
Abstract
Abstract
Purpose:
To evaluate the long-term effects of intravitreal dexamethasone implants (IDIs) in eyes with macular edema (ME) due to retinal vein occlusion (RVO).
Methods:
We reviewed the records of 10 patients followed for 5 years after they received their first IDI. The main outcome measures included changes in best corrected visual acuity (BCVA), central macular thickness (CMT), and central macular volume (CMV), and the incidence of side effects.
Results:
Ten patients were included in the study with a mean follow-up of 65.51 months. Forty IDI injections were performed. An improvement in BCVA was observed after 92.5% of the IDI injections (P < 0.05), while the CMT and the CMV decreased significantly (P < 0.05) after 97.5% of the injections. After 27.5% of the injections, the intraocular pressure rose more than 10 mmHg and 3 of the 7 phakic patients required phacoemulsification surgery.
Conclusion:
IDI is an effective therapy for the treatment of ME secondary to RVO with a favorable long-term safety profile.
Introduction
R
The treatment options available for ME secondary to RVO include laser photocoagulation when associated with BRVO, and intravitreal corticosteroid therapy, intravitreal treatment with antivascular endothelial growth factor (anti-VEGF) agents and pars plana vitrectomy with peeling of the internal limiting membrane for both BRVO and CRVO. 5 Clinical studies and data from clinical practice have shown that repeated treatments are often required to control ME and prevent the loss of vision, as well as to increase the chance of visual improvement. 5
The intravitreal dexamethasone implant (0.7 mg, IDI, Ozurdex; Allergan, Inc., CA) is a biodegradable, sustained-release drug delivery system that secretes low doses of dexamethasone into the vitreous cavity over a period of 6 months. 6 In Spain, Ozurdex received approval in 2010 for the treatment of adult patients with ME following BRVO or CRVO based on the conclusions of the GENEVA study, 7 in 2011 for the treatment of noninfectious posterior uveitis, based on the results of the HURON study, 8 and, in 2014, for the treatment of patients with visual impairment due to diabetic macular edema who are pseudophakic or who are considered insufficiently responsive to and/or unsuitable for noncorticosteroid therapy, based on the results of the MEAD study. 9
The GENEVA study demonstrated the efficacy and safety of IDI delivery to the vitreous cavity to treat ME due to either BRVO or CRVO. A single IDI treatment produced significant improvements in best corrected visual acuity (BCVA) as early as 30 days post-treatment, and in many eyes this improvement was sustained for as long as 6 months. 7 Single and repeated IDIs were well tolerated over a 12-month period, although the progression of cataracts was accelerated.7–10
The data available regarding the long-term effects of IDIs in patients with RVO-associated ME, who have been administered multiple injections over several years, are limited. Most of the studies available have focused on the effects of IDIs over shorter periods of time, and usually over 6 months. There are some data available on patients with RVO-associated ME who received between 1 and 3 IDI injections over a 12-month period.10,11 Elsewhere, a mean of 2.6 injections were administered over 2 years 12 and the largest number of injections administered to date were reported in the SHASTA study, patients receiving 2 to 9 injections to treat RVO-associated ME.13–15 Moisseiev et al. 16 reported the first long-term evaluation (50.5 months) of patients treated with Ozurdex with a favorable long-term safety profile and a beneficial effect on the visual prognosis in BRVO. To the best of our knowledge, the present study is the first to assess the efficacy and safety of IDI use in patients with RVO-associated ME with a follow-up of 5 years.
Methods
A retrospective, single-center study was carried out on patients with ME secondary to RVO who attended the Hospital Universitario Araba (Spain). After a retrospective review of their medical records, a total of 16 patients were identified who had been treated with IDIs on an “as-needed” basis between May 2010 and November 2017, and who had been followed for at least 60 months after receiving the first implant. The inclusion criteria used were as follows: patients at least 18 years of age; diagnosed with ME secondary to CRVO or BRVO; with Snellen BCVA at baseline less than 20/40; who have been followed for at least 60 months after the first implant; with a central macular thickness (CMT) >350 μm at baseline, measured by spectral domain-optical coherence tomography (SD-OCT); and with a central macular volume (CMV) >9 mm3 measured by SD-OCT. Patients who had undergone prior vitrectomy or glaucoma surgery, patients who required anti-VEGF intravitreal injection after IDI treatment, and patients with a follow-up period less than 60 months after the first implant were excluded. Thereafter, 6 patients were excluded. Previous treatments to decrease ME were tolerated. Laser treatment was permitted during the follow-up period at the discretion of the investigator. The study was approved by the Bioethical Committee of the Hospital Universitario Araba and informed consent was obtained from all the patients included in the study in accordance with the principles of the Helsinki Declaration for medical research involving human subjects.
Data were retrieved by retrospective review of the patients' medical records. Among the parameters considered at the baseline (before the first injection) were demographic information, ocular history, type of RVO, previous treatments for RVO-associated ME, associated pathologies, BCVA, intraocular pressure (IOP), CMT, CMV, ME duration, and lens status. After IDI injection, the patients were followed for a period of at least 60 months, during which the efficacy and safety of the IDI treatment were evaluated.
Outcome measures included the following: the mean change in BCVA, CMT, and CMV from the baseline to the last follow-up visit and from before each injection to the day demonstrating the greatest improvement after each injection; the proportion of patients with at least a 3-line improvement of BCVA; and the retreatment interval between each injection. For the safety analysis, ocular hypertension, cataract surgery, endophthalmitis, retinal detachment, and vitreal hemorrhage were evaluated. 17 Cataract progression was assessed using the Lens Opacities Classification System (LOCS) III and with Scheimpflug images. 18
ME resolution was considered to have been resolved if the IDI was permanently discontinued for at least 6 months after the last injection. 17
Descriptive parameters were used to describe the characteristics of the sample (eg, sex and age,), using measures of central tendency and dispersion (eg, mean values, ranges, standard deviations). Changes in BCVA (converted to the logarithm of the minimum angle of resolution—logMAR) between baseline and at each follow-up visit and between baseline and at the last follow-up visit were compared using Wilcoxon test and IOP, and CMT and central macular volume (CMV) at baseline and at each follow-up visit were compared using a paired t-test using version 23 of the SPSS statistical analysis package (IBM Corp., Armonk, NY).
Results
Baseline demographic and patient characteristics
A total of 10 patients satisfied the inclusion criteria for the study, and their demographic and baseline characteristics are presented in Table 1. The patients' mean age was 58 years (range 36–77) and 6 patients (60%) were male. Of the 10 patients, 6 were diagnosed with BRVO and 4 with CRVO. None of the patients presented ischemia at the baseline measured by fluorescein angiography. The mean duration of RVO-associated ME before the first IDI was 373.8 days (83–1,007 days), and it was >90 days in 9 of the 10 patients. Seven patients had previously received treatment to manage their ME and of these, 2 patients had been treated with ranibizumab and pegaptanib, 2 patients with intravitreal triamcinolone, 1 patient with ranibizumab, and 2 patients with bevacizumab and laser treatment. Only 1 of the patients had a documented history of elevated IOP in response to steroid treatment. All patients had an IOP <22 mmHg at baseline, including the patient with pre-existing glaucoma, and while 7 patients were phakic, 3 had undergone prior cataract surgery.
BRVO, branch retinal vein occlusion; CMT, central macular thickness; CMV, central macular volume; CRVO, central retinal vein occlusion; F, female; IOP, intraocular pressure; LE, left eye; M, male; ME, macular edema; OHT, ocular hypertension; RE, right eye; VA, visual acuity.
Treatment
A total of 40 IDI injections were administered to the patients during the period of the study, with the patients receiving between 1 and 10 implants. An average of 4 injections per patient were given during the follow-up period, and 60% of patients received 3 or more IDIs. Three patients (30%) required only 1 implant to manage their condition, 2 patients required 3 injections, while each of the remaining patients (10%) required 2, 5, 6, 8, or 10 injections, respectively. The mean interval between the IDI injections was 286.8 days (range 141–1,216 days), and the mean time from the last injection was 1,073.1 days (range 84–2,052) days. All patients were followed up for at least 60 months (mean: 65.5; range: 60.7–68.3) and only 1 patient was still being actively treated at the end of the study (until December 2017 he had received 16 IDI injections).
Efficacy analysis
The mean baseline BCVA before injection was 0.61 (±0.27) logMAR, which improved to 0.34 (±0.24) logMAR (P < 0.05) after the injections (Table 2). The BCVA improved after 37 of the 40 IDI injections (92.5%) and this improvement was ≥3 Snellen lines after 19 of the 40 IDI injections (47.5%). At the last follow-up visit, 9 patients displayed an improvement in the BCVA from the baseline values from 0.58 (±0.27) logMAR to 0.22 (±0.17) logMAR (P < 0.005), with a mean improvement of 3.3 Snellen lines. Moreover, 4 patients had an improvement in BCVA relative to the baseline ≥3 Snellen lines.
BCVA, best corrected visual acuity; CMT, central macular thickness; CMV, central macular volume; IOP, intraocular pressure; logMAR, logarithm of the minimum angle of resolution.
After all but 1 of the 40 injections, a decrease in the CMT was evident relative to the previous value (P < 0.05), decreasing from 481 (±156.8) μm to 249.1 (±66.4) μm and with a mean decrease of 217.5 μm. At the last follow-up visit, the CMT had improved in 9 patients relative to the baseline (P < 0.05) (Fig. 1). The mean CMV improved relative to the baseline (P < 0.05) after each of the 40 IDIs, decreasing from 11.7 (±1.9) mm3 to 9.4 (±1.5) mm3, with a mean decrease of 2.2 mm. 3 At the last follow-up visit, the CRV had improved relative to the baseline in all patients (P < 0.05).
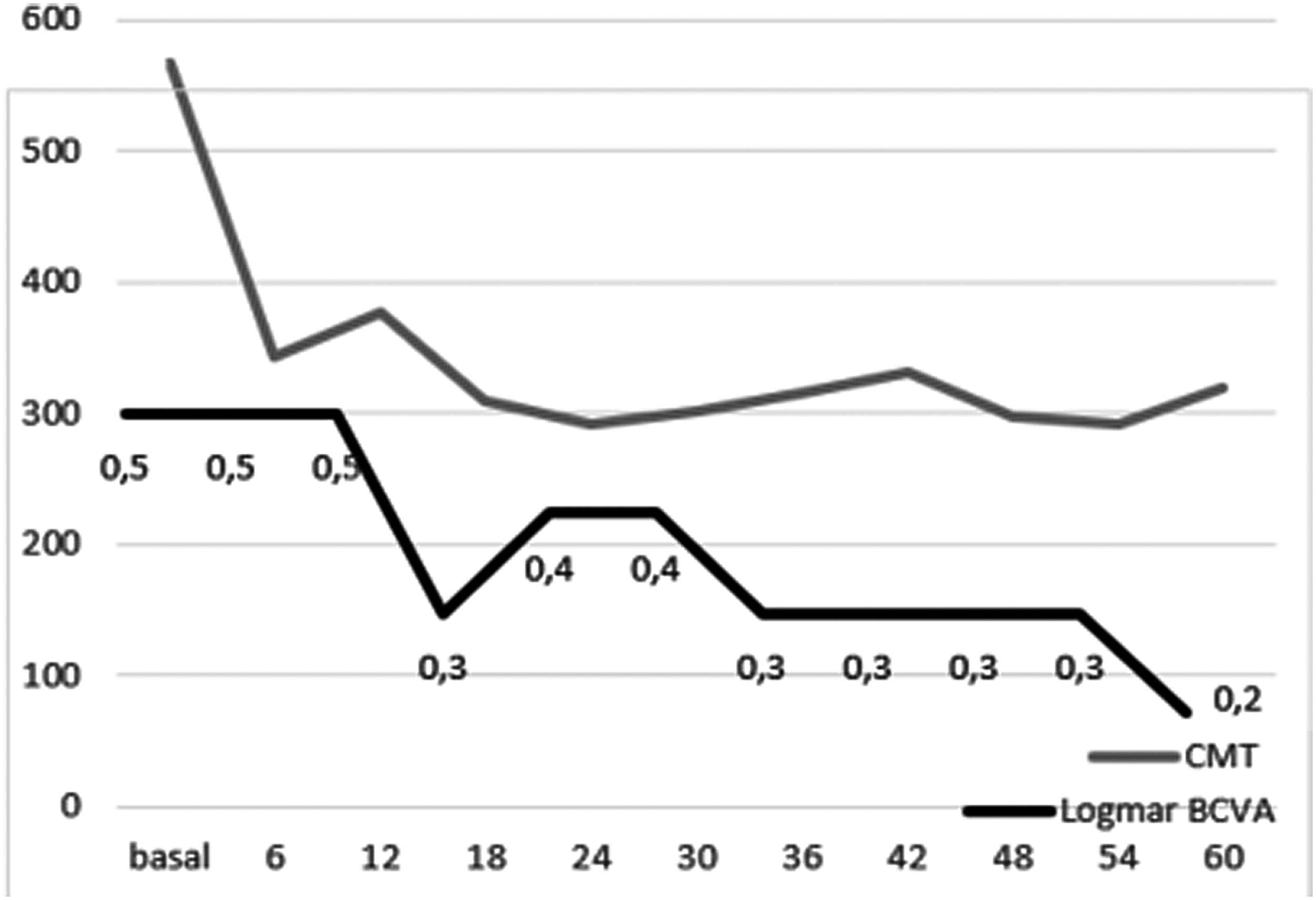
Mean values of CMT and BCVA in logMAR scale during the 60 months of follow-up. BCVA, best corrected visual acuity; CMT, central macular thickness; logMAR, logarithm of the minimum angle of resolution.
During the follow-up, the treating physician decided to perform grid laser treatment on 2 eyes, and neither posterior nor anterior segment neovascularization developed in any studied patient.
Safety analysis
Among the 7 patients with phakic eyes at baseline, 3 (42.85%) underwent cataract surgery during the study period. The baseline opacity was LOCS III grade 1 in 2 patients and progressed to a posterior subcapsular grade 4 (Fig. 2), while opacity of the eye of the third patient was grade 3 and progressed to grade 4. The mean age of these patients was 55.3 years. Cataract surgery was performed after the third IDI injection in 1 patient and after the fifth IDI injection in the other 2 patients. All these surgical interventions were performed without any complications.
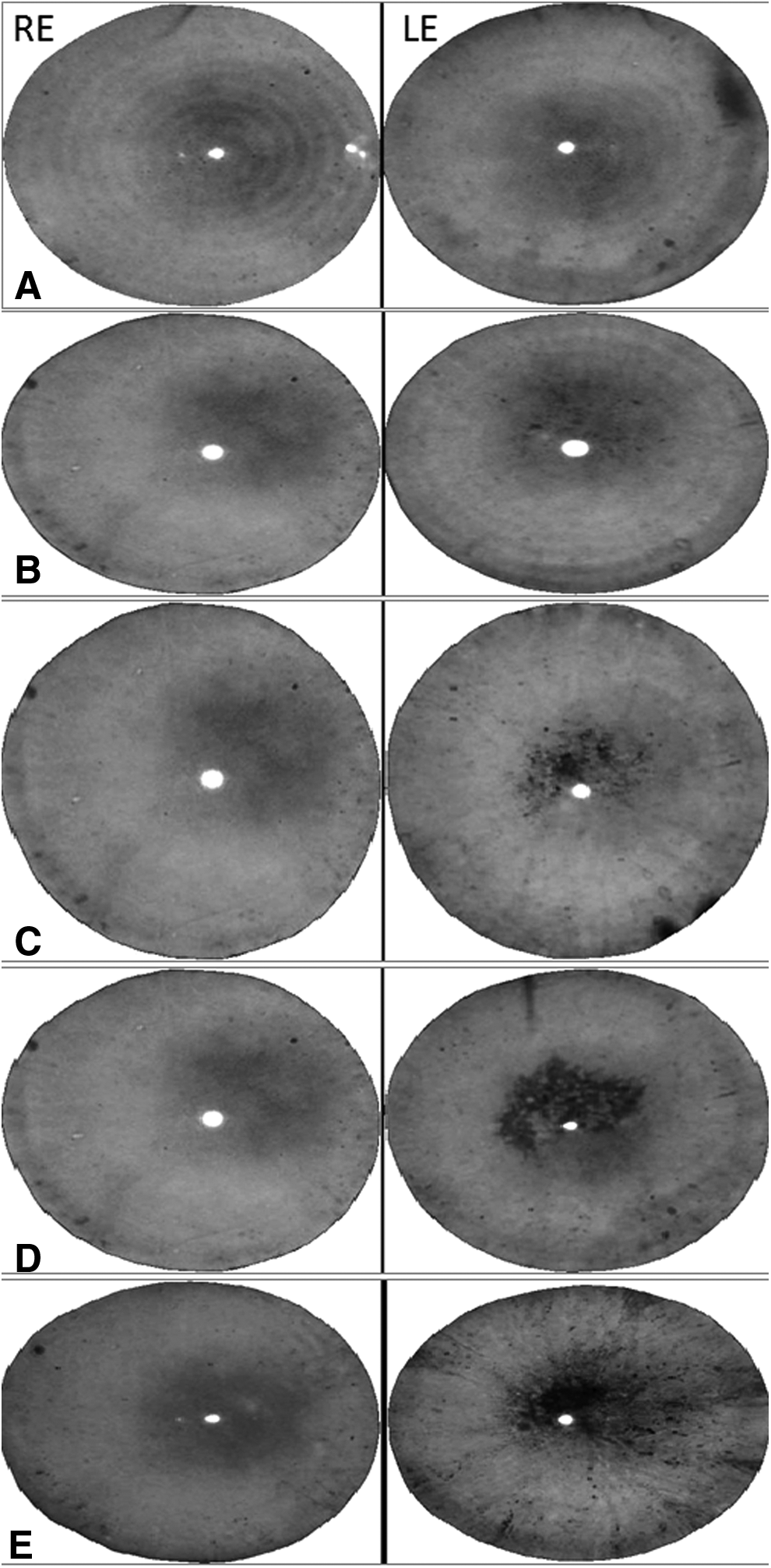
Left eye posterior subcapsular cataract development. Images captured before each injection being right eye the control eye.
The second most common adverse event (AE) associated with IDI injection was an increase in IOP. At baseline, all patients had an IOP <21 mmHg, although 1 patient was being treated with topical antihypertensive drugs. Before injection, the mean baseline IOP was 16.96 ± 2.76 mmHg and it rose to 24.25 (±6.5) logMAR (P < 0.05) after the injections (Table 3). After 11 of the 40 IDI injections (27.5%), the mean IOP had increased ≥10 mmHg from the baseline, and after 14 of the 40 IDI injections, the mean IOP was higher than 25 mmHg. In 2 patients, the IOP exceeded 35 mmHg, although this increase was controlled with topical treatment. As a consequence of this elevation, 6 of the 10 patients used IOP-lowering medication; a treatment that restricted the increase in IOP from the baseline to the last visit to less than 10 mmHg in all 10 patients. At the last follow-up visit, 4 patients were using IOP-lowering medication. No patients required laser treatment or incisional glaucoma surgery during the study period.
IOP, intraocular pressure.
Finally, 1 patient underwent pars plana vitrectomy for epiretinal membrane progression, whereas none of the patient's suffered severe ocular (eg, endophthalmitis, retinal detachment, and vitreous hemorrhage) or systemic AEs during the follow-up period.
Discussion
This retrospective study focused on the long-term response to IDI therapy of a small cohort of patients with RVO-associated ME in a clinical setting in Spain. These patients represent the cohort that has been followed for the longest time reported to date, confirming the efficacy and tolerability of this treatment over a follow-up period of at least 5 years. After 92.5% of the IDI injections, an improvement in VA was observed and in 90% of patients the BCVA improved relative to the baseline. The CMT also improved in 9 patients at the last follow-up visit and all the injections improved the CMV, which was better than at the baseline. Thus, IDIs appear to represent an effective treatment for ME secondary to RVO, even though reinjection was required every 8 months. Indeed, this treatment seemed to be effective even though ME was chronic in 90% of patients and that 80% of patients had received prior treatments to treat complications related to RVOs.
IDI therapy was well tolerated in our cohort of RVO-ME patients, and all AEs were predictable and manageable. The most common AEs were high IOP and cataract progression, consistent with the safety profile previously established for IDI injections.6,10–15,17 Indeed, while 35% of the injections provoked high IOP, this was controlled with topical antihypertensive drugs. However, 42.85% of the phakic patients required cataract surgery, which we believe is due to the long follow-up and to the high mean number of injections. These 2 reasons we believe explain why cataract development becomes the most common AE.
Moisseiev et al. 16 reported the first long-term evaluation of patients treated with Ozurdex indicating a favorable long-term safety profile and a beneficial effect on the visual prognosis in BRVO. However, they allowed additional treatment administration, so that 7 of their 17 patients were treated with bevacizumab injections. Their long-term results may be conditioned by this additional drug. However, during the follow-up period of our study, the use of any other drug is not allowed.
Our study has some limitations and, in addition to the fact that it is a retrospective and observational study, the main weakness of this study is the small sample size. Moreover, there was no standardization of patient evaluations, and a detailed comparison of the data obtained with that from previous clinical trials and retrospective studies was complicated by the fact that they involve different patient groups. This is particularly true regarding the type and length of the prior treatments, and the intervals between the IDI injections.
Despite the relatively small study population and the absence of detailed comparisons, the results of the present study do indicate that IDI treatment is likely to be a safe and effective long-term therapy for RVO-associated ME.
In conclusion, treatment with IDI for ME secondary to RVO is an effective therapy for such long-term treatment and it has a favorable safety profile similar to that observed in studies that have focused on shorter follow-up periods.
Footnotes
Acknowledgments
The authors would like to thank BiomedRed S.L. for the drafting of the document and editorial support, funded by Allergan plc. (Irvine, CA) and Arantza Saezdelafuente-Moriñigo, from the Statistical Department of the Hospital Universitario Araba, for the statistical analysis.
Author Disclosure Statement
None of the authors has conflict of interest with this submission. This study was partially presented at the XXI Congress of the Sociedad Española de Retina y Vitreo in March 2017 held in Madrid.