
Abstract
Biomechanical properties of the cornea have recently emerged as clinically useful in risk assessment of diagnosing glaucoma and predicting disease progression. Corneal hysteresis (CH) is a dynamic tool, which measures viscoelasticity of the cornea. It represents the overall deformability of the cornea, and reduces significantly with age. Low CH has also been associated with optic nerve damage and progression of visual field loss in glaucoma. The extracellular matrix (ECM) constituents of the cornea, trabecular meshwork (TM), sclera, and lamina cribrosa (LC) are similar, as they are predominantly made of fibrillar collagen. This suggests that biomechanical changes in the cornea may also reflect optic nerve compliance in glaucomatous optic neuropathy, and in the known increase of TM tissue stiffness in glaucoma. Increased collagen cross-linking contributes to tissue stiffening throughout the body, which is observed in normal aging and occurs at an accelerated rate in systemic conditions such as fibrotic and cardiovascular diseases, cancer, and glaucoma. We reviewed 3 ECM cross-linking proteins that may have a potential role in the disease process of increased tissue stiffness in glaucoma, including lysyl oxidase (LOX)/lysyl oxidase-like 1 (LOXL1), tissue transglutaminase (TG2), and advanced glycation end products. We also report elevated messenger RNA (mRNA) levels of LOX and TG2 in glaucoma LC cells to support our proposed theory that increased levels of cross-linking proteins in glaucoma play a role in LC tissue stiffness. We highlight areas of research that are needed to better understand the role of cross-linking in glaucoma pathogenesis, leading potentially to a novel therapeutic strategy.
Introduction
The Ocular Hypertension Trial Study (OHTS) identified thinner central corneal thickness (CCT) measurements as a baseline factor that predicted the development of primary open-angle glaucoma (POAG). 1 Elevated intraocular pressure (IOP) is the only known modifiable risk factor for glaucoma development and progression, and lowering IOP is known to slow progression.2–5 Thinner CCT results in an underestimation of the true IOP measurement. However, inaccuracy of IOP measurements alone cannot fully explain the relationship between CCT and glaucoma risk. We propose that understanding the biomechanical properties of the cornea and their response to pressure would provide a more comprehensive understanding of its role in glaucoma. 6
Corneal hysteresis (CH) is a biomechanical property of the cornea relating to its viscoelasticity—specifically, the relative ability of the cornea to absorb pressure by bending when pressure is applied. Lower CH has emerged as a potentially significant factor in the development and progression of glaucoma, and CH of <10 mmHg has been found in glaucomatous patients when compared to normal controls.7–13 Low CH indicates a stiffer cornea, which suggests it is unable to disperse the internal force (i.e., stress) created by raised IOP within the anterior segment. This undispersed stress could potentially be transmitted posteriorly to the optic nerve head (ONH), 14 contributing to optic nerve cupping and neuronal cell death. Low CH may also be indicative of globe biomechanical properties and susceptibility to IOP stress. 15
The cornea consists of 5 layers and the stroma accounts for 90% of the corneal volume and consists of mostly Type I collagen fibrils16,17 in its extracellular matrix (ECM). The ECM of the cornea is also rich in proteoglycans such as keratin sulfate and dermatan sulfate—all of which contribute to the transparency and structural mechanics of the cornea. 18 Type IV collagen is only found in basement membranes (BM) and acts as a scaffolding protein 19 to maintain the function of the BM, which includes induction of cell differentiation and facilitation of cell migration. 20 The presence of Type IV collagen has been observed in the corneal epithelium BM and Descemet's membrane.21,22 A potential cause of low CH could be an increase in collagen cross-linking within the cornea, as seen in the normal aging process. 23
Tissue stiffness can be defined as the degree to which a tissue resists deformation in response to applied stress. The tissue biomechanical property depends largely on the ECM, where its constituents such as elastic fibers, fibrillar collagen, and glycoaminoglycans (GAGs) are regulated to achieve mechanical homeostasis. 24 Increased collagen cross-linking is observed with increasing age and contributes to the disease process of various systemic conditions, including arteriosclerosis, renal, hepatic, and pulmonary fibrosis, and cancer.25–27 Enzymes that cross-link between 2 proteins, normally between collagen and another ECM constituent such as elastin, are regulated to maintain mechanical homeostasis. Altered cross-linking processes result in tissue stiffness.
There are 3 cross-linking proteins potentially associated with glaucoma, which include lysyl oxidase (LOX)/lysyl oxidase-like 1 (LOXL1), tissue transglutaminase (TG2), and advanced glycation end products (AGEs). These proteins have been implicated in the increased stiffness of the eye as a consequence of increased expression in the lamina cribrosa (LC)28–30 or trabecular meshwork (TM) cells. 31
The aim of this review is to provide an understanding of the biomechanical properties of the cornea and its relevance to glaucoma, coupled with an overview of collagen cross-linking proteins in relationship to glaucoma. We will also discuss future potential therapeutic strategies in reducing the risk of developing and progression of this blinding disease.
Literature search strategy
As preparation for writing this review article, we performed a literature search to identify all of the relevant scientific articles. We used the PubMed database as our searching tool and entered keywords, including aging, glaucoma, ocular stiffness, CH, collagen cross-linking proteins, optic nerve stiffness, and ECM. We also made use of the relevant studies referenced in selected articles that were not identified from our initial search process. There was no constraint on publication date and we included articles that are published in English language only.
CCT and Glaucoma
The cornea and its significance in glaucoma were first highlighted by the OHTS trial.1,32 Goldmann Applanation Tonometry (GAT) was introduced in the 1950s and has become the standard for IOP measurement in clinical practice. The development of GAT and IOP measurement provided a basis for IOP to be recognized as a modifiable risk factor in the development and progression of glaucoma. The key influence of CCT on IOP and glaucoma development was not known for a further 50 years.
Brandt et al. 32 found that subjects with ocular hypertension (OHT) had thicker corneas than the general population. African American subjects had thinner corneas than white subjects, while thicker CCT was associated with younger age, female gender, and diabetes. Thus, he concluded CCT might influence the accuracy of GAT in the diagnosis, screening, and management of patients with glaucoma and OHT.
Several studies noted the influence of CCT on IOP measurement and suggested it would be ideal to adjust for CCT to attain the “true” IOP.33,34 However, there is no consensus on a robust formula for this “correction factor” to eliminate the confounding CCT value in IOP measurement.
CCT as a risk factor for progression of glaucoma
Gordon et al. 1 found that participants in the OHTS with a CCT <555 μm had a 3-fold greater risk of developing glaucoma. The Early Manifest Glaucoma Trial (EMGT) found that thinner CCT (1.01–1.55 per 40 μm lower) may play a role in predicting progression in those with higher baseline IOP. 35 Other studies have shown that progression of visual field loss in glaucoma was associated with thinner CCT measurements.35–39 Thus, the role of CCT in glaucoma is likely more complex than inaccuracy of IOP measurement, leading to undertreating /overtreating of glaucoma. It is likely that the human cornea and its biomechanical properties rather than just CCT alone influence the risk of development and progression of glaucoma.
Corneal Hysteresis
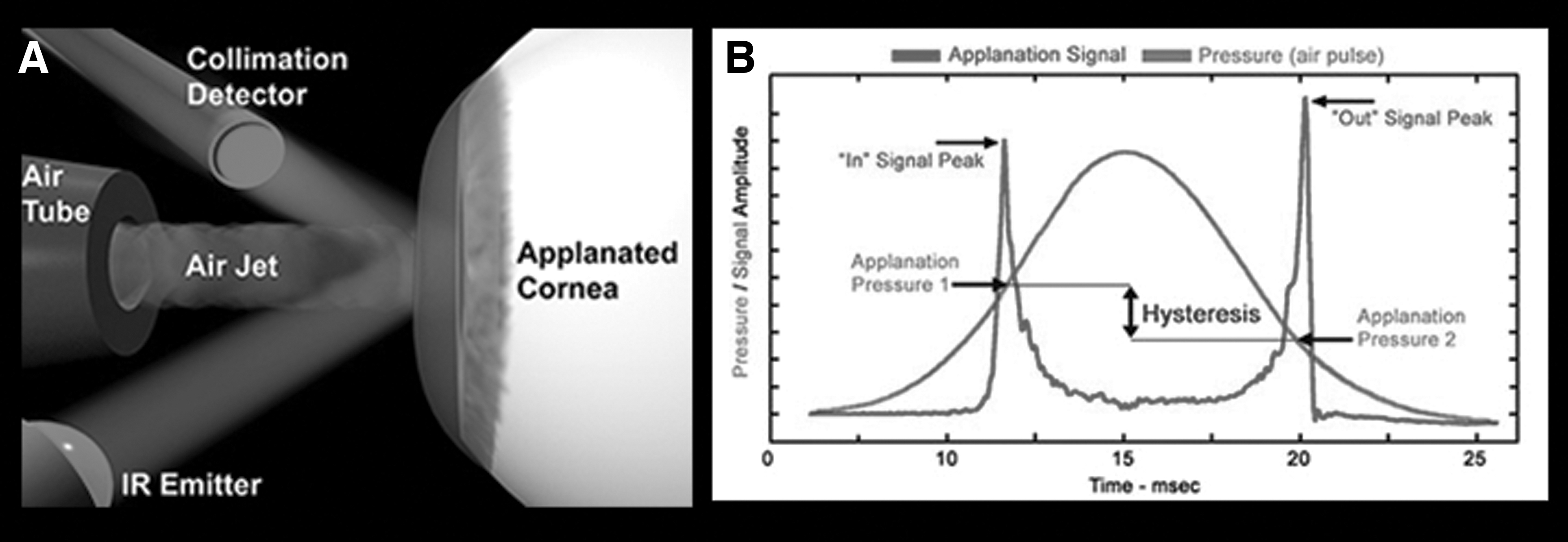
CH is defined as the nature of the cornea's response to an applied force and is dependent on both the elastic and viscous properties. The Reichert Ocular Response Analyzer (ORA; New York, NY) is a simple and noninvasive technique that is commercially available to measure the biomechanical properties of the cornea and CH. As CH is a measure of the cornea's ability to absorb and dissipate energy, the ORA uses the concept of rapid loading/unloading mechanism on the cornea. Bidirectional applanation by air-jet pressure measures the viscoelastic property of the cornea, which is detected by a photodetector (Fig. 1A). 40 The difference between the rapid loading pressure (P1) and rapid unloading pressure (P2) in mmHg is the CH (Fig. 1B). 40
Recently, a second commercial instrument has been introduced into clinical practice. The Oculus Corvis ST (Wetzlar, Germany) captures corneal deformation, IOP, and pachymetry measurements using Scheimpflug images to provide a detailed analysis of the biomechanics of the cornea.
CH and aging
A recent cross-sectional study within the UK Biobank with 93,345 eligible participants explored the distribution of CH and its associated factors. 41 It was found that CH was significantly associated with age, gender, and ethnicity, all of which are known risk factors for developing glaucoma and should be taken into account when interpreting CH values. In this large cohort group, lower CH was significantly associated with higher prevalence of self-reported glaucoma.
There are various studies that precede and support the UK Biobank's findings. CH in normal controls has been shown to be between 10.2 and 12.6 mmHg,42–44 with little variation in CH over a 24-h period.44,45 CH is thought to be heritable, with the strongest correlation found among monozygotic twins 46 and first-degree relatives. 47 In terms of ethnicity, Detry-Morel et al. compared the CH values between 30 African with 25 Caucasian normal subjects. They found African normal (non-glaucoma) subjects to have lower CH (8.3 ± 1.7 mmHg, P < 0.001) in comparison to Caucasians (9.2 ± 1.1 mmHg) 48 of the same age.
CH decreases with increasing age.13,45,49–51 Mean CH among children has been found to be between 11.78 and 12.5 mmHg.13,49 The European Prospective Investigation of Cancer (EPIC)-Norfolk Study 50 found a mean CH of 9.35 mmHg in men and 9.74 mmHg in women over 80 years of age. Ortiz et al. 51 found CH in those 60–80 years of age was 10.0 ± 1.2 mmHg and significantly lower when compared to a younger group (children 9–14 years of age, CH = 11.1 ± 1.1 mmHg, P = 0.01).
The more recent Antioxidants, Essential Lipids, Nutrition and Ocular Diseases (ALIENOR) Study 52 also confirms lower CH values (mean = 9.4 mmHg) in an elderly population (mean age = 82). They also found that the CH values within this group are associated with elevated plasma low-density lipoprotein cholesterol and higher lifetime ultraviolet radiation exposure, both of which may modify the biomechanical structure of the cornea.
CH in glaucoma
Early studies by Mangouritsas et al. 7 found that CH in POAG subjects (mean 8.95 mmHg) was significantly lower than normal age-matched controls (mean 10.97 mmHg). Kaushik et al. 53 found among a large cohort of 323 subjects, including normal OHT, PACG, POAG, and normal-tension glaucoma (NTG) subjects, that the POAG and NTG group had the lowest CH value (Table 1).
Corneal Hysteresis Values from Various Studies Measuring Across Glaucoma Subtypes
CH, corneal hysteresis; NTG, normal-tension glaucoma; OHT, ocular hypertension; PACG, primary angle-closure glaucoma; POAG, primary open-angle glaucoma; PXFG, pseudoexfoliative glaucoma.
Further studies examining CH in glaucoma and OHT patients found CH values of POAG and NTG subjects were significantly lower than those of OHT subjects.8,53 In both normal and glaucoma patients, CCT increases as CH does,8,10,43,54–57 suggesting that corneal viscoelastic behavior may be influenced by its thickness.
There is a moderate positive correlation between CH and CCT, with CH being significantly lower in glaucoma in comparison to OHT. 8 Following a multivariate analysis, CH was the only multivariate variable that was independently related to glaucoma, which could differentiate POAG from OHT. 8 Similarly, Pillunat et al. found a statistically significant correlation between ORA parameters with IOP, CCT, axial length, and age. 58 They also found that POAG patients had the lowest adjusted CH values (8.96 ± 1.4 mmHg) in comparison to patients with OHT (10.2 ± 1.5 mmHg) and controls (9.7 ± 1.4 mmHg). When adjusted for the correlated factors, corneal biomechanical parameters may be helpful to stratify the severity of POAG patients, which determine the management plans for this group of patients. 58 The same of group of researchers also evaluated the effect of trabeculectomy on corneal biomechanical properties and IOP measurements. They measured ORA parameters of 35 glaucoma patients undergoing first-time trabeculectomy with mitomycin C and found there was no significant difference of CH values pretrabeculectomy and post-trabeculectomy (CHpre-trab = 7.75 ± 1.5 mmHg vs. CH post-trab = 7.62 ± 1.7 mmHg, P = 0.72). The corneal compensated IOP (IOPcc) of these patients was markedly and significantly reduced postoperatively and the accuracy of ORA-IOP measurements is not altered following this procedure.
Several studies have found CH to be lower among patients with NTG, especially if the eye showed evidence of progression. In asymmetric NTG, the worse-eye group had lower CH of 6.8 mmHg when compared to the better-eye group (CH = 7.6 mmHg). Among 82 patients with progressive NTG, patients who showed progression had lower CH (CH = 9.4 ± 1.3 mmHg) compared to patients who do not progress (CH = 10.8 ± 1.4 mmHg). 59
It is important to note that among all the glaucoma subtypes, patients with pseudoexfoliative glaucoma (PXFG) tend to have the lowest CH values. 60 Studies that have compared PXFG and POAG have found CH values ranging between 7.6 and 8.8 mmHg in PXFG groups,12,61 which are significantly lower than the POAG groups (CH range 9.1–9.9 mmHg). PXFG is also associated with lower CH in comparison to patients with the pseudoexfoliative syndrome (PXS). Two large group studies investigated the ORA parameters of PXFG and PXS in a Turkish population and found almost similar CH value, which is lower in PXFG (CH = 6.8 ± 1.7 mmHg) when compared to PXS and healthy subjects (CHPXS = 8.2 ± 1.4 mmHg and CHhealthy = 10.3 ± 1.4 mmHg).62,63 Increased corneal stiffness in PXFG is possibly related to deposition of pseudoexfoliative material, which was identified through in vivo confocal microscopy as hyper-reflective substances on the corneal endothelium and anterior stroma. 64
CH as a risk factor for progression of glaucoma
Congdon et al. conducted one of the first studies to assess the association between CCT and CH with glaucoma damage. 65 They found thinner CCT was associated with higher cup disc ratio, lower CH was associated with progressive visual field worsening, and a weak correlation between CCT and CH existed.
Further studies have shown that eyes with lower CH have faster rates of visual field loss than those with higher CH.66,67 De Moraes et al. found a mean global rate of visual field change in mean deviation of −0.34 ± 0.7 dB/year among 153 patients. 66 Lower CH (7.5 ± 1.4 mmHg) and thinner CCT (525 ± 34.2 μm) were noted in individuals with significant progression of visual field defect. 66 Each 1 mmHg lower CH value was associated with a 0.25%/year faster rate of visual field index (VFI) decline over time. 67
These findings are also similar for NTG.15,59,68 Helmy et al. investigated 240 eyes and found CH was inversely proportional to the mean deviation in visual fields among patients with asymmetrical NTG. 15 Park et al. found that eyes with progression of NTG had lower CCT (530.2 ± 38.6 μm), thinner average retinal nerve fiber layer (RNFL) thickness (70.6 ± 16.1 μm), and lower CH (9.4 ± 1.3 mmHg). 59 Rapid VF progression (defined as the upper 25th percentile group of median MD change over 3 years) occurred in NTG patients whose CH is low (8.4 ± 1.1 mmHg) and IOPcc is high (15.8 ± 1.8 mmHg). 68
Glaucomatous structural progression has also been shown to be associated with lower CH. Age and CH were significantly associated with structural optic nerve progression as assessed through flicker chronoscopy. 69 Among 5134 patients in the EPIC-Norfolk study, lower CH was associated with structural changes associated with glaucoma, including rim area and RNFL measured by scanning laser polarimetry. 70
Most studies on CH and glaucoma progression to date have been retrospective, thus whether CH reflects a cause or as a result of progression cannot be determined. However, the Medeiros et al. 67 was a prospective study over 4 years and demonstrated a highly significant correlation between CH and VFI decline (P < 0.001). Baseline CH was the best predictive biomarker for subsequent progression. They also found that the effect of IOP on rates of progression depended on CH, which conforms to the association of CH with deformation of optic nerve surface during transient elevations of IOP. 14
The ECM
The ECM is fundamental in maintaining the form and function of soft connective tissue. 71 The main constituents of ECM that provide mechanical properties for a tissue are elastic fibers, collagens, GAGs, and proteoglycans. 24 Material stiffness is defined as how stress changes in response to deformation 24 and this is maintained by collagens within the ECM. Elastin is another key ECM protein, which plays a role in elasticity to allow flexibility and stretch-relaxation capacity of tissues such as large arteries, lung, ligaments, and skin. 72 In the arterial wall, the elastic fibers that are damaged due to the aging process are not replaced as elastin expression is switched off. This causes more collagen production, which decreases the elastin:collagen ratio and shifts the arterial mechanical properties into the stiffer range of the collagen fibers. 73
The ECM has a reservoir of regulatory molecules, including cytokines, hormones, and extracellular microRNA (miRNA). These regulatory molecules are important for a bidirectional signal transduction process to promote mechanical homeostasis as a response to extrinsic stress signals onto the ECM. 74 In particular, the ECM turnover is necessary to maintain mechanical homeostasis of soft connective tissue in response to increased stress load. Computational models of the ECM suggest that to achieve mechanical homeostasis, it depend on factors including rates of ECM production, rates of ECM removal, the mechanical properties of the ECM constituents, and the degree of prestress value that is built into the constituents. 75 The short-term response to increased loading is characterized by matrix reorganization and collagen cross-linking, and in the long term, this is balanced by matrix degradation and deposition of the new constituents under the appropriate prestress level. 24 The tissue's form and function can only be maintained if the structural constituents that are degraded are replaced with new constituents that have the same properties and in the same ratio, including the same prestress-induced stiffness. 76 If there is imbalanced remodeling and degradation, pathologic signaling will then induce fibrotic responses leading to permanent stiffness of the tissue. 77
Cross-Linking and Tissue Stiffness
The major collagen cross-linking proteins found within the ECM include LOX and TG2, both of which have been described in relationship to tissue stiffness. The critical role of tissue stiffness in the pathophysiology of disease has emerged through numerous studies related to cancer. Increased stiffness as a result of continuous tumor microenvironment remodeling is a hallmark feature of aggressive tumor progression. 27 Each of the collagen cross-linking proteins in this review appears to have a role in tissue stiffness in cancer pathophysiology, which may also provide an insight of its similar role for ocular stiffness in glaucoma.
Breast cancer tissue, for example, can be 10-fold stiffer than normal breast tissue 78 and also appear stiffer on elastography when compared to benign tumors. 79 The breast tumor-associated ECM has been shown to have collagen Type 1 and fibronectin as the most abundant ECM components deposited. 80 Collagen cross-linking in response to increased collagen deposition is mediated by the activity of LOX proteins, which has been described to increase the invasiveness of many types of cancer cells81,82 and tumor metastasis. 83
TG2 has also been found to catalyze cross-linking of ECM proteins, including collagen, fibronectin, and elastin. 84 TG2 accounts for a variety of biochemical activities, including adhesion, migration, growth, survival, apoptosis, differentiation, and ECM organization. 85 Their activities are calcium dependent, and in relationship to ECM organization, TG2 can render ECM proteins resistant to degradation 86 and also induce profibrotic effector functions. 84 The expression of TG2 is elevated in many fibrotic diseases such as pulmonary, 87 hepatic, 88 and kidney 89 fibrosis. TG2 has also been implicated in cancer, where it is associated with cancer cell migration and invasion. 90
In contrast to LOX and TG2, AGEs elicit synergism with oxidative stress. AGEs lead to the generation of reactive oxygen species (ROS) and AGE production is promoted by oxidative stress. 91 They are thought to exacerbate disease progression through 2 general mechanisms. First, these modified proteins form detergent-insoluble, protease-resistant nondegradable aggregates through cross-linking processes and impair normal cellular/tissue functions. Second, AGEs modulate cellular function through binding to specific receptors, receptor for AGE (RAGE). Activation of RAGE initiates a wide range of abnormal responses in cells and tissues such as inappropriate expression of growth factors, alterations in growth dynamics, accumulation of ECM, promotion of vasoregulatory dysfunction, and initiation of death pathways. 92 These 2 mechanisms are found most relevant in context with diabetes and aging where accumulative levels of AGEs are highest and renal function may be impaired.
Ocular Stiffness in Glaucoma
It is hypothesized that stiffening of ocular structures, including cornea, sclera, and LC, may relate to the pathogenesis of glaucoma. 93 Wells et al. 14 found CH to be lower in glaucoma patients, and CH significantly correlated with optic disc compliance in contrast to CCT. They also found that CH was associated with increased deformation of optic nerve surface during transient elevations of IOP. These findings support their hypothesis that if optic nerve rigidity was related to cross-linking between collagen fibrils in the laminae, then it is expected that the greater LC stiffness was associated with lower hysteresis. Lanzagorta-Aresti et al. found a relevant outcome in context to this hypothesis when they showed CH in 61 eyes with OHT or POAG was significantly correlated with LC displacement (R 2 = 0.48, P = 0.03) after medical lowering of the IOP, meaning the least reversal of cupping (LC displacement) following medical IOP-lowering treatment occurs in the stiffest cornea, that is, lower CH. 94
Multiple mechanisms, including glucose-mediated cross-linking, calcium and lipid accumulation, oxidative stress, and enzymatic proteolysis, are implicated in elastic fiber remodeling. The pathogenesis of glaucoma is also likely related to age-related stiffening at the ONH, and within the TM and LC, with increased age as a major risk factor for glaucoma development. The similarities of ECM constituents of the cornea, TM, and LC may also imply that similar cross-linking process can occur within these structures to result in ocular stiffness (Table 2).
A Summary of the Extracellular Matrix Constituents of the Cornea, Trabecular Meshwork, and Optic Nerve Head, Which May Suggest Similar Cross-Linking Processes Occur Within These Ocular Structures
ECM, extracellular matrix; GAGs, glycoaminoglycans.
Source: Marshall et al. 20
The ECM of the human ONH undergoes age-related changes at the LC, which underpin the age- related optic neuropathy as found in glaucoma. Albon et al. found changes in the collagenous and noncollagenous components of the ECM with increasing age.29,95 There is an increase of total collagen and collagen cross-links in the aged LC. 29 Noncollagenous components of ECM of the LC include fibronectin, elastin, and sulfated GAGs. There is an increase of the elastin content (from 7% in the 0–9 age group to 28% in the 80–89 age group), with decreased fibronectin and GAGs, all of which may contribute to changes in mechanical integrity of the ONH. 95 These changes reduce the tissue resilience in response to strain. They followed through these findings by conducting a study to investigate the mechanical compliance of the LC with age. 96 They found that there is an increased stiffness of the LC, whereby the ability to regain its original shape and size after removal of pressure is reduced. This may be related to the more rigid cribriform plates found in an elderly LC, suggesting an increased susceptibility to plastic flow and permanent deformation contributing to axonal damage as seen in glaucoma.
There is now increasing evidence that the biomechanical properties of the TM is altered in glaucoma due to increased collagen cross-linking of the ECM, which results in decreased ECM turnover, abnormal ECM accumulation, and eventually tissue stiffness. 97 Last et al. conducted a study to compare the stiffness of human TM in normal and glaucomatous tissue using atomic force microscopy to measure elastic modulus. 98 They found a 20-fold increased stiffness of the glaucomatous TM (80.8 kPa) compared to normal TM (4.0 kPa), and subsequent mathematical modeling showed substantial impairment in outflow facility with increased TM stiffness.
In normal human cornea, loss of stromal organization as seen in advancing age or corneal pathology results in altered corneal biomechanics. 17 Daxer et al. 99 found that there is a small, but significant age-related increase in the collagen fibril diameter with increased intermolecular spacing and elongation of the collagen fibrils as a result of continual deposition of collagen molecules. These findings agree with a study by Malik et al., 100 in which they found an increase in the cross-sectional area within each corneal collagen molecule (from 3.04 to 3.46 nm2) with advancing age. They also suggested that this may be due to an increase in nonenzymatic cross-linking between collagen molecules, shown by an increase in glycation and AGEs using fluorescence emission.
Collagen Cross-Linking Proteins in Glaucoma
LOX, TG2, and AGEs may have a role in the increased collagen cross-linking processes that lead to ocular stiffness in glaucoma. Table 3 summarizes the mechanism of action of these proteins and their relationship to glaucoma that has been identified so far.
A Description of 3 Collagen Cross-Linkers That May Be Implicated in Ocular Stiffness in Glaucoma
AGE, advanced glycation end product; LOX, lysyl oxidase; LOXL1, lysyl oxidase-like 1; RAGE, receptor for AGE; TG2, tissue transglutaminase; TGF, transforming growth factor.
LOX/LOXL1
There are 5 members in the LOX family and they are copper-dependent enzymes that oxidize lysine residues in elastin and collagen to form covalent cross-links that render these fibers insoluble in the ECM. 101 The LOXL1 or LOX homolog type 1 enzyme is necessary for tropoelastin cross-linking and elastic fiber formation, maintenance, and remodeling. 102 LOX and LOXL1 are very similar in terms of their catalytic domain. 103 Our best knowledge on the LOX family in glaucoma is based on studies in relationship to pseudoexfoliative syndrome (PXS). Thorleifsson et al. 104 was the first to describe the association of LOXL1 in exfoliation glaucoma following a genome-wide association study (GWAS) of the Icelandic population. They identified 2 single-nucleotide polymorphisms (rs1048661 and rs3825942) in exon 1 of the LOXL1 gene associated with an increased risk of developing pseudoexfoliative glaucoma (PXFG).
The pathogenetic concept behind PXS is it is a type of stress-induced elastosis associated with excessive production and abnormal aggregation of elastic fiber components and abnormal enzymatic cross-linking processes. 105 In pseudoexfoliative glaucoma (PXFG), stiffness of the sclera and peripapillary sclera (ppSc) is possibly related to LOXL1 deficiency. 106 Dysregulation of the LOXL1 causes elastic fibers to become highly resistant to degradation or turnover 102 and is associated with ultrastructural alterations of the elastic networks of the laminar beams in PXS eyes. 106 LOXL1 genes are expressed in cultured human TM and may be partly responsible for the increased aqueous outflow resistance in glaucoma due to abnormal cross-linking signaling in the ECM 107 and chronic accumulation of fibrillar PEX aggregates in the outflow pathways. 108 Schlotzer-Schrehardt et al. 108 found that LOXL1 expression was significantly increased in early stages of PXFG; however, at advanced stages, the expression is decreased, which promotes abnormal elastogenesis.
At present, there is inconsistent association of LOXL1 with POAG109–111 ; however, a recent GWAS in an Asian population identified 7 novel susceptibility loci associated with POAG, including LOXL1. 112
Tissue transglutaminase (TG2)
TG2 is a calcium-dependent enzyme responsible for protein cross-linking of lysine and glutamine residues. 113 The resultant cross-linked ECM protein would be highly resistant to proteolysis and degradation. 114 Recent data by Raychaudhuri et al. showed elevated expression of TG2 in the TM increases N-e(G-glutamyl) lysine cross-linking in mice TM. This consequently increases aqueous outflow resistance resulting in IOP elevation. 31
Tovar-Vidales et al. 115 studied the differences in expression and activity of TG2 between normal and glaucoma TM cells. They found that TG2 are present in both normal and glaucoma TM cells; however, there is an increased TG2 expression and enzyme activity in glaucoma TM cells. In addition, fibronectin—a glycoprotein, which binds ECM components that is mediated by TG2, was also found to be elevated in Schlemm's Canal of glaucomatous TM. 115 These results support the potential role of TG2 may be pathogenic in altering the biomechanics of TM, thus increasing outflow resistance in glaucomatous eyes. 115
The ONH and collagen cross-linking proteins
Zeimer and Ogura investigated the mechanical compliance of ONH in glaucoma patients ex vivo. 116 They defined ONH stiffness as low/small displacement of the ONH when the displacement is measured by increasing the IOP to 60 mmHg from a resting IOP of 12 mmHg. The eyes that had more severe glaucomatous changes exhibit a reduced ONH displacement. They suggested their results might be interpreted as a cumulative change in elastic properties of the LC, which is likely due to a change in the ECM of the tissue. This corresponds with findings by many studies that described altered collagen metabolism in glaucoma leading to a change in the physical properties of the LC.117–119
A study by our group reported on global and ECM-focused differential gene expression between POAG and normal LC cells using microarray analysis. 30 They identified 50 most expressed genes in POAG LC cells, which reflected the multimechanistic pathology of glaucoma that included a combination of ECM, cytoskeletal, angiogenic, neuronal, and developmental genes. Of particular interest from this study is the higher expression of the ECM-related gene LOX in the POAG LC cell lines (0.5 fold increase).
We recently examined the messenger RNA (mRNA) expression of TG2 and LOX in human LC cells using standard real-time polymerase chain reaction. Analysis of TG2 and LOX transcripts showed a significantly higher level of both genes in glaucoma LC cells in comparison to normal LC cells (Fig. 2). 120 This unpublished finding suggests that active collagen cross-linking can also occur in glaucoma LC cells due to elevated expression of major cross-linking proteins such as LOX and TG2, which may subsequently alter the mechanical properties and stiffening of the LC, leading to progressive neurodegeneration of the ONH.
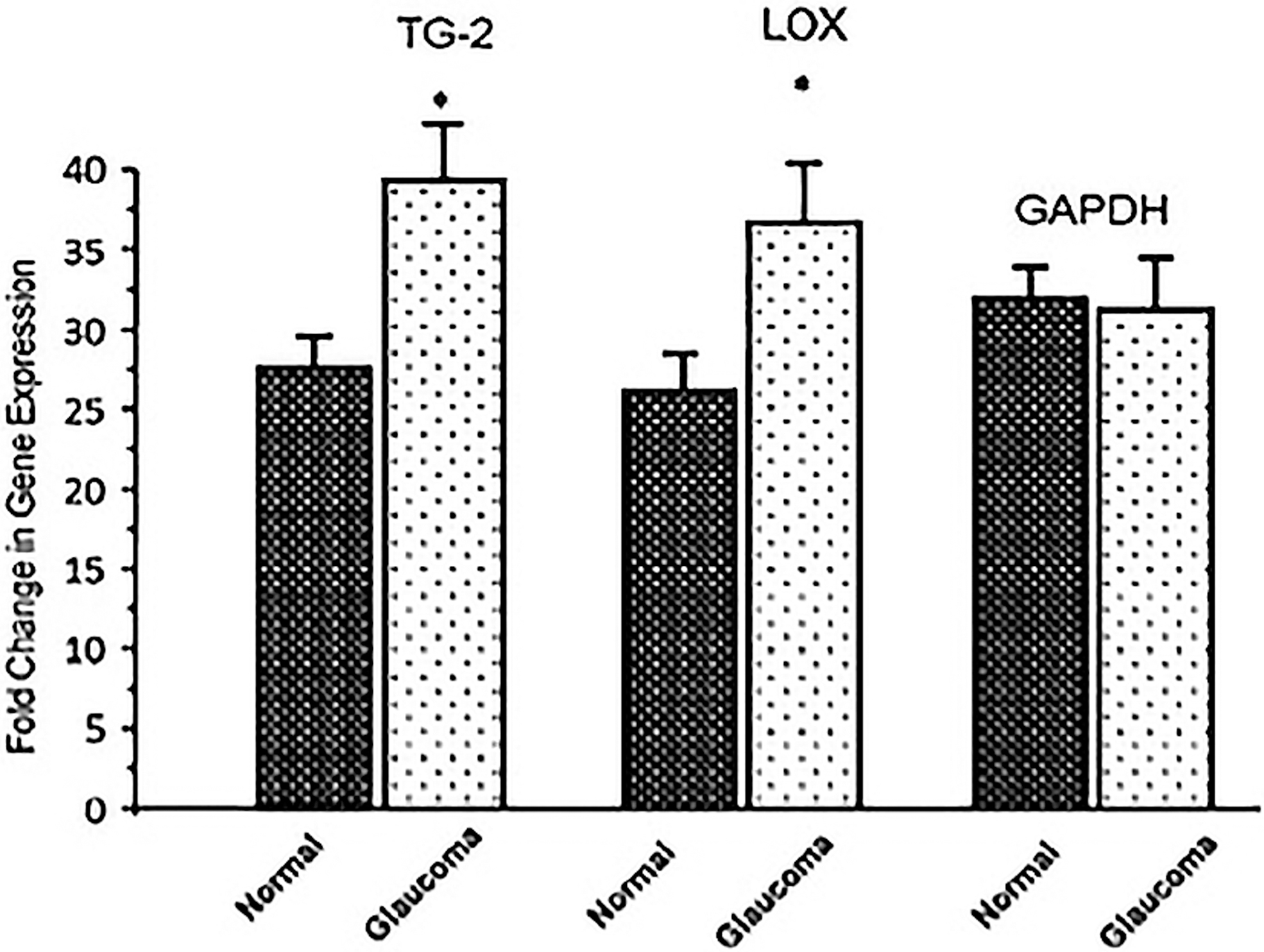
TG2 and LOX expression in normal and glaucoma LC cells. mRNA expression of TG2 and LOX was performed by RT-PCR in normal (n = 3) and glaucoma (n = 3) LC cells lines. Analysis of TG2 and LOX showed that both genes were significantly expressed at higher level in glaucoma LC cells compared to normal LC cells. 119 LC, lamina cribrosa; LOX, lysyl oxidase; mRNA, messenger RNA; RT-PCR, real-time polymerase chain reaction; TG2, tissue transglutaminase.
Advanced glycation end products
AGEs are by-products of nonenzymatic glycation reactions between reactive carbonyl groups of compounds (such as glucose) with proteins, lipids, or nucleic acids. 121 A complex series of reactions (over months or years) leads to metabolic by-products of glycolysis, which interact with extracellular proteins to form - that can bridge between the free amino groups of neighboring proteins to form intermolecular cross-links.
AGEs and the eye
AGEs have been found in the aqueous humor, lens, retina, Bruch's membrane, and optic nerve. 121 Accumulation of AGEs has been found in corneal endothelial cells in elderly populations. 122 Corneal collagen modification following advanced Maillard reactions has been shown to occur in the cornea of diabetics. 123 Nonenzymatic collagen cross-linking causes an increase in cross-sectional areas of collagen fibrils 99 and fibrillar molecules, 100 and a decrease of interfibrillar spacing related to changes in proteoglycan composition of the interfibrillar matrix. 124 This results in increased deposition of ECM in response to cell and matrix disorganization. Similar to the aging process, the mechanism of corneal stiffness is likely related to ECM modification and collagen cross-linking; in glaucoma and diabetes, this could be at an accelerated rate, potentially in the presence of AGEs. As an example, collagen cross-linking mediated by AGEs has been suggested to explain the significant increase in stiffness of diabetic ONH in rats. At 5% strain, the stress of the ONH in diabetic rats (897 ± 295 kPa) was significantly higher than nondiabetic, control rats (671 ± 246 kPa, P = 0.011). 125
AGEs and glaucoma
There is growing evidence of oxidative stress as a disease process in glaucomatous neurodegeneration. 126 AGEs lead to the generation of ROS and AGE production is promoted by oxidative stress. 91 Hondur et al. 127 identified that AGEs and protein carbonyls are promising candidates as oxidative stress-related molecular biomarkers for clinical predictions of glaucoma when they found a 3.1-fold increase of AGE levels in glaucomatous aqueous humor samples in comparison to normal samples (17.6 ± 4.6 vs. 5.7 ± 2.3 μg/mL). Analysis of the aqueous humor is likely useful to provide relevant and specific glaucoma-related information due to its close proximity to disease sites of glaucoma, such as the TM and Schlemm's Canal.
However, AGEs mainly accumulate on long-lived proteins in tissues such as the LC and ONH. Tezel et al. 28 found increased AGE accumulation in glaucomatous tissues in the retina and ONH, supporting the theory that an accelerated aging process accompanies neurodegeneration in glaucomatous eyes. They also found increased signaling of RAGE within retinal glial cells in glaucomatous tissue. Furthermore, substances such as glyceraldehyde and methylglyoxal, which are precursors of AGEs through the Maillard reaction, may also have a role in altering the biomechanical properties of the ECM. Spoerl et al. found an increased stiffness of human LC and ppSc after these structures were treated with glyceraldehyde and methylglyoxal, respectively. 128 In contrast, collagenase A was found to reduce the stiffness of the tissues. 128 This findings support that AGEs can induce changes of the biomechanical behavior of the LC and ppSc, which could potentially be reversed, leading to the development of therapeutic options in glaucoma.
Targeting Collagen Cross-Linking Proteins as a Potential Therapeutic Strategy in Glaucoma
Based on numerous studies of LOX, TG2, and AGEs in their role in cancer progression and fibrosis, it has been suggested that these 2 enzymes are potential targets for cancer therapy. For example, an inhibitory monoclonal antibody targeting LOXL2 resulted in a marked reduction in activated fibroblasts, desmoplasia, and endothelial cells, decreased production of growth factors and cytokines, and decreased transforming growth factor (TGF)-β pathway signaling in xenograft models of cancer as well as lung and liver fibrosis. 129 Similarly, inhibition of TG2 showed potential novel target for pulmonary fibrosis 84 as it decreases the profibrotic effector function of TG2.
LOX is increasingly considered a therapeutic target and there is potential in glaucoma treatment. There is an LOX cross-linking inhibitor—β-aminopropionitrile (BAPN), which has been shown to be effective in reducing ECM stiffness in artherosclerosis 130 and murine models of tumors and fibrosis.131,132 There may be potential for BAPN to be used to reduce TM stiffness. It was found that TM treatment with BAPN significantly increased outflow rates by 1.5- to 2-fold in normal human and porcine anterior chamber perfusion culture. 133
There is also potential for TG2 as therapeutic target. TG2 knockout mice exhibit reversal of disease phenotypes in neurodegenerative and chronic inflammatory disease models. 134 In relationship to glaucoma, Raychaudhuri et al. followed on their initial findings of higher expression of TG2 in transduced mice that results in an increase of IOP and decrease of outflow facility. 31 They subsequently tested the effect of TG2 knockout on IOP of TG2-floxed mice. 135 They found that TG2 knockout significantly decreases the IOP and in TGF-β2-induced OHT mice. The outflow facility following TG2 knockout is also improved in TGF-β2-induced eyes.
Alagebrium, which is also termed as ALT-117, breaks AGE cross-links and prevents accumulation of collagen and AGEs. It is has been found to improve arterial compliance of the cardiovascular system. 136 ALT-117 has also been found to improve the left ventricular stiffness in healthy older individuals. 137 Kiland et al. 138 investigated the effect of alagebrium on anterior segment morphology and ocular AGE and RAGE on aged rhesus monkey. Alagebrium did not have any major effect on IOP or outflow facility; however, they found formation of focal plaques within the juxtacanalicular network. Due to this, they concluded that AGE cross-link breaker is an unlikely approach for glaucoma therapy.
Conclusion
This review provides an understanding of the biomechanical properties of the cornea in relationship to glaucoma. Corneal, TM, and ONH stiffness occur with aging, findings that are exacerbated in glaucomatous change. The ECM plays an important role in the mechanical homeostasis of a tissue as it balances its structural constituents in response to stress loads. The ECM composition of the cornea, TM, and ONH is very similar, in particular, its collagen distribution. Abnormal collagen cross-linking results in tissue stiffening with resistance to degradation within the ECM. Collagen cross-linking proteins such as LOX, TG2, and AGEs have been implicated in glaucoma and its downstream effects may be seen as a risk factor for development and/or progression of glaucoma. Figure 3 summarizes the potential relationship between collagen cross-linking proteins and ocular/corneal stiffness, whereby the basis of the proposed mechanism is in context to the ECM alteration seen in the pathophysiology of cancer and fibrotic diseases.
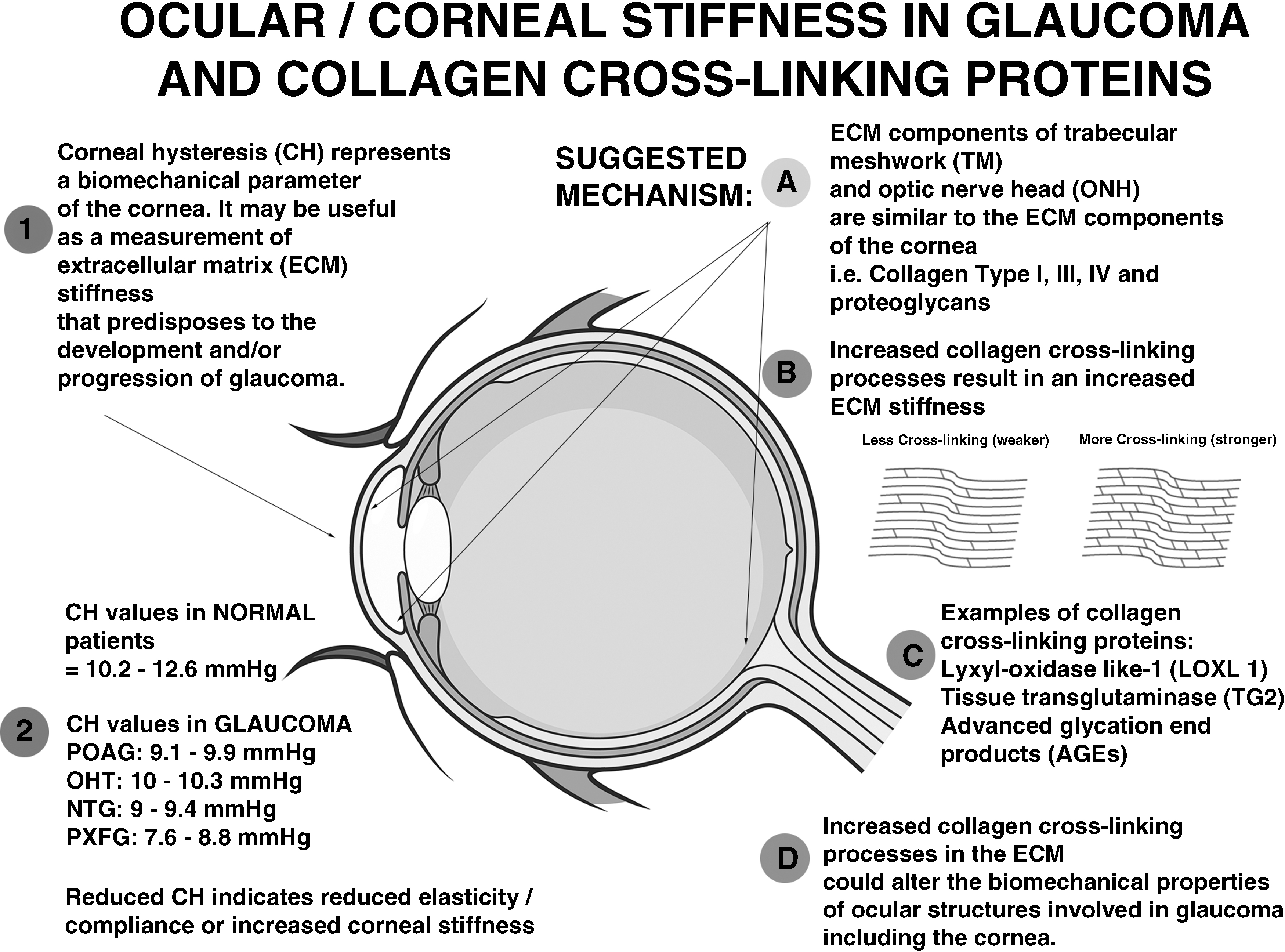
This infograph summarizes our review article that suggests the relationship between collagen cross-linking proteins and ocular/corneal stiffness.
The relationship between corneal biomechanical properties and collagen cross-linking provides a theoretical mechanism that may explain the progressive ocular stiffness process demonstrated in normal aging and is exaggerated in glaucoma. Further investigative studies are required to identify potential cross-linking biomarkers and therapeutic strategies in preventing the degenerative process of glaucoma.
Footnotes
Author Disclosure Statement
The authors declare they have no commercial or financial interests.
Funding Information
No funding was received for this article.