and 14. The plates were also tested in duplicate and were incubated at 37°C for 24 h to detect any visual bacterial growth.
CFU, colony forming unit.
Cytotoxicity study
The biocompatibility of the formulation was tested and compared with Tobradex suspension using bovine corneal endothelial cells by MTT assay. Bovine eyes were obtained from Kastel's Slaughter House and Processing Center (Riga, MI), and the corneal cells were harvested according to a published protocol. 28 The cells were plated in DMEM supplemented with 10% fetal bovine serum (FBS), penicillin (100 U/mL) and streptomycin (100 μg/mL) and were then incubated at 37°C. After the cells reached ∼80%–90% confluency, they were seeded into a 96-well plate at a density of 10,000 cells/well. The cells were incubated in a 37°C and 5% CO2 environment for 24 h to assist cell adhesion. Cells were then exposed to negative control composed of 200 μL DMEM, positive control composed of DMEM with 20% DMSO, DMEM mixed with 0.01%,0.1%, 1%, 5%, 50%, 100% of microemulsion, and DMEM mixed with 0.01%,0.1%, 1%, 5%, 50%, 100% of Tobradex eye drop suspension. After 60 min, the medium was aspirated, fresh DMEM was replaced with 10% MTT reagent, and the cells were incubated in 5% CO2 at 37°C for 3 h. The yellow medium was then removed, and 150 μL of 100% DMSO was added to each well to allow dissolution of the formazan salt formed, and the viable cells were quantified using a microplate reader at 570 nm.
Anti-inflammatory assay
The anti-inflammatory activity of the drug-loaded microemulsion was compared to the Tobradex suspension using microglial cells by Griess assay. Microglial cells were plated with DMEM supplemented with 10% FBS, streptomycin (100 μg/mL), and penicillin (100 U/mL) and incubated at 37°C and 5% CO2. After the cells reached ∼80%–90% confluency, they were seeded in a polylysine-coated 24-well plate at a density of 2 × 105 cells/well. The cells were incubated at 37°C and 5% CO2 for 24 h. Cells were then pretreated with drug-loaded microemulsion and Tobradex suspension at concentrations of 0.001%, 0.01%, and 0.1% for 1 h. Except for the negative control, cells were stimulated using LPS (LPS obtained from E. coli 055:B5) at a concentration of 200 ng/mL. After 24 h, cells were subjected to Griess assay for determining the presence of nitrite ions. Equal volumes of Griess reagent (0.4% naphthylethylenediamine dihydrochloride, 2% sulfanilamide in 5% phosphoric acid) and microglial culture supernatant were mixed and incubated for 10 min. The absorbance of the cells was measured using a Synergy H1 microplate reader with Gen5 Data Analysis Software at 540 nm.
Antimicrobial disk diffusion susceptibility test
Preparation of inoculum
The antimicrobial activity of the microemulsion was compared to the Tobradex suspension using E. coli by the disk diffusion susceptibility test. The bacteria were subcultured and tested in their log phase of growth to ensure that results obtained were valid. Using a sterile cotton swab, 4 or 5 isolated colonies of the bacteria were transferred into a glass tube containing 3 mL of saline and vortexed to obtain a uniform suspension. This suspension was prepared just before inoculating the agar plate with bacteria. The turbidity of the inoculum was adjusted to that of 0.5 McFarland standard by diluting it with sterile saline if the suspension obtained was too turbid or by addition of more bacteria if the suspension obtained was too light.
Inoculation of MH agar plate
A sterile cotton swab was dipped into the inoculum tube and rotated against the sides of the tube using firm pressure, to ensure that there was no dripping due to excessive fluid. The MH agar plate was then inoculated by streaking 6 times with the swab, thereby covering the entire agar surface. Each time, the plate was rotated ∼60° to ensure uniform distribution of the inoculum. The plates were then allowed to dry at room temperature for 3–5 min before placing the impregnated discs.
Preparation and placement of impregnated discs
Ten microliters of microemulsion and Tobradex suspension containing 30 μg of tobramycin was carefully transferred onto blank sterile disks. A standard disc of tobramycin (10 μg) was used as a control and to ensure that the medium supported bacterial growth beyond the zone of inhibition. With the use of a sterile forceps, discs containing microemulsion, Tobradex suspension, and tobramycin (standard) were equidistantly placed onto the agar plate and were pressed gently to ensure complete contact with the surface of the agar.
Incubation of agar plates and measurement of zones of inhibition
The inoculated plates were incubated at 37°C for 24 h, and the zones of inhibition were measured. All the measurements were taken by viewing the back of the plate against a dark nonreflecting surface illuminated with reflected light. The diameters of the zones were measured to the nearest millimeter using a ruler.
Histological evaluation in bovine cornea
To ensure the safety of the prepared microemulsion for ocular administration, histology was performed using bovine corneas, and the evaluation was compared to the Tobradex suspension. Fresh bovine corneas were obtained from Kastel's Slaughter House and Processing Center. The bovine corneas were rinsed with phosphate buffer (pH 7.4) and then treated with 1 mL of the prepared microemulsion and marketed suspension. After 3 h of treatment, the tissues were fixed using 10% formalin solution for 24 h and then stored in 70% ethanol. The formalin-fixed tissues were processed using an automatic tissue processor and were transferred to a mold, to which hot paraffin wax (65°C) was added using a paraffin dispenser. The mold was then placed on a cooling surface for 30 min until the paraffin was completely hardened. Later, the wax block was removed and sectioned using a microtome at a thickness of 5 μm. The sections were then placed on microscope slides, stained using hematoxylin and eosin, and observed under a microscope to detect any morphological changes.
Stability test
Stability testing is a prerequisite for the approval of any pharmaceutical product, as it ensures the product quality, safety, and efficacy throughout the shelf life. 29 To assess the physical and chemical stability of the prepared formulation, microemulsion samples were stored at different temperatures (4°C, 25°C, and 40°C) for a period of 3 months. Samples were withdrawn at regular intervals of 0, 30, 60, and 90 days and evaluated for pH, particle size, clarity/transmittance, and drug content.
Statistical analysis
All the data obtained are expressed as mean ± SD. Analysis of variance was applied to analyze the significant difference between samples followed by Student's t-test. P < 0.05 was considered to be significant in all the cases.
Results
Construction of pseudoternary phase diagrams
Four phase diagrams were developed, and the regions of microemulsion formation were determined. The phase diagrams constructed using 1:4, 2:3, 3:2, and 4:1 (surfactant to cosurfactant) ratios are shown in Fig. 1. The microemulsion region increased with the ratio of surfactant to cosurfactant (1:4 < 2:3 < 3:2 < 4:1). However, the microemulsion region containing 3:2 ratio of surfactant to cosurfactant was considered for further studies due to its lower surfactant concentration. From the microemulsion region in the pseudoternary phase diagram Fig. 1C, a system was selected for further characterization and evaluation (Table 3).

Pseudoternary phase diagrams of microemulsion containing cremophor EL and 1-butanol in
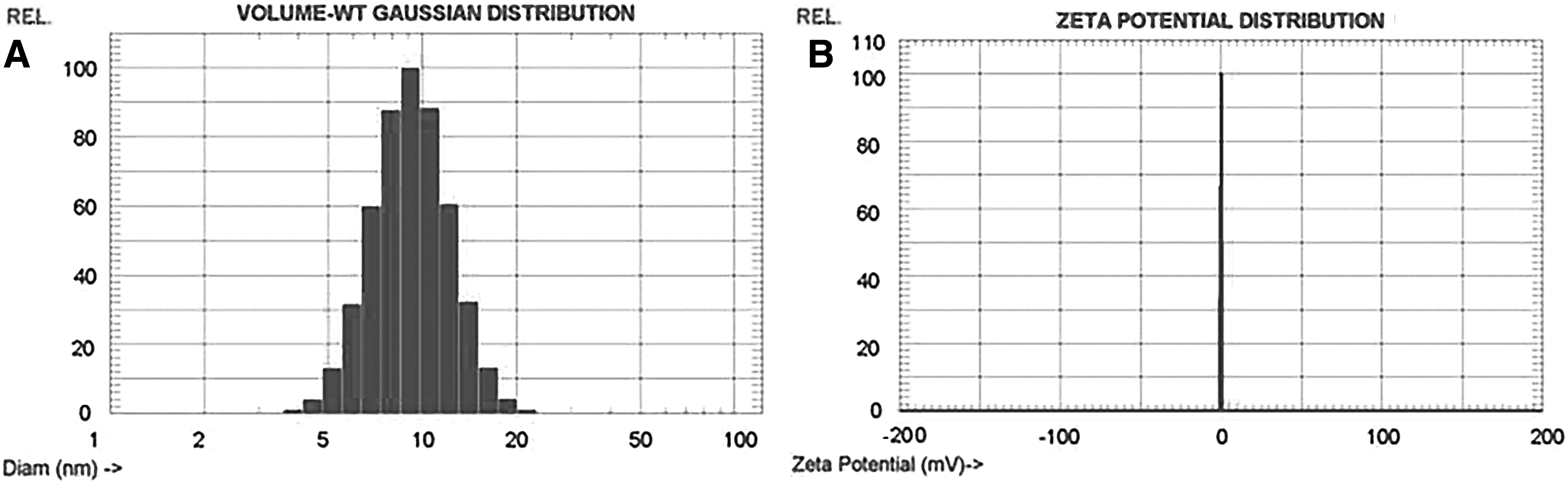
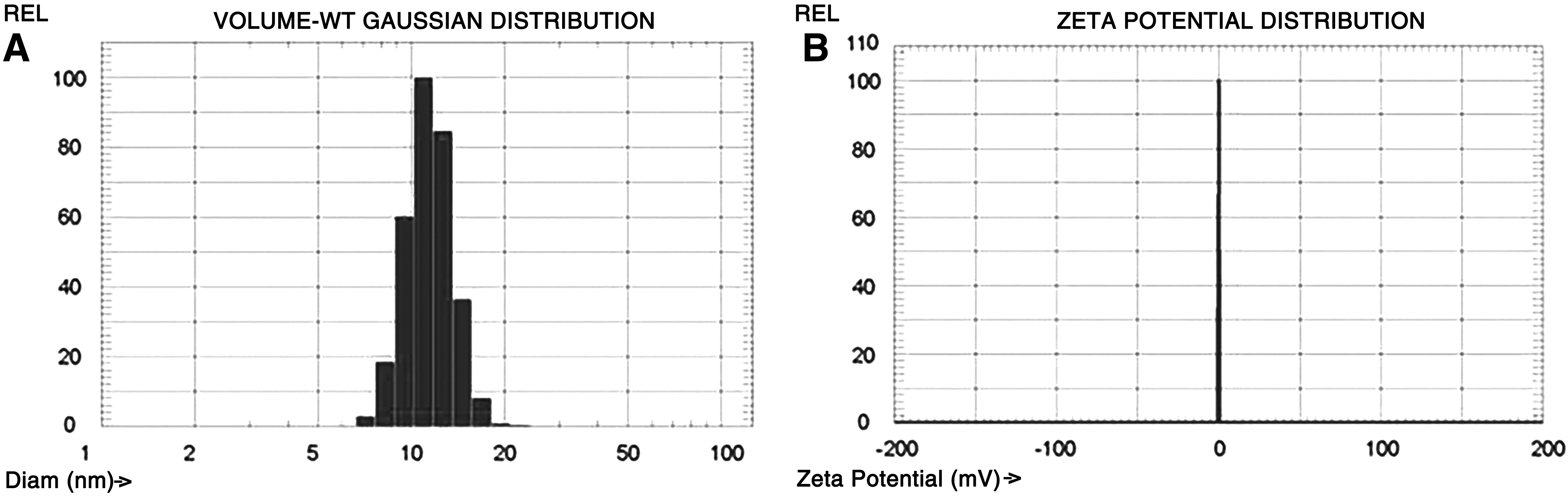
Droplet size and zeta potential analysis
In o/w microemulsions, droplet size refers to the size of dispersed oil droplets in a continuous water phase. The average droplet diameter of the undiluted blank and drug-loaded microemulsion was found to be 9.33 ± 0.04 nm and 11.4 ± 0 nm, respectively. The zeta potential of the blank and drug-loaded microemulsions was found to be neutral. Representative images are shown in Figs. 2 and 3, respectively.
pH and clarity
The pH is of major importance, as it indicates the stability of most drugs and to avoid irritation to the eye. 30 An unbuffered solution with a pH ranging from 4 to 8 is suitable for ocular use. On administration, the pH of these solutions is modulated by the buffering capacity of tear fluids to the physiological range. 31 The pH values of the blank and drug-loaded formulation were found to be 6.87 ± 0.07 and 6.91 ± 0.03, respectively. The clarity of the microemulsion was studied to confirm the ability of light transmission through the formulation. Blank and drug-loaded microemulsions were found to be clear, with transmittance values of 98.4 ± 0.48 and 98.5 ± 0.47, respectively.
Differential scanning calorimetry
DSC thermograms of pure dexamethasone, tobramycin, blank microemulsion, and drug-loaded microemulsion are shown in Fig. 4. Dexamethasone exhibited a sharp endothermic peak at an onset temperature of 267.70°C, with a peak temperature of 271.93°C, which corresponds to the melting point of dexamethasone. 32 The thermogram confirmed the typical crystalline nature of dexamethasone. The thermogram of tobramycin showed 3 events: an endothermic peak of anhydrous metastable form of tobramycin at an onset temperature of 173.41°C, with a peak temperature of 183.30°C, which corresponds to the melting point of tobramycin; an exothermic peak followed by a sharp endothermic peak at 224.39°C. These events correspond to the crystallization and melting of stable form of tobramycin. 33 Blank and drug-loaded microemulsions exhibited a sharp endothermic peak at an onset temperature of 97.39°C and 100.19°C, respectively. These correspond to evaporation and loss of water from the samples. 34

Differential scanning calorimetry thermograms of (A) dexamethasone, (B) tobramycin, (C) blank microemulsion, and (D) drug-loaded microemulsion.
TEM of microemulsion
TEM images of blank and drug-loaded microemulsions are shown in Fig. 5. The observed droplets were spherical in shape, and the droplet size in both cases was found to be slightly higher than the values obtained using DLS.

Transmission electron microscopy images of
HPLC analysis of dexamethasone
A quantitative method for the estimation of dexamethasone using HPLC was successfully developed and validated. The method was validated by determining accuracy, precision, limit of detection (LOD), and limit of quantification (LOQ). The chromatogram of dexamethasone presented a sharp peak with a retention time of 2.9 min. A linear calibration curve (y = 2038.4x − 447.94) was obtained, with a regression coefficient (R 2 ) of 1. LOD and LOQ were calculated according to ICH Q2(R1) guidelines 35 and were found to be 0.53 and 1.61 ng, respectively. The percentage recovery of dexamethasone ranged from 97.13% to 100.24%. The method also showed good interday precision and suitability with a relative standard deviation (RSD) of <2%.
UV analysis of tobramycin
A quantitative method for the estimation of tobramycin using UV spectrophotometer was successfully developed and validated. A linear calibration curve (y = 0.0027x + 0.0138) was obtained in the concentration range of 50–250 μg/mL, with a regression coefficient (R 2 ) of 0.9993. LOD and LOQ were found to be 2.26 and 6.85 μg/mL, respectively. The percentage recovery of tobramycin ranged from 96.44% to 103.01%. The method also showed good interday precision and suitability with RSD of <2%.
Validation of sterility
Except for the positive control, all the test tubes remained clear and did not show any signs of bacterial growth. The same was observed with the plate inoculation method (Table 4). The clear positive sample control could be attributed to the presence of BAK in the formulation. 36
In vitro drug release study
The in vitro release pattern of dexamethasone from the microemulsion is shown in Fig. 6. The release pattern was obtained by plotting the percentage of cumulative drug release versus time. Initially, a burst release was observed in the first 30 min during which nearly 35% of the drug was released. Later on, the drug release was slow and continuous and complete drug was released over a period of 8 h. This suggests that the oil phase of microemulsion serves as a reservoir, and the drug transport occurs primarily from the water phase. 37 No visual change was observed on incubation with the phosphate-buffered saline (pH 7.4) containing 0.025% (w/v) Tween 80, indicating the stability of drug-loaded microemulsion in the presence of the release medium.
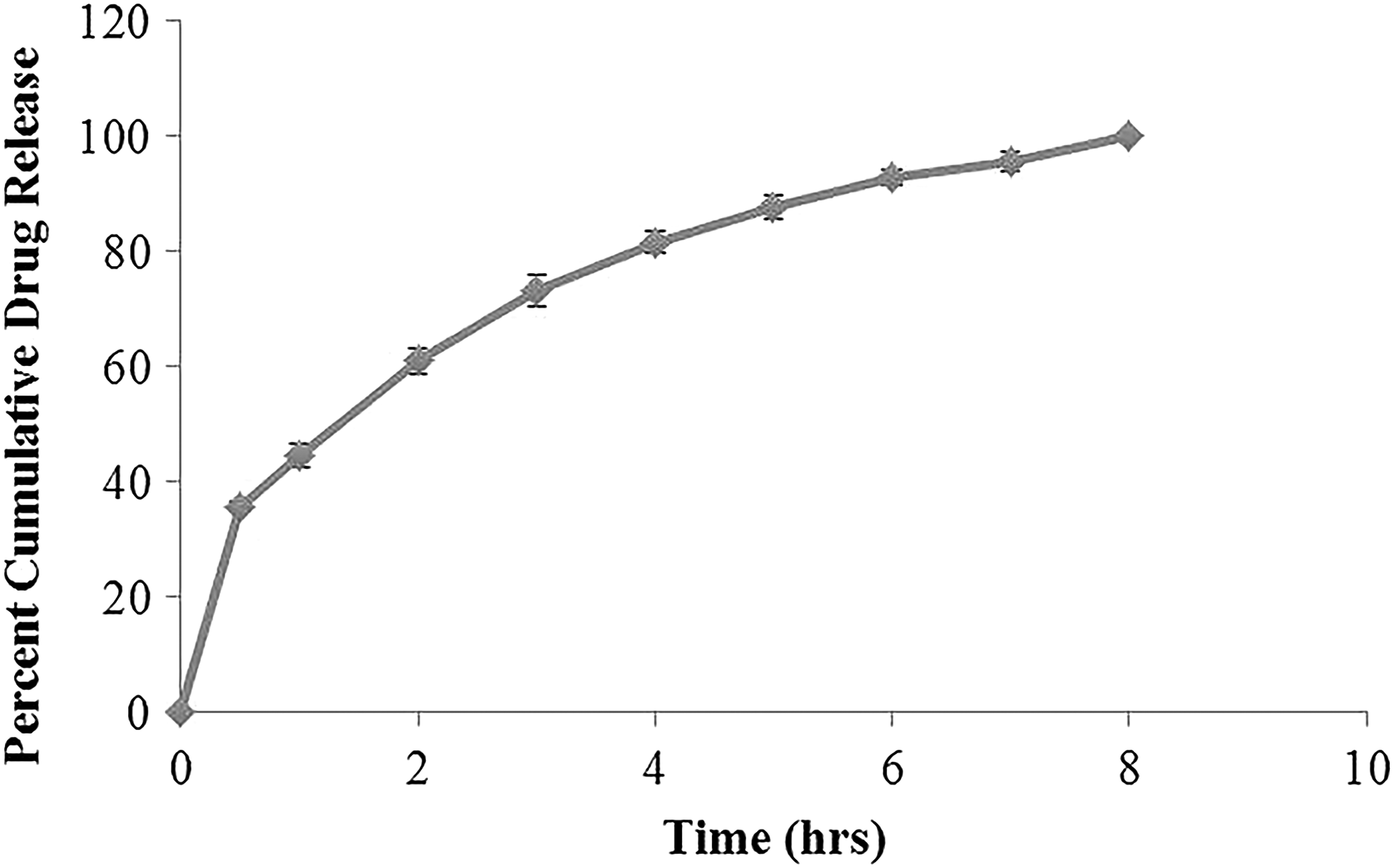
In vitro drug release of dexamethasone from microemulsion (n = 3). Values are represented as mean ± SD. Error bars represent SD. SD, standard deviation.
Cytotoxicity study
The cytotoxicity of the microemulsion was compared with the Tobradex suspension using bovine corneal endothelial cells, as shown in Fig. 7. The percentage of cell viability in the presence of 20% DMSO was 10.88%. With both formulations, the cell viability was >100% at lower concentrations (0.01%, 0.1%, 1%, and 5%), whereas the cell viability was <15% at higher concentrations (50% and 100%).

Cell viability of bovine corneal endothelial cells treated with microemulsion and marketed suspension (n = 5). *P < 0.05. Error bars represent SD.
Anti-inflammatory study
The anti-inflammatory activity of the microemulsion and Tobradex suspension determined using Griess assay is shown in Fig. 8. The amount of nitrite ions produced by microglial cells treated with different concentrations (0.001%, 0.01%, and 0.1%) of microemulsion was lower than that produced by suspension- treated cells. Moreover, the anti-inflammatory activity demonstrated by the drug-loaded microemulsion was significantly (P < 0.05) higher than that of the Tobradex suspension at 0.1% concentration.

Griess assay using microglial cells activated with LPS (n = 3). Negative control (cells without LPS treatment) and positive control (cells with LPS treatment). *P < 0.05. Error bars represent SD. LPS, lipopolysaccharides.
Antimicrobial disk diffusion susceptibility test
The antimicrobial activities of the microemulsion and Tobradex suspension (n = 9) are shown in Table 5 and Fig. 9. The average zone of inhibition observed with the standard tobramycin disc was 21.8 ± 0.03 mm. The drug-loaded formulation exhibited a higher zone of inhibition (29.33 ± 0.06 mm) compared to the Tobradex suspension (27.4 ± 0.04 mm). Moreover, the antibacterial activity demonstrated by the microemulsion was significantly higher (P < 0.05) than that of the Tobradex suspension.
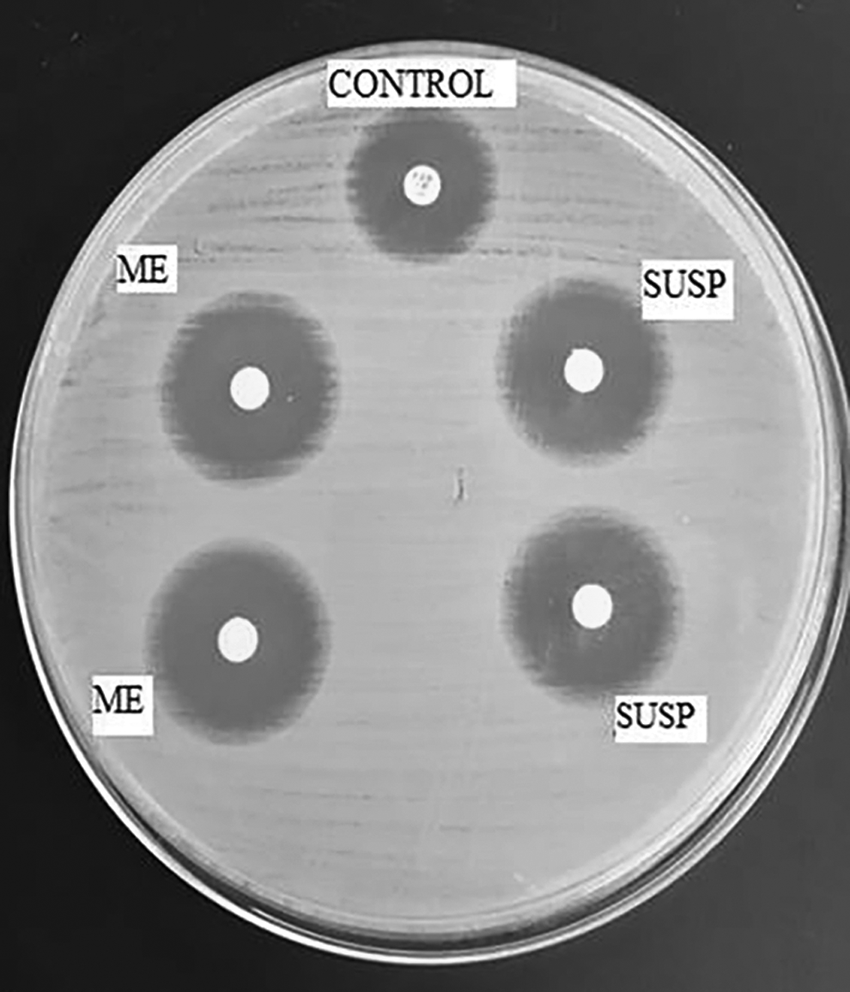
Zone of inhibition produced by the developed microemulsion (ME), Tobradex® suspension (SUSP), and standard tobramycin 10 μg disk (control) (n = 9). *P < 0.05.
P < 0.05.
SD, standard deviation.
Histological evaluation in bovine cornea
Images of bovine corneas treated with microemulsion and Tobradex suspension are shown in Fig. 10A and B, respectively. Microscopic evaluation showed no signs of toxicity with intact corneal epithelium in both cases. This confirms the safety of the prepared microemulsion for ocular administration.
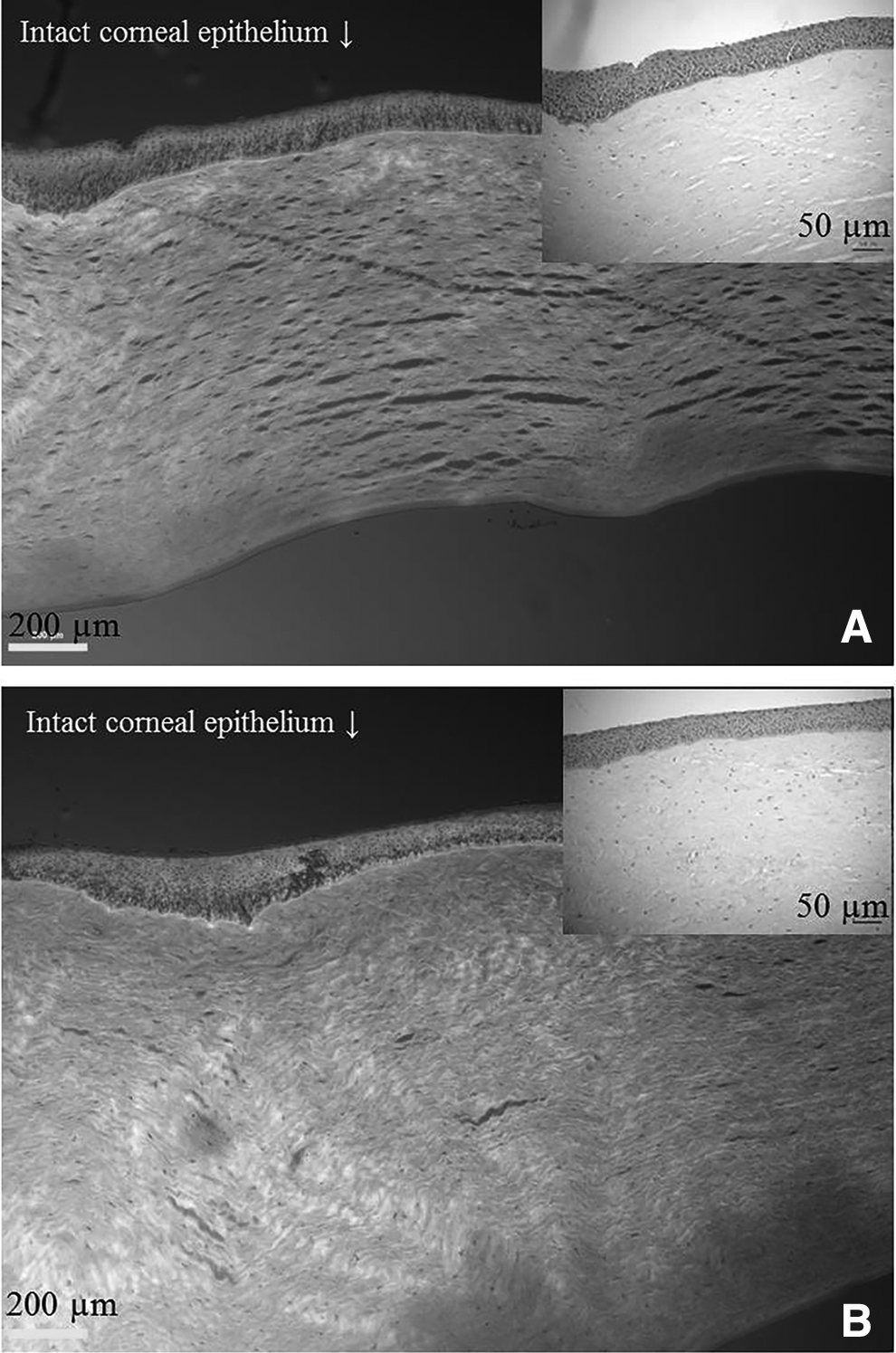
Representative micrographs of hematoxylin/eosin-stained bovine cornea treated with
Stability study
Microemulsion showed good stability when stored at 4°C and 25°C. The results of the study are shown in Table 6. At 40°C, the formulation was not stable over the testing period, with respect to drug content and clarity (data not shown). No significant change was observed with the samples tested over a period of 3 months.
Values represented as mean ± standard deviation.
Discussion
We have successfully formulated a microemulsion of dexamethasone and tobramycin using ricinoleic acid (2.5%), cremophor EL (9.3%), 1-butanol (6.2%), and distilled deionized water (82%) by spontaneous emulsification method. Ricinoleic acid is a naturally occurring, unsaturated omega-9 fatty acid and is obtained from mature castor plants. About 90% of the total fatty acid content in castor oil is from ricinoleic acid and is used as one of the lipophilic vehicles in cyclosporine eye drops. 38 Ricinoleic acid is known for its analgesic, anti-inflammatory, and antibacterial activities on acute or repeated local application.22,39,40 Hence, we selected ricinoleic acid for the oil phase. Cremophor EL and 1-butanol were chosen as the surfactant and cosurfactant, respectively, which are nonionic by nature. Generally, nonionic surfactants cause less irritation to the eye compared to cationic and anionic agents. 41 Cremophor EL is widely used as surfactant in commercial ophthalmic formulations and is shown to be nonirritating and nontoxic to the eye. 42 Even though 1-butanol is not a generally recognized as safe excipient, it has been extensively studied for its use in the preparation of microemulsions.43–45 Recently, Ince et al. investigated the potential of an ocular microemulsion of pilocarpine using soybean oil, Span 80, Brij 35P, 1-butanol, and water. The results of the ocular tolerance and histology studies in rabbits revealed that the formulation was nonirritant, with no signs of toxicity. 46 Hence, we selected 1-butanol as a cosurfactant for the study.
The formulated ocular microemulsion of dexamethasone and tobramycin was evaluated for pH, particle size, zeta potential, light transmittance/clarity, morphology, drug content, sterility, in vitro drug release, and stability. The pH values of the blank and drug-loaded formulation were found to be 6.87 ± 0.07 and 6.91 ± 0.03, respectively. These values are close to the physiological range, suggesting the suitability of the microemulsion for ophthalmic use. 31 Ocular preparations should exhibit more than 90% transmittance or absorbance <0.1 at 400 nm. 47 Blank and drug-loaded microemulsions were clear, with light transmittance around 95%–100%. Microemulsions with such clarity can address the problem of transient blurring of vision associated with the marketed eye drop suspension.
Droplet size of a microemulsion plays a significant role in predicting the rate and extent of drug absorption. 48 The average droplet diameters of the undiluted blank and drug-loaded microemulsion were found to be 9.33 ± 0.04 nm and 11.4 ± 0 nm, respectively. The small size of the droplets could be due to the presence of cosurfactant molecules that penetrate into the interfacial film and lower the fluidity and surface viscosity, eventually decreasing the radius of curvature. 49 Also, the slight increase in the droplet size of the drug-loaded microemulsion versus that of the blank microemulsion could be attributed to the incorporation of dexamethasone molecules within the core.
The zeta potential of blank and drug-loaded microemulsion was found to be neutral, and this could be attributed to the nonionic nature of the surfactants used in the preparation. DSC was performed to confirm the absence of any undissolved drugs in the microemulsion. The characteristic endothermic peaks of dexamethasone and tobramycin were completely absent in the microemulsion, indicating that these drugs were either converted to an amorphous form or were molecularly dispersed in the formulation. 26 The morphology of the microemulsion was studied using TEM. The images revealed the presence of slightly larger droplets than that observed with DLS. This could be due to the different experimental conditions used in DLS and TEM. In TEM, the oil droplets spread onto the surface of the grids, and this process is facilitated by low interfacial tension, which further results in coalescence and the formation of larger structures, as evident from the images. 50
Sterility is an important parameter of ophthalmic products. In the present study, the microemulsion was sterilized by passing through a Millex sterile nylon syringe filter (0.22 μm). Later, the sterility of the microemulsion was validated according to United States Pharmacopeia guidelines by direct as well as plate inoculation methods. Except for the positive control, remaining plates/tubes tested were found to be clear, with no signs of bacterial growth. The reason for a clear positive sample control (plate/tube) could be due to the activity of BAK against gram-positive bacteria, such as Staphylococcus aureus, used in the study. 51 The prepared microemulsion remained sterile for 14 days, and the test also confirmed that aseptic filtration is sufficient for the sterilization of microemulsions. The in vitro release pattern of dexamethasone was studied by the dialysis bag method. The developed microemulsion showed a complete release of dexamethasone over a period of 8 h in a sustained manner. The cytotoxicity of the microemulsion was compared with that of the Tobradex suspension using MTT assay. Lower concentrations (0.01%, 0.1%, 1%, 5%) did not show any cytotoxicity and resulted in cell proliferation, whereas higher concentrations (50% and 100%) were toxic with both formulations. Literature findings suggest that dexamethasone shows a dose-dependent effect on epithelial cell proliferation at low concentrations and inhibition at high concentrations. 52 Our study result aligns with the literature findings. As the drug delivery to the anterior segment of the eye is limited by several physiological constraints and anatomical barriers, <5%–10% of the instilled dose actually reaches the ocular tissues. 16 Therefore, it is highly unlikely that these higher concentrations of 50% and 100% reach the ocular tissues and cause any in vivo toxic effects.
Microglial cells activated with LPS were used to compare the anti-inflammatory activities of the microemulsion and Tobradex suspension by Griess assay. The inflammation induced by LPS was reduced by dexamethasone in the formulation. Griess assay was carried out to detect the presence of nitrite compounds. Nitric oxide is an important signaling molecule in the pathogenesis of inflammation. Under abnormal physiological conditions, overgeneration of nitric oxide acts as a proinflammatory mediator that induces inflammation. Nitric oxide is metabolized (oxidization) to a stable, nonvolatile nitrite anion. The assay is based on the diazotization reaction between the nitrites present in the sample and the sulfanilic acid present in the Griess reagent. The resultant diazonium salt formed reacts with the azo dye agent (naphthylethylenediamine dihydrochloride), resulting in a pink color. The amount of nitrite present was estimated based on the intensity of pink color using a microplate reader. As determined from the nitrite ions produced by the microglial cells, the anti-inflammatory activity exhibited by the drug-loaded microemulsion was significantly higher (P < 0.05) than that of the Tobradex suspension at 0.1% concentration. This could be due to the synergistic anti-inflammatory effects of dexamethasone and ricinoleic acid, combined with the improved dose uniformity of the microemulsion. Similar results were also reported by Kesavan et al. Dexamethasone-loaded microemulsion was prepared using isopropyl myristate, Tween 80, propylene glycol, and distilled water and was further coated with chitosan so as to increase the mucoadhesive properties. In vivo studies revealed a marked improvement in the anti-inflammatory effect in microemulsion-treated eye when compared to the marketed suspension in uveitis-induced rabbits. 53
The Kirby-Bauer disk susceptibility test was performed to compare the antimicrobial efficacy of tobramycin in the microemulsion and Tobradex suspension using E. coli. The test measures the sensitivity or resistance of microorganisms to antibiotics on MH agar media using antibiotic-impregnated discs. The absence of growth surrounding the discs reveals the ability of an antibiotic to kill the particular microorganism. In our study, we observed that tobramycin loaded in the microemulsion showed higher antimicrobial efficacy (P < 0.05) than the Tobradex suspension. This could be due to the synergistic antibacterial activity of tobramycin and ricinoleic acid present in the formulation. The presence of 1-butanol and the dose uniformity of the developed formulation could also contribute toward the enhanced antibacterial activity. Histological evaluation of bovine corneas treated with the microemulsion and Tobradex suspension showed intact corneal epithelium with no signs of toxicity. Also, the prepared dexamethasone- and tobramycin-loaded microemulsion was found to be stable at 4°C and 25°C for 3 months.
A similar ocular microemulsion was prepared by Fialho and da Silva-Cunha using dexamethasone, cremophor EL, propylene glycol, isopropyl myristate, BAK, and distilled water. The prepared microemulsion was nonirritant, stable, and showed good acceptable physiochemical properties. The formulation demonstrated greater permeation into the anterior segment of the eye and sustained release over a longer period of time than the conventional suspension preparation. Also, the pharmacokinetic studies revealed that area under the curve was 2 times higher with microemulsion than the suspension. 54
Conclusion
In this study, we report the development and evaluation of an ocular microemulsion of dexamethasone and tobramycin for treating anterior segment eye infections. Both the blank and drug-loaded microemulsions displayed a droplet size of <20 nm by DLS and a neutral zeta potential. The pH of microemulsions was close to physiological range, with light transmittance around 95%–100%. The microemulsion was successfully sterilized using a 0.22 μm filter. The cytotoxicity study in bovine corneal endothelial cells showed no signs of toxicity at lower concentrations (0.01%–5%) when compared to the control. The anti-inflammatory study in microglial cells showed that the activity was significantly greater with microemulsion than with the Tobradex suspension at 0.1% concentration. The antibacterial study revealed that the microemulsion had significantly higher efficacy when compared to the marketed suspension. Stability studies indicated that the formulation was stable at 4°C and 25°C for 3 months. In conclusion, an o/w microemulsion of dexamethasone and tobramycin was successfully prepared using ricinoleic acid, cremophor EL, 1-butanol, and water. This formulation could be explored as a suitable alternative to the Tobradex suspension. Long-term stability and efficacy of the formulation in an animal model should be established.
Footnotes
Acknowledgments
The authors acknowledge Drs. Zahoor Shah and Rose Jung for providing the microglial cells and E. coli strain, respectively. This work was supported by start-up funds from The University of Toledo and a grant from the deArce Memorial Endowment Fund in support of medically related research.
Author Disclosure Statement
No competing financial interests exist.