
Abstract
Purpose:
To evaluate the efficacy of adiponectin (APN)-derived short peptides (ADPs) 355 compared with globular APN in a mouse model of experimental dry eye (EDE) and corneal alkali burn.
Methods:
EDE and chemical burn were induced in C57BL/6 mice by desiccating stress and application of NaOH, respectively. Eye drops consisting of 0.01% globular APN, 0.01% ADPs, 0.1% ADPs, or balanced salt solution (BSS) were applied. Tear volume, tear film break-up time, and corneal staining scores were measured. Concentrations of interleukin (IL)-1β, interferon (IFN)-γ, IL-6, CXCL-9, and CXCL-10 using multiplex immunobead assay were evaluated, and flow cytometry were performed. Corneal epithelial defects and haze degree were analyzed, and enzyme-linked immunosorbent assay for IL-1β and transforming growth factor (TGF)-β levels were observed.
Results:
All treatment groups showed an improvement in clinical parameters and CD4+CCR5+ T cell and CD11b+ cell infiltrations in the conjunctiva (all P < 0.05). Both ADPs groups had significantly decreased concentrations of IL-1β, IFN-γ, IL-6, CXCL-9, and CXCL-10 in the conjunctiva than the EDE or BSS group. Significantly improved parameters of epithelial defect, degree of haze, and concentrations of IL-1β and TGF-β were observed in all treatment groups. However, no significant differences were noted in clinical or experimental parameters among treatment groups.
Conclusion:
Topical ADPs could effectively improve clinical signs and inflammation of ocular surface in the EDE or alkali burn, and its efficacy and potency were similar to those of globular APN.
Introduction
Adiponectin (APN) is a 244 amino acid large cytokine that is 30 kDa protein secreted mainly by the adipose tissue. 1 The protein structure is similar with tumor necrosis factor (TNF)-α and has useful outcomes against insulin resistance and inflammatory case.2–8 APN signals through 2 receptors, AdipoR1/R2, leading to activation of AMP-activated protein kinase. 9 Previous studies suggest that APN participates in immunoregulatory effect, results in increased levels of anti-inflammatory cytokines and decreased levels of proinflammatory factors.10–12
In our previous study, we demonstrated that globular APN could improve clinical parameters and reduce inflammation of ocular surface in the experimental dry eye (EDE). 13 In addition, globular APN could promote wound healing in an experimental model of chemical burn. 14 However, APN protein are still unavailable, as a result of difficulties in converting the full-sized APN protein into a viable systemic regulator. The excessive insolubility of the C-terminal domain and larger peptide fragments are main reasons preventing the pharmacological utilization of APN protein. 15
APN-derived short peptides (ADPs) are first-in-class APN receptor agonists. 16 The lead peptide, 10-mer ADPs 355, is similar to full-sized APN, which involved C-terminal domain. Recently, ADPs has been shown to have nontoxic properties and remarkable stability in the human serum. It was found to exhibit the typical effects of APN and prevent brain injury caused by human immunodeficiency virus protease inhibitors.17,18
In our research, we evaluate the potency of topical ADPs compared with the globular APN in a mouse model of EDE and after chemical burn.
Methods
Mouse model design and experimental procedures
This research protocol was confirmed by the Chonnam National University Medical School Research Institutional Animal Care and Use Committee. All animals were treated in accordance with the Association for Research in Vision and Opthalmology Statement for the Use of Animals in Ophthalmic and Vision Research. Experiments were conducted using 7 weeks old female C57BL/6 mice.
In the EDE model, subcutaneous injection of 0.5 mg/0.2 mL scopolamine hydrobromide (Sigma-Aldrich, St. Louis, MO) was received by mice 4 times a day at 30% ambient humidity.19–23 The mice were randomly assigned to 6 subgroups: untreated (UT) control; EDE control; EDE mice treated with balanced salt solution (BSS; Alcon, Fort Worth, TX), 0.01% globular APN, 0.01% ADPs 355, and 0.1% ADPs 355. APN eye drops were made by diluting globular monomeric fragment recombinant mouse gAdiponectin/gAcro30 solution (R&D Systems, Minneapolis, MN) or Adipocectin peptides 355 powder (CS13253; CS Bio, Menlo Park, CA) with BSS.
All treated mice given 2-μL eye drops 3 times a day. At 5 and 10 days, we evaluated tear volume, tear film break-up time (TBUT), and corneal staining scores (CSS). Ten days after treatment, multiplex immunobead assay and flow cytometric analysis were performed.
In the chemical burn model, mice were anesthetized with an intraperitoneal injection of ketamine/xylazine. A round piece of filter paper that contained 2 μL of 0.1 M NaOH was placed in right eye. After 10 s, the wounded cornea was rinsed thoroughly by saline. The burn resulted in epithelial defects in all mice. Mice were casually divided into 1 of 4 treatment groups: BSS, 0.01% globular APN, 0.01% ADPs, or 0.1% ADPs, and received eye drops 3 times a day. After 6 h, 1, 2, 3, 5, and 7 days treatment, we measured parameters of epithelial defect and degree of haze. Enzyme-linked immunosorbent assay (ELISA) was observed 7 days after injury induction. In EDE experiment, 3 mice (6 eyes) were used for multiplex immunobead assay and western bolt, and 6 mice (12 eyes) for flow cytometry. In the chemical burn experiment, 6 mice (6 eyes) were used for ELISA. All experiments and analysis were repeated 3 times.
Evaluation of clinical parameters in the ocular surface
Phenol red-impregnated cotton threads (Zone-Quick; Oasis, Glendora, CA) was used to measure the tear volume. 23 The threads were placed in the lateral canthus for 20 seconds. Tear volume, expressed in millimeters of thread wet by the tear and turned red, was measured using a microscope (SMZ 1500; Nikon, Melville, NY).
One microliter of 1% sodium fluorescein was instilled into the inferior conjunctival sac, then TBUT was recorded by slit lamp (BQ-900; Haag-Streit, Bern, Switzerland). Punctate staining in the surface of cornea was assessed after 90 s. The cornea was distributed into 4 parts and scored separately. CSS were calculated through a 4-point scale and added up a final score (0–16). 24
Western blot
Western blot was used for activation of AMPK and NF-κB in the conjunctival tissues (6 eyes per group). Proteins were extracted from conjunctiva using a lysis buffer (mammalian protein extraction reagent [M-PER]; Pierce Biotechnology, Rockford, IL) with protease inhibitor cocktail. Centrifugation of the lysates was at 25,200 g and 4°C for 10 min. Proteins of the sample were separated and transferred to polyvinylidene difluoride membranes. 25 The blots were then washed with tris buffered saline with Tween® (TBST, 10 mM Tris-HCl [pH 7.6] mixed with 150 mM NaCl and 0.05% Tween-20 detergent), blocked with 5% skim milk for 1 h, and incubated for 2 h at room temperature with primary antibodies. 25 After incubating with secondary antibodies, the immunoreactive bands were visualized using an enhanced chemiluminescence system (ECL Blotting Analysis System; Amersham, Arlington Heights, IL). Anti-β-actin was used as an inner control.
Multiplex immunobead assay
Multiplex immunobead assay (Luminex 200; Luminex Corp., Austin, TX) for concentrations of interleukin (IL)-1β, IL-6, interferon (IFN)-γ, CXCL-9, and CXCL-10 was performed in the conjunctiva (6 eyes per group). 22 Samples of conjunctiva were collected for 30 min and pooled in lysis buffer containing protease inhibitors. Cell extracts were centrifugated at 15,000 rpm and 4°C for 15 min. The supernatants that were stored at −70°C were added to wells containing the appropriate cytokine bead mixture for 60 min, which included mouse monoclonal antibodies specific for the cytokines and chemokines. After washing, the biotinylated secondary antibody mixture was applied for 30 min in the dark at room temperature. The reactions were detected after addition of streptavidin-phycoerythrin using an analysis system (xPONENT; Luminex Corp.).
Flow cytometric analysis
Flow cytometry was performed to determine the number of CD4+CCR5+ T-cells and CD11b+ cells from the conjunctiva (6 eyes per group) using a previously described method.25,26 Tissues were mixed with collagenase (Roche Applied Science, Indianapolis, IN) for 60 min. Cells were ground, retrieved, centrifuged, and resuspended in phosphate-buffered saline (PBS) with 1% bovine serum albumin. The samples were washed and then incubated with antibodies for 30 min at 37°C. FACSCalibur cytometer with Cell Quest software (BD Biosciences) was performed on the CD4+CCR5+ T cells and CD11B+ cells.
Evaluation of corneal wound healing and haze
All mice photos were captured using a stereoscopic microscope (SMZ 1500®; Nikon). 14 Epithelial defect staining was taken with 0.1% fluorescein. The area and longest diameter of the epithelial defects were calculated using Image-Pro Plus® software. The haze degree was scored clinically on a numerical scale of 0–4, as previously described. 14
Enzyme-linked immunosorbent assay
Total transforming growth factor (TGF)-β and IL-1β levels from cornea (6 corneas per group) were detected by ELISA (Quantikine®; R&D Systems). Corneal tissues were excised and kept in reserve at −80°C. After homogenized samples in PBS, the lysates were centrifugated at 10,000g 4°C for 10 min. Supernatants were collected and measured by Bradford assay. TGF-β and IL-1β protein detection was performed with commercially available sandwich ELISA kits with capture and detection antibodies as per the manufacturer's instructions. ELISA was repeated 3 times.
Statistical analysis
The statistical analyses were done using Statistical Package for Social Sciences (version 17.0; SPSS, Chicago, IL). Results are presented as mean ± standard deviation. The data were analyzed using 1-way analysis of variance with a Tukey post hoc analysis; P < 0.05 was considered statistically significant.
Results
Tear film and ocular surface parameters
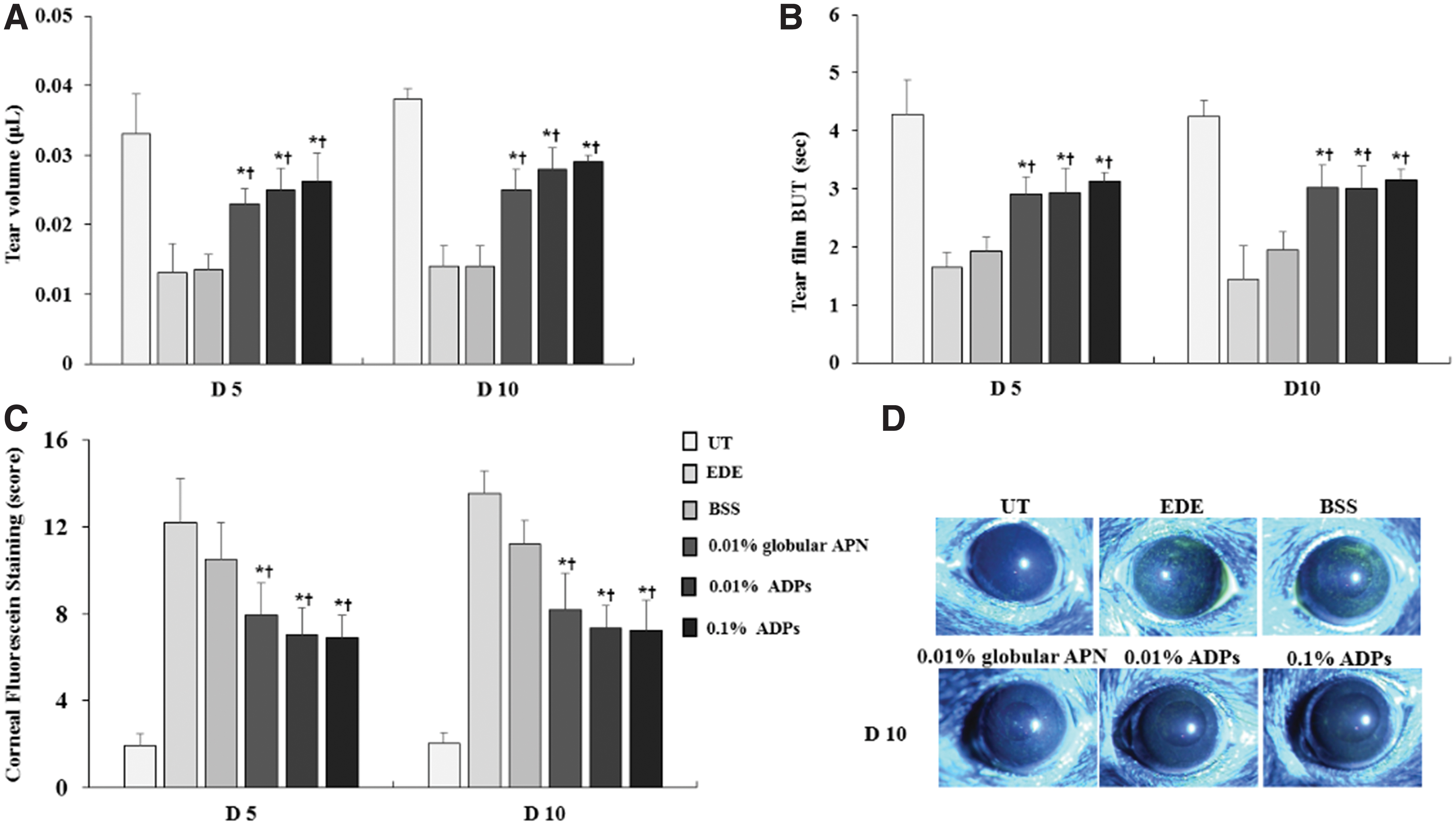
The mean tear volume was 0.033 ± 0.006 μL (UT), 0.013 ± 0.004 μL (EDE), 0.014 ± 0.002 μL (BSS), 0.023 ± 0.003 μL (0.01% globular APN), 0.025 ± 0.003 μL (0.01% ADPs), and 0.026 ± 0.004 μL (0.1% ADPs) in the respective groups, at 5 days. Ten days after treatment, the respective tear volume was 0.038 ± 0.002 μL (UT), 0.014 ± 0.003 μL (EDE), 0.013 ± 0.003 μL (BSS), 0.025 ± 0.003 μL (0.01% globular APN), 0.028 ± 0.003 μL (0.01% ADPs), and 0.029 ± 0.001 μL (0.1% ADPs) (EDE vs. 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs, P < 0.05; BSS vs. 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs, P < 0.05, Fig. 1A).
Mean tear volume
Five days after induction, values for TBUT were 4.28 ± 0.61 s in the UT, 1.65 ± 0.26 s in the EDE, 1.93 ± 0.23 s BSS, 2.91 ± 0.30 s in the 0.01% globular APN, 2.93 ± 0.42 s in the 0.01% ADPs, and 3.12 ± 0.16 s 0.1% ADPs groups, respectively. The respective values were 4.25 ± 0.28 s (UT), 1.45 ± 0.57 s (EDE), 1.94 ± 0.31 s (BSS), 3.01 ± 0.40 s (0.01% globular APN), 2.99 ± 0.39 s (0.01% ADPs), and 3.15 ± 0.16 s (0.1% ADPs) at 10 days (EDE vs. 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs, P < 0.05; BSS vs. 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs, P < 0.05, Fig. 1B).
At day 5, the CSS were 1.93 ± 0.57 in the UT, 12.22 ± 2.03 in the EDE, 10.50 ± 1.68 in the BSS, 27.93 ± 1.52 in the 0.01% globular APN, 7.03 ± 1.25 in the 0.01% ADPs, and 6.89 ± 1.04 in the 0.1% ADPs groups, respectively. At day 10, the respective CSS were 2.05 ± 0.47 (UT), 13.55 ± 1.04 (EDE), 11.22 ± 1.09 (BSS), 8.17 ± 1.70 (0.01% globular APN), 7.35 ± 1.04 (0.01% ADPs), 7.25 ± 1 (0.1% ADPs) (EDE vs. 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs, P < 0.05; BSS vs. 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs, P < 0.05, Fig. 1C). All 3 treatment groups showed significantly improved clinical parameters in comparison to the EDE or BSS group, although no significant differences were found between APN and ADPs treatment groups.
Activation of AMPK and NF-κB in conjunctiva
Figure 2 showed activation of AMPK and NF-κB in the conjunctiva. In the EDE group, we found that AMPK activation was reduced and NF-κB activation was increased. Contrasting with EDE group, the topical application of ADPs or globular APN showed reversed activations of AMPK and NF-κB.

Western blot analysis of AMPK and NF-κB activation in the UT, EDE, BSS, 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs groups at day 10 (6 eyes for each group).
Concentrations of inflammatory factor in the conjunctiva
All treatment groups had significantly lower concentrations of IL-1β, CXCL-9, and CXCL-10 than the EDE or BSS group. IFN-γ and IL-6 concentrations in the 0.01% or 0.1% ADPs group were decreased than those in the EDE and BSS groups (Table 1).
Concentrations of IFN-γ, IL-1β, IL-6, CXCL-9, and CXCL-10 in the Conjunctiva of UT, EDE, BSS, 0.01% Globular APN, 0.01% ADPs, and 0.1% ADPs Groups in Experimental Dry Eye
P < 0.05 compare to the EDE control group.
P < 0.05 compare to the BSS group.
IL, interleukin; IFN, interferon; UT, untreated; EDE, experimental dry eye; BSS, balanced salt solution; APN, adiponectin; ADP, adiponectin-derived short peptide.
Flow cytometry
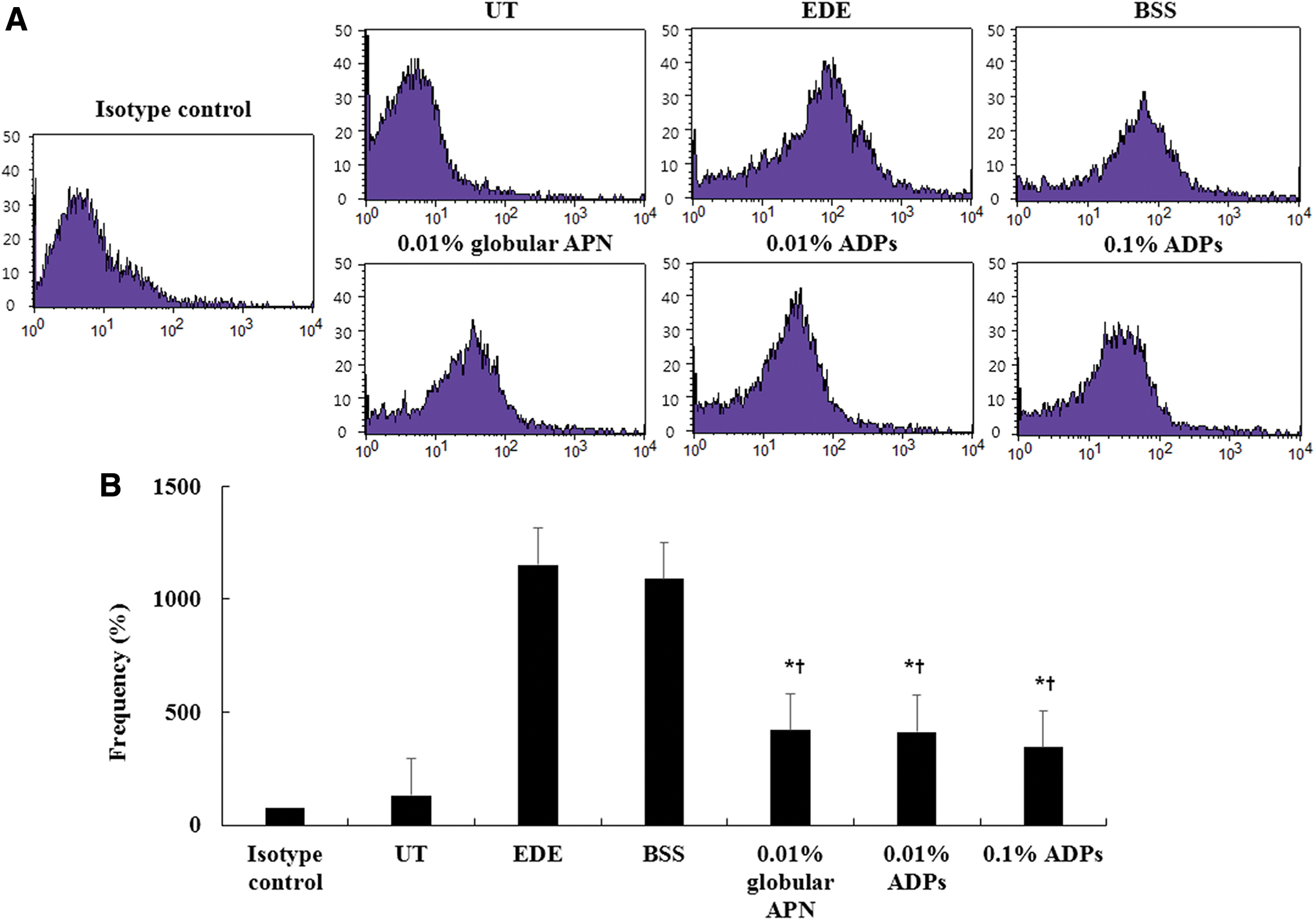
Percentages of CD4+CCR5+ T cells and CD11b+ cells from typical samples in the UT, EDE, BSS, 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs groups using histogram are shown in Figs. 3 and 4. The respective conjunctival CD4+CCR5+ T cell counts were 14.45% ± 5.32% in the UT group, 31.23% ± 10.07% in the EDE group, 27.81% ± 7.95% in the BSS group, 22.84% ± 8.27% in the 0.01% globular APN group, 18.16% ± 6.48% in the 0.01% ADPs group, and 16.64% ± 5.77% in the 0.1% ADPs group (EDE vs. 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs, P < 0.05; BSS vs. 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs, P < 0.05, Fig. 3). Furthermore, percentages of conjunctival CD11b+ cell were 100% ± 0% in the isotype-control, 130.67% ± 5.86% in the UT, 1152.33% ± 78.53% in the EDE, 1090.00% ± 81.85% in the BSS, 420.00% ± 45.83% in the 0.01% globular APN, 413.33% ± 47.09% in the 0.01% ADPs, and 343.33% ± 41.63% in the 0.1% ADPs groups (EDE vs. 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs, P < 0.01; BSS vs. 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs, P < 0.01, Fig. 4A, B), respectively. The APN- and ADPs-treated groups showed significantly decreased percentages of CD4+CCR5+ T or CD11B+ cell in comparison to the EDE and BSS groups.
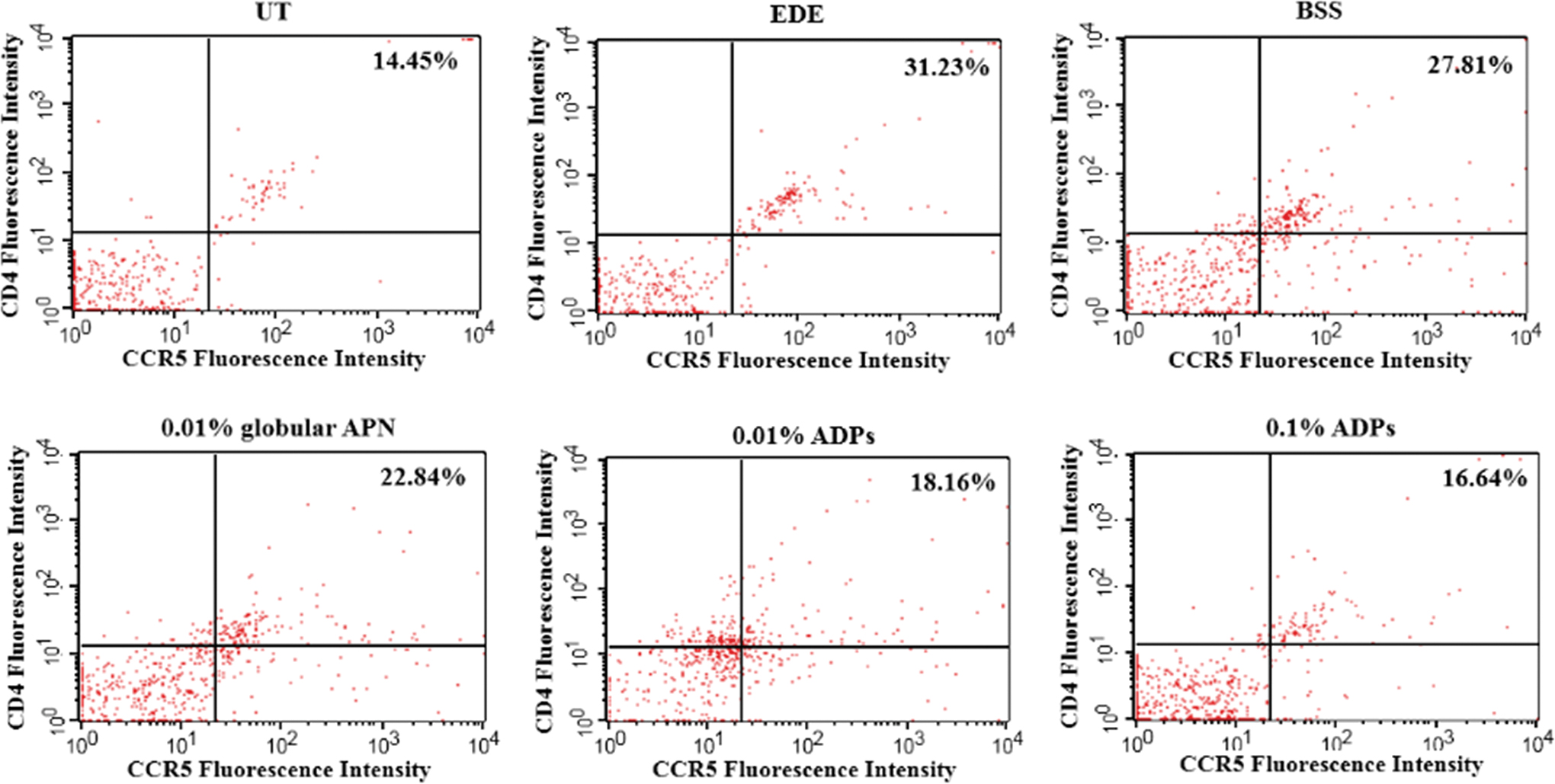
Flow cytometry showing CD4+CCR5+ T cells in the conjunctiva of the UT, EDE, BSS, 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs groups after 10 days of treatment (6 eyes per group). Three treatment groups show a lower percentage of CD4+CCR5+ T cells than the EDE or BSS groups. Color images are available online.
Flow cytometry showing representative histograms (
Parameters of epithelial defects
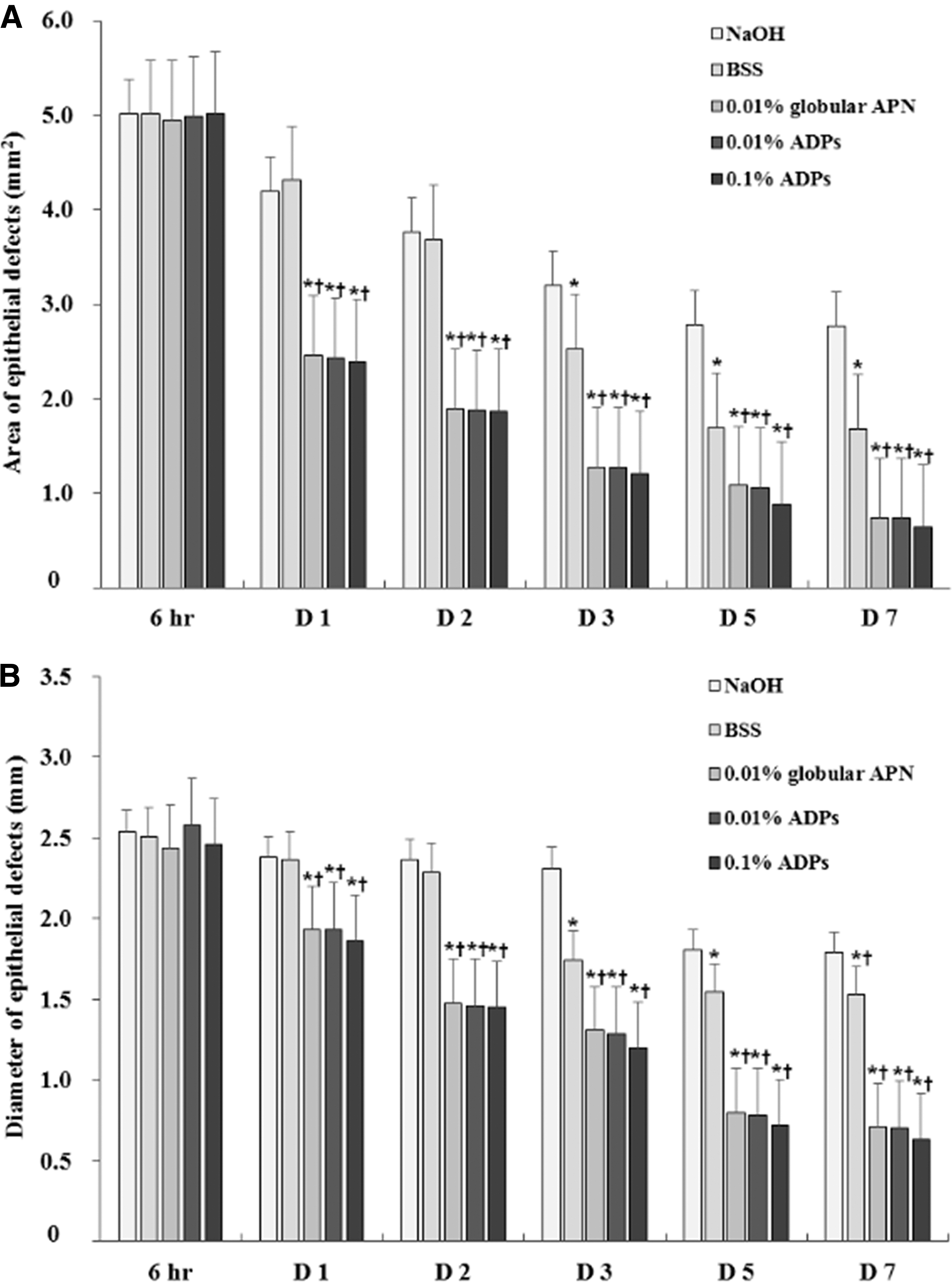
Figure 5A showed that the 0.01% globular APN-, 0.01% ADPs-, and 0.1% ADPs-treated groups had a significantly smaller area of defects compared to the NaOH and BSS groups from 1 to 7 days after treatment. After 3 days, a smaller defect of area was found in the BSS group than that in the NaOH group (P = 0.02). The defects of diameter showed a similar trend in all groups (Fig. 5B). Time to complete re-epithelialization was 8.97 ± 1.74 days in the NaOH control group, 7.50 ± 1.32 days in the BSS group, 5.58 ± 1.58 days in the 0.01% globular APN-treated group, 5.79 ± 1.05 days in the 0.01% ADPs-treated group, and 5.03 ± 1.94 days in the 0.1% ADPs-treated group, respectively (Fig. 6). Regarding all parameters of epithelial defects, there were no significant differences between the 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs groups.
Changes of areas
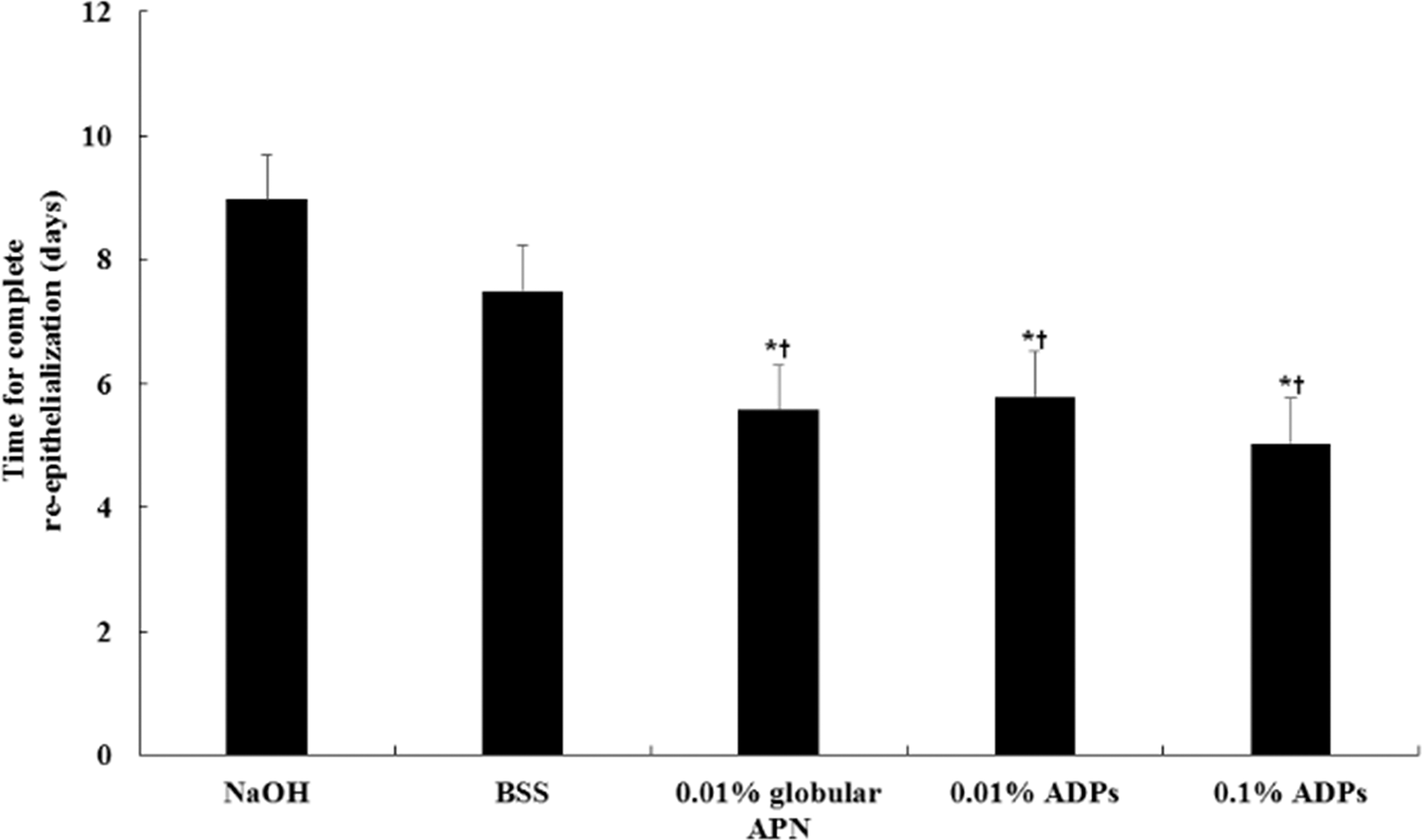
Mean time to complete epithelialization in the NaOH, BSS, 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs groups. ADPs and globular APN treated groups show a faster time to complete epithelialization compared to the NaOH or BSS groups. *P < 0.05 compared to the NaOH group, †P < 0.05 compared to the BSS group.
Degree of corneal haze
From 3 to 7 days after treatment, the 0.01% globular APN, 0.01% ADPs, and 0.1% ADPs groups showed a significantly lower degree of corneal haze than that in the NaOH or BSS group, with no difference among treatment groups (P < 0.05; Fig. 7A, B).
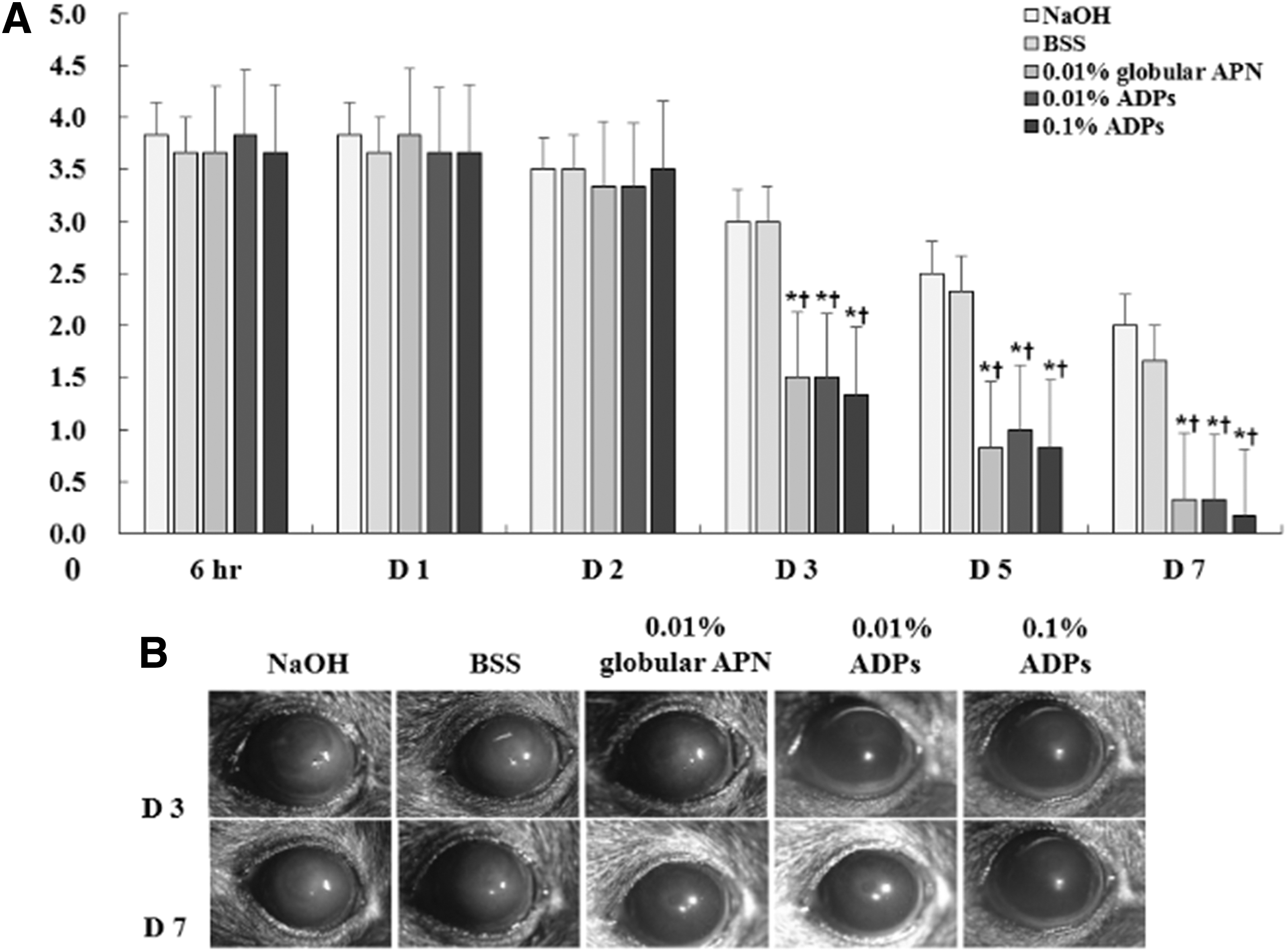
Changes of corneal haze scores
Enzyme-linked immunosorbent assay
All treatment groups had significantly lower concentrations of TGF-β and IL-1β in the cornea than the NaOH and BSS groups, with no significant difference between globular APN and ADPs treatment groups (P < 0.05; Fig. 8A, B).
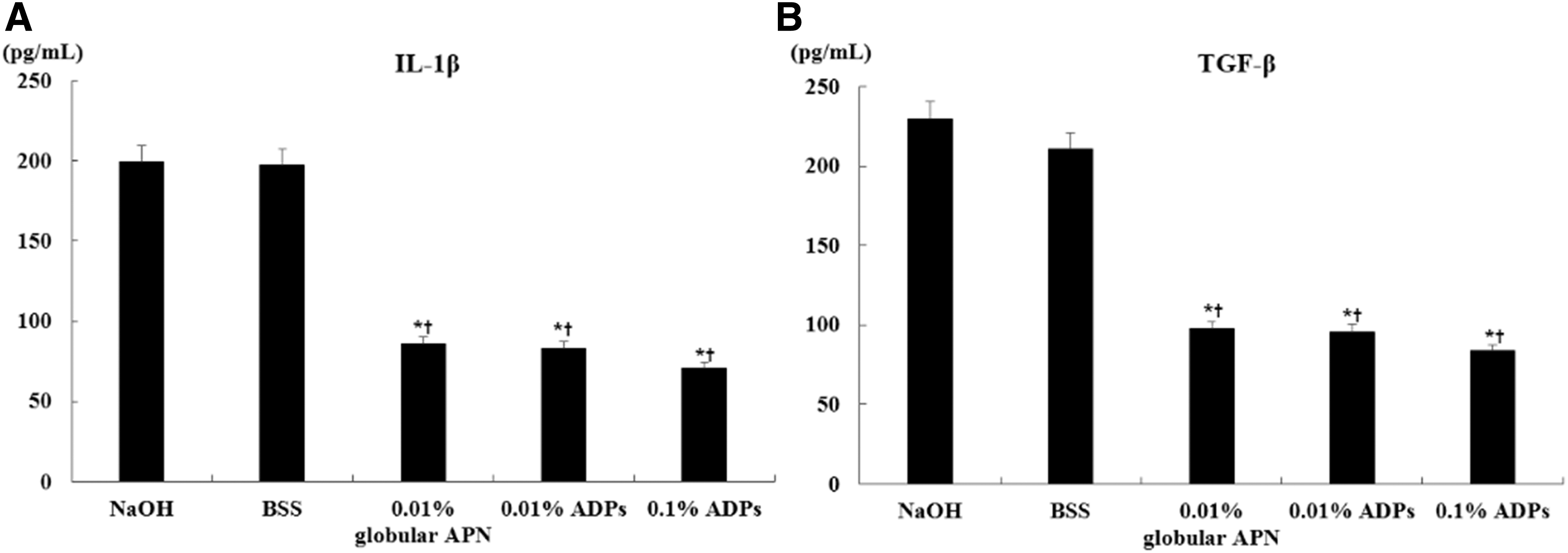
IL-1β
Discussion
Dry eye disease is a condition correlation with the inflammation of ocular surface and characterized by loss of tear production and tear film instability. Accordingly, the process of potential inflammation should be evaluated at great length. Anti-inflammation is an important point for treatment of dry eye.
APN decreases the production of proinflammatory factors, such as TNF-α and enhances the excretion of anti-inflammatory mediators for instance IL-10 and IL-1Rα.10–12 In addition, APN can decrease the autoimmune inflammation and apoptosis by activating AMPK. 26
A previous study demonstrated that ADPs was a first-in-class APN receptor agonist, similar to the full-sized APN, and could modulate several important signaling pathways in an APN-like manner, with a greater contribution of AdipoR1. 15
In the present research, eye drop instillation of ADPs caused refinement of clinical signs and reduced the inflammation in the conjunctiva of mice in an EDE model. Mice treated with 0.01% or 0.1% ADPS, which was similar to globular APN-treated mice, showed improved tear production in comparison to EDE or BSS-treated mice. Enhanced AMPK activation and reduced NF-κB were found in the ADPs or globular APN-treated group than the EDE and BSS groups. Concentrations of IL-1β, IL-6, IFN-γ, CXCL-9, and CXCL-10 and numbers of CD4+CCR5+ T cell and CD11b+ cell from conjunctiva meaningfully reduced in the globular APN and both ADPs groups similarly in comparison to the EDE or BSS groups. These results mean that topical ADPs with the same concentration as globular APN could sufficiently upgrade the clinical arguments in the ocular surface by activating AMPK and restraining the conjunctival factors of inflammation, in T cells.
Wound healing is a resurfacing, reconstitution, and restoration of the injured tissue. Re-epithelialization that participates in wound shrinkage is a crucial process. 27 Epithelial healing is essential in cases of alkaline burn because microbial infection could rapidly continue further damage of epithelium. 28 A previous study suggested that activation of AdipoR1 and AdipoR2 on the ocular surface plays an important part in facilitating cell migration and wound healing. 14 Consistent with previous results, topical application of ADPs and APN significantly promoted re-epithelialization after alkaline burn in our study.
TGF-β and inflammatory cytokines are regarded as important components in wound healing.29,30 During corneal wound healing, TGF-β processes tissues fibrosis and inflammation and regulates the migration and proliferation of corneal cells. In addition, TGF-β could control chemotaxis of monocytes and macrophages.31,32 After chemical burn, IL-1β is induced by corneal epithelial cells in the early phase. 33 In our results, concentrations of TGF-β and IL-1β were lower in the ADPs or APN treatment group. These findings support that topical ADPSs at a similar concentration to APN could promote wound healing by reducing inflammation.
In conclusion, treatment using ADPs 355 could increase tear production and decrease the levels of inflammatory cytokines, CD4+ T cells, and CD111b+ cells in EDE, similar to APN treatment. ADPs also could promote re-epithelialization and wound healing and decrease inflammation of the ocular surface after alkali burn. Our results demonstrate that topical treatment with the small-sized ADPs had therapeutic efficacy equivalent to the full-sized APN protein in dry eye and ocular alkali burn.
Disclaimer
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was partially supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Science, ICT and Future Planning (2017R1A2B4003367), and the CNUH Biomedical Research Institute (CRI18093-1 and BCRI19038).