
Abstract
Purpose:
To compare the effectiveness of topical surfactant and 3% sodium chloride (NaCl) in the treatment of corneal edema occurring after cataract surgery.
Methods:
Ninety eyes of 90 patients with no corneal disease who underwent cataract surgery were included in the study. Thirty eyes without corneal edema comprised group 1. Patients with corneal edema were divided into two groups: those treated with 3% NaCl (group 2, 30 eyes) and those treated with surfactant drop (group 3, 30 eyes).
Results:
The mean age was 70.8 ± 6.6 years, with no significant age difference between the groups. Preoperatively, there was no significant difference in mean central corneal thickness (CCT) or mean endothelial cell count (ECC) among the groups (P = 0.999). On postoperative day 1, CCT was significantly lower in group 1 (P < 0.001) but did not differ between groups 2 and 3 (P = 0.999). There was no significant difference between groups in terms of ECC (P > 0.05). At postoperative day 7 and 14, CCT differed significantly between groups 1 and 2 (P < 0.001) and between groups 2 and 3 (P = 0.001), with no significant difference between groups 1 and 3 (P = 0.474). ECC was significantly higher in group 1 (P < 0.05), whereas there was no significant difference between groups 2 and 3 (P > 0.05).
Conclusion:
Topical pulmonary surfactant may be a more effective treatment option than 3% hypertonic NaCl for the treatment of corneal edema that develops after cataract surgery.
Introduction
Corneal edema is one of the most common complications after ocular surgeries. 1 It appears immediately after surgery and usually regresses within 2–4 weeks. 2 The incidence of persistent postoperative corneal edema was reported as 0.15% in a large-scale study. 3 The underlying cause of loss of corneal transparency after cataract surgery is usually endothelial decompensation due to surgical trauma. 4 The most important feature of the endothelium is its regulation of stromal hydration through the “pump-leak mechanism.” Corneal thickness is an indirect indicator of endothelial function. 5 Pump function generated by Na/K-ATPase is an active ATP- and oxygen-dependent process. 6
The primary function of pulmonary surfactant is to prevent alveolar collapse and overexpansion. These functions are made possible by the surface tension-lowering effect of surfactant. Pulmonary surfactant consists mainly of lipids and proteins. Most of the lipids in its structure are phospholipids (PL), with most (about 80%) of these PL being phosphatidylcholine (PC).7,8 PL can act as stimulator, inhibitor, and/or stabilizer on the Na/K-ATPase enzyme.9,10 Emr et al. 11 developed an experimental acute respiratory distress syndrome model in animal lungs and compared a group that underwent gene therapy with Na/K-ATPase/ENaC (epithelial sodium channels) plasmids with a control group and reported statistically significant decreases in alveolar edema and histopathological damage, significant increases in lung function and surfactant level (Surfactant Protein-B [SP-B] component), and improved survival in the gene therapy group. This confirms that the surfactant has a stimulating effect on Na/K-ATPase.
The tear film layer and surfactants have many similar properties. The tear film layer covers the surface of the corneal epithelium, whereas surfactant coats the epithelium of the lung alveoli. Both comprised a mixture of lipids and proteins, at varying proportions. Both are dynamic and of critical importance to the tissues they cover. They have a lipid layer on their air-facing surface. 8 Also, recent studies have shown that tear film layer contains surfactant proteins.12–14
Transcorneal oxygen therapy was shown to provide faster recovery from corneal edema after cataract surgery compared with conventional treatment and systemic oxygen therapy, and preserve more endothelial cells than conventional treatment. 15 In another study it was observed that postoperative corneal edema responded better in the group that received hyperbaric oxygen therapy (n = 12) compared with the control group (n = 21). 16
Several hypotheses underlie our belief that surfactant may be an effective agent in the treatment of corneal edema. (1) PL in the surfactant structure may enhance endothelial Na/K-ATPase function, which is important in pumping fluid from the corneal stroma to the anterior chamber, thereby supporting endothelial cells facing an increased workload compared with the preoperative state. (2) By reducing surface tension similar to its mechanism in the lungs, surfactant may facilitate fluid outflow from the corneal epithelium to the external environment. (3) By increasing corneal oxygenation, surfactant increases the amount of O2 that can reach the endothelium in corneal edema and may help meet the increased aerobic respiratory demand of these cells resulting from their reduced numbers.
In this study, we aimed to compare the effectiveness of surfactant and 3% sodium chloride (NaCl), one of the routinely used treatment regimens, in the treatment of corneal edema after cataract surgery. According to our literature searches, this study is the first trial of surfactant in the treatment of corneal edema.
Methods
All cataract patients were routinely examined for central corneal thickness (CCT) and endothelial cell count (ECC) before cataract surgery at a time interval of 6 months. A total of 101 patients, including 66 patients with corneal edema and 35 patients with similar characteristics in terms of age and gender without corneal edema, were included in the study. There were 35 patients in group 1, 33 patients in group 2, and 33 patients in group 3. The number of patients decreased to 30 in all groups, due to the patients who did not participate in day-7 control. The presence/absence of corneal edema was evaluated by the same clinician (T.A.) by biomicroscopic examination. The study included the patients who underwent phacoemulsification and foldable intraocular lens (IOL) implantation in the ophthalmology department of Van Yüzüncü Yıl University Faculty of Medicine. Approval for the study was obtained from Clinical Research Ethics Committee of the same center, informed consent forms were obtained from all included patients, and the study was conducted in accordance with the principles of the Declaration of Helsinki.
Patient selection
Inclusion criteria
Patients with senile cataract and clear cornea who underwent uncomplicated phacoemulsification and in-the-bag IOL implantation.
Exclusion criteria
Age <18 years
Corneal pathology (e.g., scar and dystrophy)
Cataract surgery performed with methods other than phacoemulsification (e.g., extracapsular or intracapsular cataract extraction)
Aphakia or other IOL implantations (e.g., anterior chamber-IOL, scleral-fixated, and iris-fixated)
Systemic collagen tissue disease that may predispose to corneal abnormalities; suspected or overt corneal ectasia (e.g., keratoconus and pellucid marginal degeneration)
Trauma-induced cataract
Active or chronic uveitis symptoms
Corneal endothelial disease (e.g., Fuchs' dystrophia)
Combined operations (e.g., phacoemulsification and trabeculectomy)
Intraoperative complications (e.g., posterior capsule tears, vitreous loss, and Descemet's membrane detachment).
Patient examination
Patients underwent a full ophthalmological examination, including best uncorrected and corrected visual acuity measurement, anterior and posterior segment examination, and intraocular pressure measurement, as well as IOL power calculation, CCT measurement with optical coherence tomography (OCT), and ECC using specular microscopy (SPM). Pachymetry and ECC were performed by the same experienced technician. Examinations were performed preoperatively and on postoperative days 1, 7, and 14. Pachymetry measurements were obtained using anterior segment OCT (Spectralis® OCT; Heidelberg Engineering, Heidelberg, Germany) and epithelial cell counts by SPM (Tomey, EM-300, Japan). The patient's head was secured to the OCT device (Spectralis OCT) and the patient was asked to look straight ahead. After establishing fixation, serial scans passing through the center of the cornea were acquired (resolution 10.84 μm/pixel on the x-axis and 3.87 μm/pixel on the z-axis). Data were collected from all images by the same doctor (T.A.). For ECC, values were obtained automatically from the squares of a grid centered on the cornea of the eye that was or will be operated.
Cataract surgery involved creating 2.4-mm incisions for anterior chamber access and performing phacoemulsification using cohesive and dispersive viscoelastic devices (Healon and Healon Endocoat, respectively; Abbott Lab, USA), followed by implantation of a foldable IOL (Alcon SA60AT; Alcon Lab., USA) in the capsule.
After cataract surgery, patients were prescribed topical steroid drops (Norsol, Bilim İlaç, Turkey) 6 times daily and topical antibiotic drops (Exocin, Allergan, Ireland) 6 times daily. Patients with complications other than corneal edema (Descemet's membrane detachment, IOL decentration, endophthalmia or suspected endophthalmia, presence of vitreous in the anterior chamber, and high IOP) on postoperative day 1 were excluded from the study. Patients who met the inclusion criteria and had clear cornea were selected as the control group. Patients who met the inclusion criteria and had corneal edema were randomly divided into the NaCl and surfactant groups. On day 1, patients in the NaCl group were given a sterile dropper bottle of 3% NaCl solution with instructions to use 5 times a day, whereas those in the surfactant group were provided surfactant drops to use 5 times a day. The surfactant suspension was prepared to a concentration of 30 mg/mL and packaged in sterile 2-mL dropper bottles by an experienced health care worker in accordance with the principles of cold chain storage. The surfactant used contained 99% PL (∼70% of the total PL content was PC) and 1% low molecular weight hydrophobic proteins (SP-B and surfactant protein-C [SP-C]) (Curosurf 120 mg/1.5 mL; Chiesi, Italy). We observed no side effects (neither ocular or systemic) related to surfactant use.
Statistics
Descriptive statistics were expressed as mean, standard deviation, minimum, and maximum for continuous variables and as number and percentage for categorical variables. One-way analysis of variance (ANOVA) was performed to compare group means of continuous variables. After ANOVA, the Bonferroni multiple comparison test was used to identify groups with significant differences. The level of statistical significance was set as 5% and IBM SPPS (version 17) statistics software was used for analyses.
Results
The mean age of patients included in the study was 70.82 ± 6.6 (58–87) years. There were no statistically significant differences in age between the groups (P > 0.05) (Table 1).
Comparison of Mean Age Among the Groups
a: Group 1, b: Group 2, c: Group 3.
Max, maximum; Min, minimum; n, number of patients; NaCl, sodium chloride; SD, standard deviation.
There were no statistically significant differences between the groups in terms of gender distribution, operated side, or number of patients with diabetes mellitus, hypertension, and glaucoma (P > 0.05) (Table 2).
Numbers of Patients with Diabetes, Hypertension, and Glaucoma and Distribution of Operated Eyes and Gender in the Groups
P value was >0.05 in all parameters.
Mean CCT measured the day before surgery did not differ significantly between the groups (P = 0.999 among all groups). On postoperative day 1, mean CCT was significantly lower in the control group compared with the other groups (P < 0.001) but did not differ significantly between the NaCl and surfactant groups (P = 0.999). At postoperative 1 week, mean CCT was significantly higher in the NaCl group compared with the control (P < 0.001) and surfactant (P = 0.001) groups, whereas the difference between the control and surfactant groups was insignificant (P = 0.474). At postoperative 2 weeks, the NaCl group still showed significantly higher mean CCT compared with the control group (P < 0.001) and the surfactant group (P = 0.021), and there was still no significant difference between the control and surfactant groups (P = 0.346).
There were no significant differences between the groups in terms of preoperative or postoperative day 1 ECC (P > 0.05). At postoperative 1 week, ECC was significantly higher in the control group compared with the NaCl (P = 0.006) and surfactant (P = 0.037) groups, whereas there was no significant difference between the NaCl and surfactant groups (P = 0.768). As with CCT, this relationship between the groups persisted in ECCs obtained at postoperative 2 weeks (control vs. NaCl P = 0.002; control vs. surfactant P = 0.003; NaCl vs. surfactant P = 0.979). Figures 1 and 2 show the change over time in the groups (CCT and ECC, respectively).

Change in CCT (in μm) in the groups over time (group 1, control group; group 2, NaCl group; group 3, surfactant group). CCT, central corneal thickness; NaCl, sodium chloride. Color images are available online.
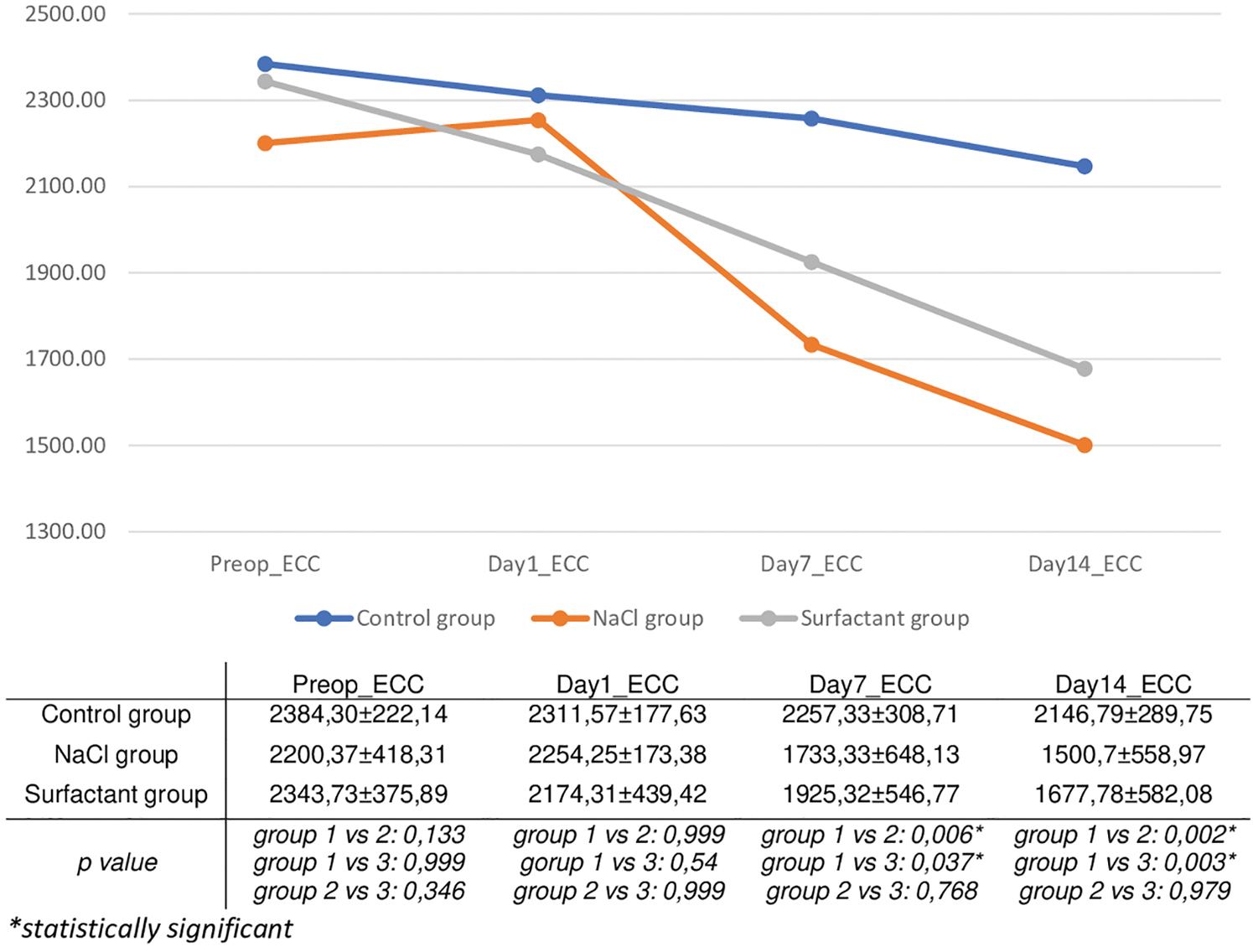
Change in ECC (in cells/mm2) in the groups over time (group 1, control group; group 2, NaCl group; group 3, surfactant group). ECC, endothelial cell count. Color images are available online.
Discussion
In this study, we did not include patients with a history of ocular trauma or endothelial abnormalities (which are major risk factors for postoperative corneal edema), patients with high postoperative IOP, or those with operative complications such as Descemet's membrane detachment and posterior capsule rupture. The mechanism most commonly used to treat corneal edema is making the tear film layer hyperosmolar to promote the flow of excess fluid in the cornea to the extracellular environment.17,18 These hypertonic agents are effective in one-third of cases of early-onset corneal edema, but sometimes treatment must be extended up to 3 months. 19 In our clinic, topical 3% hypertonic NaCl eye drop therapy is used to treat corneal edema, as in the NaCl group in this study because of commercially available 5% NaCl drops are more expensive and not easily available. In addition, according to our literature researches, there is no study showing that 5% NaCl solution is more effective than 3% NaCl solution in corneal edema.
Perone et al. 20 stated that after uncomplicated phacoemulsification compared with preoperative value, CCT increased by 8.4% at 2 h, 1.8% at postoperative day 4, and 0.1% at postoperative day 15. In another study of 13 eyes that underwent uncomplicated phacoemulsification, Salvi et al. 21 measured CCT at postoperative 1 h, 1 day, and 1 week and observed increases of 13.81%, 6.44%, and 0.57%, respectively. The control group in our study, which also included uncomplicated phacoemulsification patients, exhibited CCT increases of 6.31% at postoperative day 1 and 1.12% at postoperative week 1, but CCT decreased to preoperative levels after 2 weeks. Khripun et al. 22 administered 3% hypertonic NaCl (Ocusalin) to one group and no treatment for edema to the other group of patients with corneal edema after cataract surgery and observed CCT reductions of 18% in the NaCl-treated group and 12% in the untreated group at postoperative week 1. In our study, the decrease in CCT at postoperative week 1 and week 2 compared with day 1 was 10.21% and 15.4% in eyes treated with 3% NaCl and 19.8% and 21.1% in eyes treated with surfactant, respectively. In summary, at 1 and 2 weeks after cataract surgery, eyes that did not develop postoperative corneal edema and eyes that developed corneal edema and received topical surfactant drops had similar CCT, whereas eyes that developed corneal edema and were treated with topical NaCl had significantly higher CCT levels than both of the other groups.
In the literature, varying degrees of endothelial cell loss at postoperative 1 week have been reported and attributed to surgical trauma. 22 Factors affecting endothelial cell loss after cataract surgery include older age, ultrasound energy, surgical technique, duration of surgery, infusion volume, cataract hardness, and type of viscoelastic device used.23–26 Perone et al. recently reported that endothelial cell loss at postoperative day 15 and 30 was correlated with early postoperativecorneal edema. 20 Consistent with the literature, we observed a correlation in this study between CCT values at postoperative day 1 and change in ECC at postoperative week 2 compared with day 1 (Pearson correlation, r = 0.595). Endothelial cell losses compared with preoperative counts were 20.8% (n = 12) at week 1 and 28% (n = 11) at week 2 in eyes treated with 3% NaCl and similarly, 19.9% (n = 27) at week 1 and 27.2% (n = 29) at week 2 in eyes treated with surfactant. In addition, the ability to perform ECC with SPM can be considered an indicator that the cornea is clear and all corneal layers are smooth. ECCs could be performed with SPM at postoperative 1 week in 12 (36.4%) of the NaCl-treated eyes and 27 (81.8%) of the surfactant-treated eyes. At postoperative week 2, these rates increased to 11 eyes (50%) in the NaCl group and 29 eyes (93.5%) in the surfactant group.
Limitations of our study were that the operations were performed by multiple surgeons and cataract hardness and phacoemulsification energy used during surgery were unknown in some cases. In conclusion, this study is the first to evaluate the therapeutic use of surfactant on the ocular surface. Future research into the effect of surfactant on the ocular surface at the molecular level may provide a basis for its use in ocular surface pathologies.
Footnotes
Author Disclosure Statement
The authors declare that there is no conflict of interest regarding the publication of this article.
Funding Information
The authors received no funding for this study.