
Abstract
Purpose:
To assess the long-term anatomical and functional findings in patients with symptomatic vitreomacular traction (VMT), with or without full thickness macular hole (FTMH), after eye treatment with intravitreal ocriplasmin injection (IOI).
Methods:
This longitudinal case series includes 51 eyes from 51 symptomatic patients with VMT (<800 μm) who received a single IOI (Jetrea® 0.125 mg); 21 cases with an FTMH (<400 μm) were included. Best-corrected visual acuity (BCVA) and optical coherence tomography findings were recorded before IOI, and 1 day to 24 months thereafter. Data are presented as mean ± standard deviation.
Results:
Mean adhesion size before injection was 345 ± 146 μm. In 34 eyes (67%), complete release of VMT was observed; whereas VMT persisted in 17 eyes (33%). The latter included 15 of the 21 eyes (71%) with FTMH, 15 of which underwent pars plana vitrectomy and inner limiting membrane peeling. BCVA improved from (logarithm of the minimal angle of resolution [logMAR]) 0.41 ± 0.03 before injection to 0.32 ± 0.03 after 1 month and 0.23 ± 0.05 after 6 months and remained stable thereafter (0.24 ± 0.06 after 24 months of follow-up). Forty-five percent of the eyes presented submacular deposits soon after IOI that were not functionally relevant; 61% completely resolved by 12 months. Except floaters that disappeared within 48 h, no other adverse events were reported during follow-up.
Conclusions:
Treatment with ocriplasmin in a real-life setting showed an overall efficacy of 67% in patients with symptomatic VMT, with better results evident in the absence of an FTMH (70% vs. 62% VMT release) and a visual gain for over 2 years.
Introduction
During the initial stages of posterior vitreous detachment, adhesions may remain between the vitreous body and retina. This is called vitreomacular adhesion (VMA) and is usually asymptomatic with spontaneous resolution. Eventually, VMA may progress to vitreomacular traction (VMT) where adhesions form between the vitreous body and the foveal center. 1 VMT can lead to metamorphopsia, reduced visual acuity, blurred vision, dysopsia, scotoma, and, in some cases, macular holes (MH), which can be either a lamellar or a full thickness macular hole (FTMH). 2
Vitrectomy and membrane peeling have been the mainstay of treatment for symptomatic cases. As vitrectomy poses certain risks, such as infection, retinal detachment, hemorrhage, and cataract, it is usually only used when the patient starts to experience loss of vision.
Asymptomatic or mild cases are traditionally managed by observation. In cases with disease progression however, therapeutic options such as an intravitreal injection of ocriplasmin or vitrectomy are considered. The purpose of therapy is to release vitreous traction on the macula before the occurrence of irreversible structural retinal damage.
Substances that are directed against biochemical components of the vitreomacular interface, including chondroitinase, dispase, and hyaluronidase, have been tested but were abandoned due to insufficient clinical efficacy and/or complications.3–5
Ocriplasmin, a serine protease, enzymatically induces a “pharmacological vitreolysis” as it breaks down fibronectin and laminin at the pathological vitreoretinal interface. 6 Preclinical and clinical studies have demonstrated that ocriplasmin can induce vitreous liquefaction and separation from the retina.7–13
Recently, subretinal deposits and fluid, as well as outer segment changes, have been reported after ocriplasmin injections by several groups.14–20 It is, however, not yet known how those affect long-term visual acuity and whether the reported subretinal deposits are resorbed after a certain amount of time.
In this retrospective observational case series, 51 patients with symptomatic VMT were treated with a single intravitreal ocriplasmin injection (IOI) between February 2014 and July 2018 and followed up for 6–48 months. VMT release and MH closure rates, visual acuity changes, and subretinal deposit resolution, as well as its effect on visual acuity and potential risk factors for its development, were examined and analyzed.
Methods
The study was approved by the local institutional ethics committees in Bern (Kantonale Ethikkommission Bern and Zuerich, reference No. 2016-02084). Informed consent was obtained from each participant in accordance with the tenets of the declaration of Helsinki.
Patients were included in the series if they had persistent (>3 months) and symptomatic VMT without spontaneous release and an adhesion size <1,500 μm with or without concomitant FTMH (with a maximum size of 400 μm). Exclusion criteria included coexistence of any foveal or extrafoveal epiretinal membrane (ERM), clinically insufficiently controlled glaucoma, structural damage to the macula excluding functional gain, retinal detachment, and any systemic disease interfering with the local situation (i.e., systemic vasculitis), and any diabetic retinopathy. All eyes received 1 single injection of 0.125 mg ocriplasmin (Jetrea® ThromboGenics; Alcon/Novartis, EU) under sterile conditions in accordance with local standard procedures.
The primary endpoint was anatomical success, defined as complete VMT release and/or MH closure.
Secondary endpoints included change in best-corrected visual acuity (BCVA) from before to up to 24 months after Jetrea injection, and development and evolution of subretinal deposits visible in optical coherence tomography (OCT) in response to treatment.
All patients with a persistent and symptomatic VMT that fulfilled the inclusion criteria (adhesion size <1,500 μm and an MH size <400 μm, no ERM) were, thus, eligible for treatment.
Based on a success rate of 50%, they were given the choice of the following options: treatment with a single intravitreal injection of ocriplasmin; or surgery (pars plana vitrectomy [PPV] ± cataract surgery). Patient selection for an IOI treatment was the same as for vitrectomy provided the inclusion criteria for an ocriplasmin injection were given. Consequently, all patients were informed in advance that they were scheduled for vitreoretinal surgery if experiencing ocriplasmin treatment failure.
Eighty-six percent wanted to try an ocriplasmin injection first, due to the prospect of not having to undergo surgery in successful cases. The baseline characteristics of the patients who decided against the IOI (14%) were comparable to those who had opted for it (data not shown).
BCVA testing and OCT (Spectralis™; Heidelberg Engineering, Heidelberg, Germany) were performed to assess visual and morphological outcomes, including VMT release and FTMH closure over time.
Data appertaining to the patients were retrieved from their electronic records and from the OCT database entries that were linked to the corresponding visits. Measurements of BCVA were performed in Snellen, when necessary; BCVA was determined on a logarithmic scale and converted to Early Treatment Diabetic Retinopathy Study (ETDRS) letters; and conversion between different notations was performed regarding the ranges of vision loss defined in ICD-9-CM.
We used the central retinal thickness scan and directly measured with the measuring tool of the Spectralis Software (Spectralis; Heidelberg Engineering) on a micrometer scale the size of VMT and the MH in μm; no further calculation of adherence or lesion size was performed.
Regarding the macular subretinal deposits (MSDs), we registered clinically as well as in the OCT images if subretinal deposits were present at the different time points of our follow-up period; no specific analysis was performed.
The Shapiro-Wilk test confirmed that our data were normally distributed. Numerical data are presented as mean values and standard deviations. Data were analyzed by using Student's t-test. A P value <0.05 was considered statistically significant. We used the Point-biserial correlation (a special case of Pearson's correlation) to screen for interrelationships between 1 continuous and 1 nominal variable with 2 categories. The Chi-square test for association was applied to test whether 2 categorical variables are associated. All statistical evaluations were performed by using the SPSS software package V.23 (SPSS, Inc., Chicago, IL).
Results
During the study period, a single intravitreal injection of ocriplasmin was administered to 51 eyes of 51 patients who met the inclusion criteria. The mean follow-up period was 24 ± 14 months (range: 6–48 months), and the mean age of the patients was 76 ± 8 years (range: 50–94 years). About a quarter of patients (27.4%) were pseudophakic at the time of inclusion (Table 1).
Baseline Characteristics of Patients with Symptomatic Vitreomacular Adhesion Treated with Intravitreal Ocriplasmin
BCVA, best-corrected visual acuity; F, female; FTMH, full thickness macular hole; logMAR, logarithm of the minimal angle of resolution; M, male; MH, macular hole; VMT, vitreomacular traction.
The mean duration of symptoms was 7.5 ± 1.9 months. The mean adhesion size before injection was 345 ± 146 μm; the maximum adhesion size of the VMT in our patient cohort, however, did not exceed 800 μm (Table 1). An FTMH was present in 21 instances (41%) with a mean hole size of 263 ± 110 μm. The mean time to complete release of VMT was 12.5 ± 19.9 (2–115) days (n = 34, 67%) after successful IOI. The success rate in eyes with VMT and without FTMH was 70% (21of 30 eyes). In eyes complicated by an FTMH, the success rate was 62% (13 of 21 eyes). Interestingly, despite complete release of VMT in 13 of 21 eyes with VMT and FTMH, complete hole closure was only achieved in 6 cases (29% of all eyes with FTMH) (Table 2). PPV, in combination with cataract surgery in phakic cases, was performed in 15 eyes with persisting VMT. In addition, 4 eyes without full closure of FTMH despite VMT release after Jetrea injection also underwent PPV surgery. Two of the 21 patients who required PPV decided against surgery.
Clinical Characteristics of Patients with Symptomatic Vitreomacular Adhesion Treated with Intravitreal Ocriplasmin
The mean BCVA (logarithm of the minimal angle of resolution [logMAR]) improved from 0.41 ± 0.03 before injection to 0.32 ± 0.03 at 1 month (n = 51, P = 0.05), 0.23 ± 0.05 at 6 months (n = 27, P = 0.0005), 0.24 ± 0.05 at 12 months (n = 32, P = 0.001), and 0.24 ± 0.06 at 24 months (n = 27, P = 0.003) after injection (Fig. 1). The Supplementary Fig. S1 depicts the mean BCVA (logMAR) for all timepoints of all patients who completed 24 months of follow-up (n = 27).
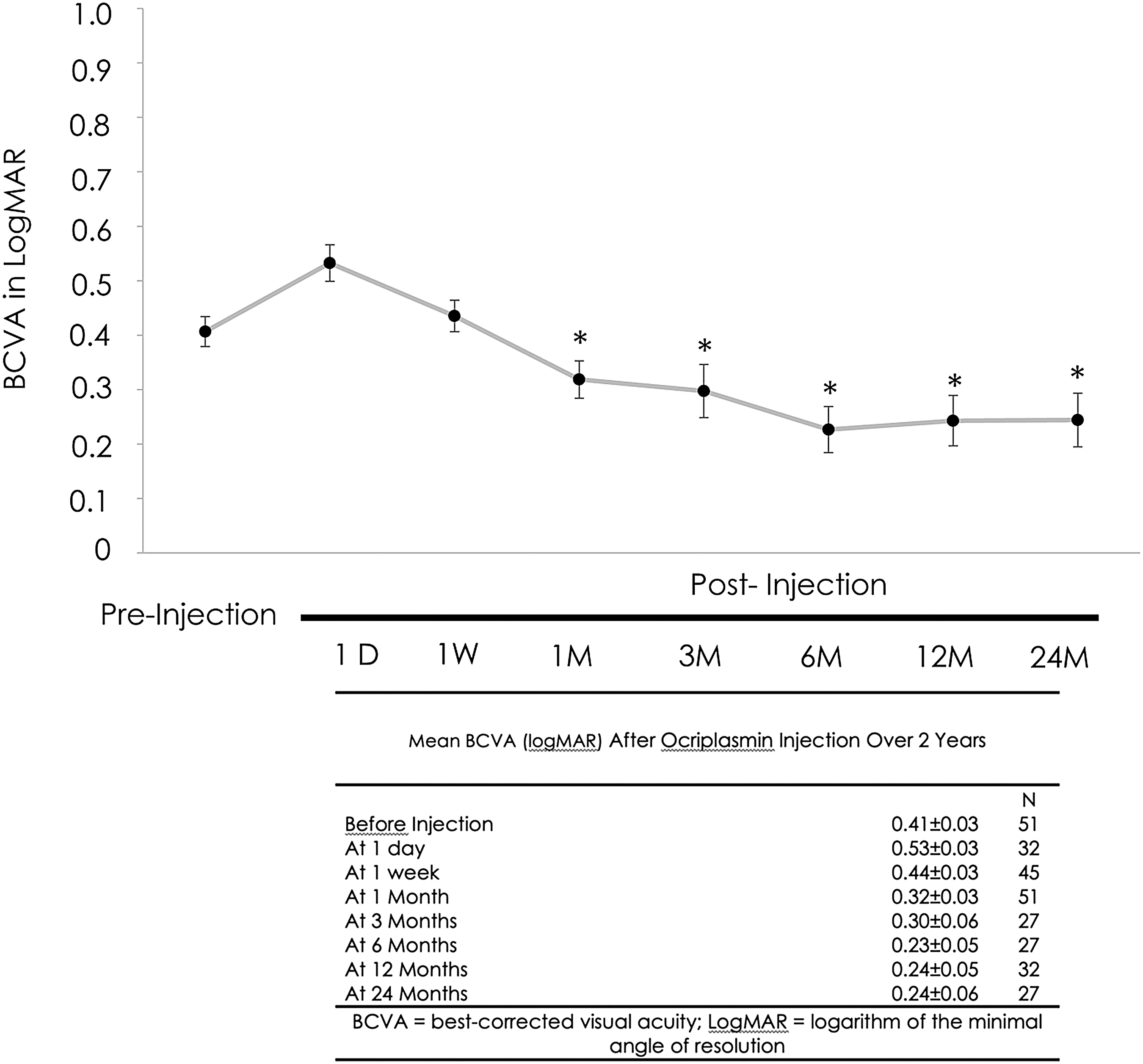
BCVA in logMAR: before the first injection of ocriplasmin (Pre-Injection) and 1 day, 1 week, and 1, 3, 6, 12, and 24 months later, *P ≤ 0.05. Error bars represent the SEM. BCVA, best-corrected visual acuity; logMAR, logarithm of the minimal angle of resolution; SEM, standard error of the mean.
In patients with successful release of the VMT and without persistent MH, the mean BCVA (logMAR) before injection was 0.37 ± 0.05 and improved to 0.26 ± 0.05 at 1 month (n = 30, P = 0.05), 0.29 ± 0.08 at 3 months (n = 12, P = 0.27), 0.20 ± 0.06 at 6 months (n = 15, P = 0.01), and 0.21 ± 0.05 at 12 months (n = 23, P = 0.005) after injection. Patients without successful release of the VMT or with persistent MH had a baseline BCVA of 0.45 ± 0.03 (n = 21) before injection with no improvement seen 1 month after ocriplasmin injection (visual acuity 0.43 ± 0.04, n = 21, P = 0.62). One month after PPV, however, the BCVA improved to 0.34 ± 0.11 (n = 14, P = 0.20). Further improvement was evident 3 (0.29 ± 0.07, n = 14, P = 0.02), 6 (0.37 ± 0.11, n = 11, P = 0.34), and 12 months (0.35 ± 0.11, n = 8, P = 0.22) after PPV surgery.
The nonstatistical difference in baseline BCVA of patients without need of vitrectomy (n = 30) versus unsuccessful (n = 21) release of the VMT or persistent MH after IOI with the need of PPV (0.37 ± 0.05 vs. 0.45 ± 0.03, P = 0.55) may be explained by the percentage of eyes with a concomitant MH (23.3% vs.66.7%).
Forty-one percent of patients needed a vitrectomy in spite of prior IOI. The mean time to vitrectomy was 1.9 ± 0.7 months (Supplementary Fig. S2).
The patients without release of VMT and/or persistent MH after IOI who underwent PPV showed an improvement of BCVA over 12 months after vitrectomy that was similar to the patients with successful release of VMT after IOI (Supplementary Fig. S2). There were no adverse events other than 2 patients with transient intraocular pressure rise shortly after PPV that could be controlled medically and disappeared by 1 month after surgery.
Floaters were reported by all 51 patients after ocriplasmin injection; however, these disappeared within 24–48 h. No ocriplasmin drug-related complications, including lens destabilization, phacodonesis, dyschromatopsia, retinal tear, or retinal detachment, were observed over the 48-month period. One phakic patient required cataract surgery after 4 years.
MSDs were evident in 23 eyes (45%) after ocriplasmin injection; of these, 61% resolved within 12 months (Table 2 and Fig. 2). This was comparable in eyes with VMT with and without FTMH. Complete resolution of the deposits occurred within 3 months in 50% of eyes with VMT and FTHM and within 1 year in the other 50%, with a similar mean FTHM size of 172 μm compared with 196 μm. In eyes with VMT without FMTH, 56% showed resolution of the deposits within 3 months, 22% within 6 months, and 22% within 1 year. Symptoms improved in response to VMT resolution in all cases independent of the presence of subretinal deposits. There was no statistical difference in BCVA (logMAR) at any time point between eyes with and without subretinal deposits.
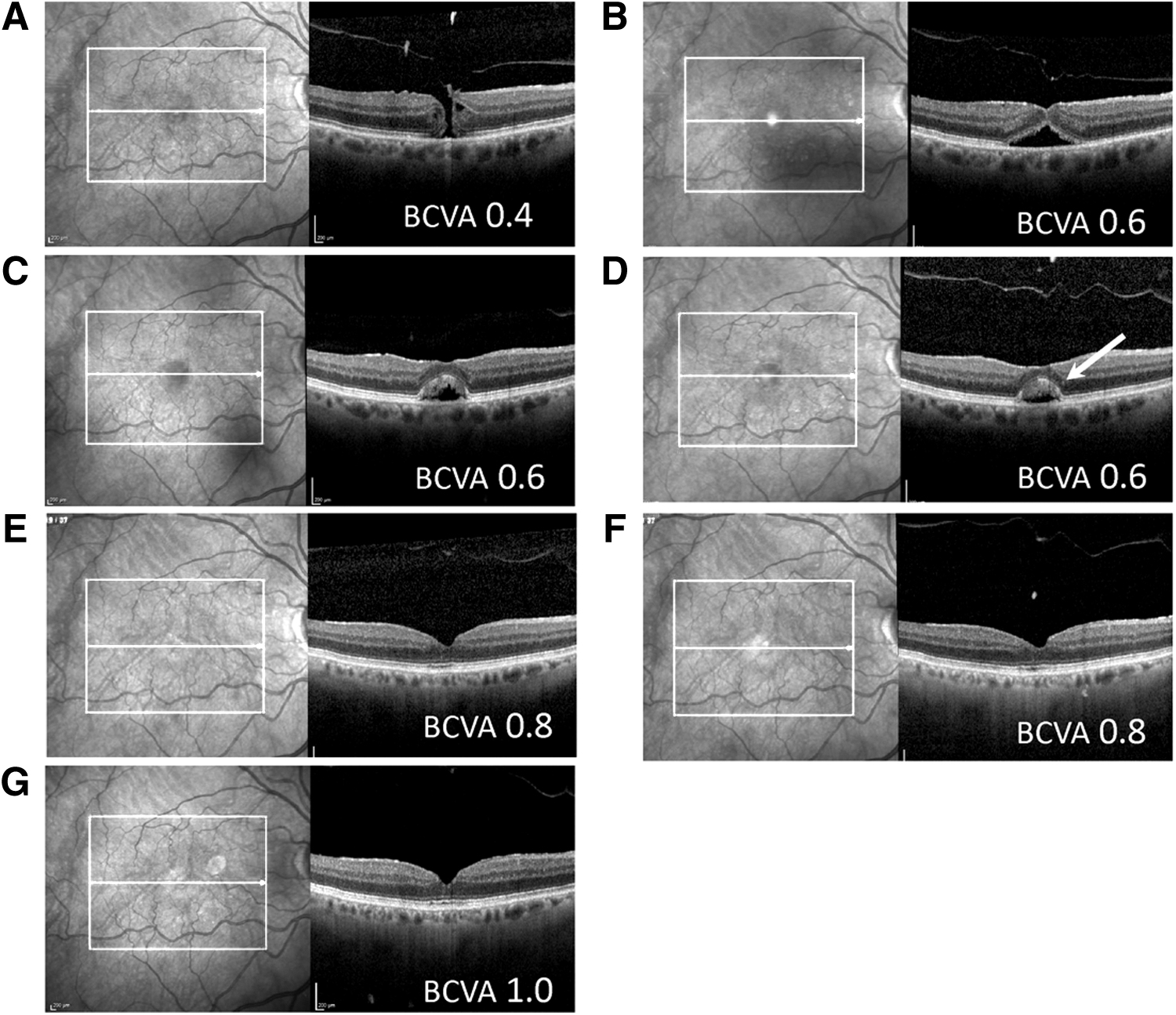
Representative images of macular subretinal deposit resolution over time. The box appears automatically when measuring with SD-OCT and shows the area that is measured.
Further, we screened our data regarding potential factors predicting success or failure. Success was defined as a vision gain of more than 5 ETDRS letters and resolution of VMT. Interestingly, neither the size of the VMT and the MH, nor the presence of MSDs seemed to play a role in the success of VMT resolution. Regarding the presence of MSD, neither the VMT size nor the presence of an MH and its size did affect the visual outcome after IOI at the measured time points (Supplementary Table S1).
Further, we tried to identify potential risk factors for the development of subretinal macular deposits. Interestingly, no correlation was found between age and gender regarding the appearance of MSDs; in addition, MHs and MSDs did not show a correlation. However, VMT and MSD did correlate: rpb = 0.39**, P = 0.005 as did VMT and age: rpb = −0.36**, P = 0.009, in the sense that with age a VMT resolution becomes less likely and in the case of VMT resolution the development of MSD might increase.
We used the Point-biserial correlation (a special case of Pearson's correlation) to screen for a correlation between age and MSD and could not find any: rpb = (−0.38), P = 0.086. We then used the Chi-square test for association between gender and MSD: P = 0.55 and could not find an association. We, therefore, concluded that gender and age are not playing a role in developing MSD; however, age does play a role in the likelihood of resolution of VMT and its resolution plays a role in the development of MSDs.
Discussion
Our study demonstrates morphological and functional success in 67% of eyes with symptomatic VMT treated with ocriplasmin. A better prognosis was evident in the absence of FTMH without relevant side effects. Careful patient selection and structured standard-of-care pathways to identify patients who might benefit from intravitreal ocriplasmin were important initial steps. This means restricted adhesion and MH sizes below the recommended maximum sizes of 1,500 and 400 μm, as well as the exclusion of eyes with an extramacular ERM.
VMT patients with mild to moderate symptoms often opt for observational management. The findings of Tzu et al., however, indicate a resolution time of 1–1.5 years without intervention. 21 Their study assessed the natural history of VMT in 230 eyes of 185 patients who were under observation for 32 months. A spontaneous release of VMT without treatment was reported in 31.7%. 21
For patients with symptomatic long-standing VMT, the prospect of vitrectomy can be daunting, and patients are often apprehensive about the potential surgical risks.22–24 Stalmans reported that observation of patients with VMT and delay in intervention result in disease progression. 25 In these situations, less invasive treatment with a single intravitreal injection may be an acceptable alternative. The latter has a success rate more than 50% and is cost-effective compared with primary vitrectomy. A crude calculation of total costs, including secondary vitrectomy in eyes without resolution of VMT, in our patients revealed savings of 20% compared with primary vitrectomy, with the additional benefit of minimal risk of surgical complication. This is in accordance with data from Waseem et al., who reported that IOI is a cost-effective intervention compared with primary vitrectomy. 26
A recently published phase 4 study reported a VMT resolution rate of 47.4% after 4 weeks with moderate functional improvement according to a ≥10-letter gain in visual acuity in 31% and a tendency to better VMT resolution in FTMH of ≤250 μm size. 27 The outcomes seen are slightly less favorable to those observed in our study, indicating that careful patient selection is crucial for good outcomes. Muqit et al. showed a VMT release rate from 69% at 6 months in eyes without ocular co-morbidity. 28 FTHM closure was achieved in 67% of eyes (4/6), whereas we achieved a complete MH closure rate of 29% (6/21 eyes). Release rates were generally found to be positively correlated with an age of below 65 years, absence of ERM, VMT diameter of ≤1,500 μm, and phakic lens status.29–31 This is in keeping with our inclusion criteria. In eyes with MHs >400 μm, or in the presence of ERM, vitrectomy may be the first choice. 32 As has been previously reported, in our series vitrectomy with internal limiting membrane peeling 1 month after unsuccessful ocriplasmin injection yielded similar results in the majority of cases to those expected after primary surgery with closure of MHs. 33 OCT images, in contrast, show more outer structural changes in vitrectomized than in ocriplasmin-treated eyes, and postoperative ellipsoid zone disruption persisted more frequently in vitrectomy-treated eyes. 20 Nevertheless, changes in the ellipsoid zone and in electroretinogram (ERG), which indicates photoreceptor damage, have also been reported after ocriplasmin injection34,35 and have prompted further investigation into potential diffuse effects of ocriplasmin in the retina. 35
In our study, we found 45% MSDs after ocriplasmin injection, of which 61% resolved over a period of 12 months. Previous studies have also reported subretinal fluid and subretinal deposits after ocriplasmin intravitreal injection, particularly in eyes where traction has been successfully resolved.14,16,18,36–38 This seems to be in line with our correlation between resolution of VMT and the development of MSDs, which argues for mechanical stimuli and, subsequently, a possible outer retinal defect repair.
It has been proposed that macular subretinal material deposition is due to a breakdown of photoreceptor outer segments. 14 According to Chen et al., however, ocriplasmin does not affect photoreceptor cells but its effect on the RPE and adjacent structures remains unclear. 12 Alternatively, macular subretinal material deposition may result from diminished retinal pigment epithelium (RPE) function, leading to decreased absorption of subretinal fluid and accumulation of opsin breakdown material along the outer photoreceptor layer. 14 ERG changes post-ocriplasmin injection support this assumption.15,16,36 Along with dyschromatopsia and ellipsoid zone changes on spectral domain-optical coherence tomography (SD-OCT) after ocriplasmin injection, a potential diffuse retinal impact of ocriplasmin cannot be excluded.15,16 The long-term visual acuity outcomes observed in our series, however, argue against a relevant functional impact of these findings up to 4 years. From week 40 post-injection, a resolution of serous detachment and a decrease in the amount of subretinal material found may indicate RPE recovery. 14 This is in line with our findings; in 61% of eyes with subretinal deposits, complete resorption was observed after 12 months. The deposition of macular subretinal material after ocriplasmin injection had no functional relevance in our series. However, when screening our data regarding potential factors predicting success or failure, we concluded that gender, age, VMT, and MH size are not correlated in developing MSDs; nevertheless, age does play a role in the resolution of VMT and its resolution is associated with the development of MSDs.
Conclusion
Our retrospective case series demonstrated improved functional and anatomical success in 67% of patients with symptomatic VMT after a single IOI. The effect on resolution of VMT and BCVA improvement lasted up to 24 months; thus, long-term negative effects of ocriplasmin on retinal function are unlikely.
Footnotes
Acknowledgment
Assistance in organizing the study was provided by U. Hornberger, a study nurse at Triemli Hospital Zürich.
Author Disclosure Statement
J.G.G. acts as an advisor to several pharmaceutical companies and has contributed to several pharma-sponsored international clinical studies that are independent of this study. The research foundation at the City Hospital Triemli has received research grants (Novartis, Bayer) and reimbursement for consultancy work by S.M. (Novartis, Bayer, Allergan, Roche, Pfenex, Clanotech). Nevertheless, neither of them nor the other authors received direct support for this study or have conflicting interests with regards to the data presented here.
Funding Information
The study was partially supported by the Werner H. Spross Foundation (Zürich, Switzerland).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.