
Abstract
Purpose:
To compare the clinical effects of postoperative versus perioperative injection of anti-vascular endothelial growth factor (VEGF) drugs before and after pars plana vitrectomy (PPV) in patients with vitreous hemorrhage secondary to polypoidal choroidal vasculopathy (PCV).
Methods:
This was a retrospective study of patients who underwent PPV due to vitreous hemorrhage between October 2013 and June 2019 at Ningbo Eye Hospital. The patients who underwent PPV surgery due to PCV-secondary vitreous hemorrhage were included. The primary outcome was the changes in best-corrected visual acuity. The secondary outcome was the central macular thickness.
Results:
Compared with the postoperative group (n = 20), the perioperative group (n = 18) showed a smaller number of postoperative anti-VEGF injections (5.1 ± 0.8 vs. 8.0 ± 1.5, P < 0.05) and lower frequencies of early hyphema (5.6% vs. 30.0%, P < 0.05), and recurrent vitreous hemorrhage (11.1% vs. 30.0%, P < 0.05). The logarithm of minimal angle resolution (LogMAR) was smaller in the perioperative group compared with the postoperative group at 1 week, 1 month, and 3 months after PPV (P < 0.05), but there were no differences thereafter. Compared with the postoperative group, the perioperative group had thinner fovea at 1 week, 1 month, and 3 months (P < 0.05), but the differences disappeared after 3 months.
Conclusion:
In patients with PCV and vitreous hemorrhage, compared with postoperative anti-VEGF, perioperative anti-VEGF could reduce the difficulty of surgery and reduce the occurrence of postoperative complications, but there were no differences in long-term vision and macular thickness after surgery.
Introduction
Polypoidal choroidal vasculopathy (PCV) is a variant of age-related macular degeneration (AMD) that can account for 50% of neovascular AMD cases in persons of Asian descent compared with 8%–13% in Caucasians.1,2 Vitreous hemorrhage is a common complication of PCV in patients >60 years of age. Uyama et al. 3 divided PCV into 2 types: exudative and hemorrhagic. The exudative type manifests as serous retinal pigment epithelium (RPE) detachment, whereas the hemorrhagic type manifests as hemorrhagic RPE detachment. Sudden subretinal hemorrhage in the macular area causes a sudden loss of vision in the affected eye. Large hemorrhage under the retina can cause vitreous hemorrhage.
Studies in China showed that 4.5% of PCV patients could present with vitreous hemorrhage at the first diagnosis, and the number of cases with vitreous hemorrhage can be as high as 19.9%.4–8 A large amount of vitreous hemorrhage is difficult to absorb.
PCV with wet AMD (wAMD) is more likely to cause vitreous hemorrhage. 2 Although vitreous hemorrhage in wAMD patients may be absorbed by itself, such a phenomenon has not been reported in vitreous hemorrhage combined with PCV. A large amount of thick subretinal hemorrhage or vitreous hemorrhage can cause a proliferative reaction in the vitreous body.9–11
At present, the commonly used treatments for PCV include intravitreal injection of anti-vascular endothelial growth factor (VEGF) drugs (ranibizumab, aflibercept, and conbercept) 4 and photodynamic therapy (PDT).1,12,13 Vitrectomy can not only remove the vitreous hemorrhage but also identify the cause of the vitreous hemorrhage, which is an effective measure for the treatment of vitreous hemorrhage. If the hemorrhage is not cleared in time, it is very likely to cause proliferative vitreoretinopathy, and it can also cause traction on the site of the original hemorrhage. Retinal detachment can cause irreversible visual damage and even blindness in severe cases.
For PCV accompanied by vitreous hemorrhage and hemorrhagic retinal detachment, pars plana vitrectomy (PPV) is usually performed to remove vitreous hemorrhage. 14 PPV can improve the visual outcomes of patients with PCV and subretinal hemorrhage. 7 Anti-VEGF drugs and PDT can be used as adjuvant treatment after PPV; still, the results indicate that this strategy can decrease,10,15 or increased 4 the risk of hemorrhage. Pneumatic displacement of the blood clot combined with anti-VEGF can also improve the visual outcomes. 9 One study examined the use of anti-VEGF after PPV in 16 eyes and reported no reactivation and improved visual acuity during follow-up in 7 eyes. 16
Still, the exact impact of the use of anti-VEGF drugs before and after PPV in patients with PCV and vitreous hemorrhage is poorly known. Therefore, this study aimed to compare the clinical effects and complications of injection of anti-VEGF drugs before and after PPV in patients with PCV and vitreous hemorrhage.
Methods
Study design and participants
This was a nonrandomized retrospective comparative study of patients who underwent PPV due to PCV-induced vitreous hemorrhage between October 2013 and June 2019 at Ningbo Eye Hospital. This study was in compliance with the Declaration of Helsinki and was approved by the Ethics Committee of Ningbo Eye Hospital. The need for individual consent was waived by the committee.
The inclusion criteria were (1) preoperatively diagnosed with vitreous hemorrhage with indications for PPV, that is, nonclearing vitreous hemorrhage using conservative treatments, (2) PCV was confirmed by postoperative optical coherence tomography (OCT) or indocyanine green (ICG) angiography (ICGA), (3) anti-VEGF treatment was given based on the 3+PRN regimen after PPV, (4) PDT treatment was not performed before surgery, and (5) postoperative follow-up time was at least 6 months. The exclusion criteria were (1) presence of retinal choroid pathological changes other than PCV, (2) diabetic retinopathy, (3) retinal vein occlusion, (4) pathological myopia, (5) angioid streaks of the fundus, or (6) other choroidal neovascularization diseases.
The diagnostic criteria for PCV were based on those developed by the Japanese PCV Research Group 3 : (1) color fundus photography revealing raised orange or red lesions; and (2) ICGA examinations showed typical polypoidal lesions, that is: (i) multiple polypoidal dilated lesions in the abnormal branched choroidal vascular network and its ending; or (ii) scattered polypoidal choroidal vascular dilated lesion, but no obvious branched choroidal blood vessels.
Grouping
The patients were grouped according to their timing of PPV and anti-VEGF drugs. In the perioperative group, intravitreal injection of anti-VEGF drugs was performed at least once within 3 months before surgery, and anti-VEGF treatment was continued according to the 3+PRN regimen 2 weeks after PPV. In the postoperative group, intravitreal injection of anti-VEGF drugs was started according to the 3+PRN regimen 2 weeks after PPV.
Visual acuity
Best-corrected visual acuity (BCVA) was measured using an international standard visual acuity chart. For statistical analysis, BCVA was converted to the logarithm of minimal angle resolution (LogMAR). LogMAR = log (1/decimal visual acuity). The exponent was converted to 1.86, with the manual conversion of 2.28 and the light perception conversion of 2.84.
Pars plana vitrectomy
PPV was performed routinely in all patients. All patients were made fully mydriatic before surgery with Mydrin P and 1% atropine eye drops. Retrobulbar anesthesia was performed using 2% lidocaine and 0.75% bupivacaine. All surgeries were performed by the same surgeon (Dr. Q.Y.Y.) using the Stellaris PC Vitrectomy System (Bausch and Lomb, Inc., Rochester, NY). All patients underwent conventional 23G 3-channel PPV, and the 23G Bausch & Lomb puncture cannula system (Bausch and Lomb) was used to puncture at 3.5–4.0 mm away from the posterior corneoscleral region. The puncture cannula was used to puncture in the direction of the center of the eyeball and then into the eyeball at an angle of about 70° to achieve incision occlusion. The puncture cannula in the infratemporal region was used for water, and the puncture cannulas in the supra-nasal and supratemporal regions were used as PPV and fiber-optic heads for insertion. The fundus observation during PPV was performed using the Resight noncontact wide-angle viewing system.
The surgical procedures first included removal of the central vitreous body and hemorrhage and then removing the peripheral vitreous bodies and hemorrhage. A posterior vitreous detachment was performed to remove the posterior vitreous cortex. If a cataract was present, combined phacoemulsification cataract extraction and intraocular lens implantation were performed during surgery. If the subretinal hemorrhage was thick or was accompanied by an old hemorrhagic clot, which was difficult to absorb, a small incision of the peripheral retina was performed to remove part of the subretinal hemorrhagic and clots.
In both groups, a flute needle with a silicone tip was used to control bleeding during surgery. An endolaser was used to treat the peripheral retinal incision. If it was complicated with retinal detachment, laser treatment of the peripheral retinal incision was performed after pressing the retina with perfluorocarbon, followed by a liquid–gas exchange. Air, C3F8, or silicone oil was used for intraocular tamponade, with a viscosity of silicone oil being 5,000 cs. At the end of the surgery, the microcannulas were removed, and if leakage of the puncture was found, an 8-0 polyglactin suture was used for suturing. At the end of the procedure, dexamethasone was injected into the inferior subconjunctival space. Topical antibiotics and steroids were prescribed for 1 month. Patients who had gas or silicone oil tamponade were instructed to remain face down for 7–10 days.
Postoperative management
During follow-up, antiglaucoma eyedrops such as β-blockers, carbonic anhydrase inhibitors, or prostaglandin analogs were prescribed when intraocular pressure (IOP) was >21 mmHg. Re-examinations of BCVA, slit-lamp microscope, IOP, color fundus photography, and OCT were performed 1 week after surgery. If there was no history of allergy, fundus fluorescein angiography and ICGA were performed. Anti-VEGF treatment of the affected eyes was conducted 2 weeks after surgery according to the 3+PRN regimen. Re-examinations of BCVA, slit-lamp microscope, IOP, B-mode ultrasound, color fundus photography, and OCT were performed monthly within 6 months after surgery. The criteria for reinjection were (1) vision loss ≥ Early Treatment Diabetic Retinopathy Study (ETDRS) 5 letters and OCT showing macular effusion, (2) OCT scans in any of the 6 directions showing an increase in central retinal thickness >100 μm, and (3) new macular hemorrhage.
Intravitreal injection of anti-VEGF drugs
Ranibizumab intraocular injection (Novartis Pharma Schweiz AG, registration number: S20100025, specifications: 10 mg/mL, 0.2 mL/bottle) and conbercept intraocular injection (Chengdu Kanghong Biotechnology Co., Ltd., CN20130483, 10 mg/mL, 0.2 mL/injection) were used. All patients were treated with levofloxacin hydrochloride eye drops 3 times/day for 3 days. Routine disinfection, surface disinfection with oxybuprocaine hydrochloride, anesthesia, and eyelids opening were performed; disinfection of the eyeballs was made with 5% povidone-iodine eye drops. After 90 s, the cornea and bulbar conjunctival sac were washed with normal saline. Then, 0.05 mL of ranibizumab or conbercept was extracted with a 1-mL empty needle. The needle was inserted 4 mm behind the corneal limbus in the infratemporal region, and the drug was slowly injected into the vitreous cavity. After removing the needle, the wound was pressed with a sterile wet cotton swab for 1–2 min. Levofloxacin eye ointment was applied to dress the affected eye.
Outcomes
The primary outcome was the changes in BCVA. The secondary outcome was the central macular thickness.
Statistical analysis
Continuous data were presented using means ± standard deviations and ranges and analyzed using the Wilcoxon rank-sum test or the independent Student's t-test, according to the results of the Kolmogorov–Smirnov test for normal distribution. Categorical variables were presented as numbers (percentages) and analyzed using the Fisher's exact test. P values <0.05 were defined as statistically significant. Statistical analyses were performed using SPSS 20.0 for Mac (IBM, Armonk, NY). For patients with bilateral lesions, only 1 eye in each patient was randomly selected for analysis.
Results
Characteristics of the patients
In the perioperative group, there were 18 cases (18 eyes), including 12 males (12 eyes) and 6 females (6 eyes). In the postoperative group, there were 20 cases (20 eyes), including 14 males (14 eyes) and 6 females (6 eyes). The preoperative baseline data are presented in Table 1. There were no significant differences in the demographic characteristics, course of the disease, preoperative BCVA, IOP, lens, results of B-ultrasonography and fundus examination, and retinal detachment between the 2 groups (all P > 0.05). In the perioperative group, the mean number of injections of anti-VEGF in the first 3 months of the perioperative period was 1.7 ± 1.0. The mean time from the last anti-VEGF injection to surgery was 20.9 ± 7.6 days.
Characteristics of the Patients
BCVA, best-corrected visual acuity; IOP, intraocular pressure; LogMAR, logarithm of minimal angle resolution; VEGF, vascular endothelial growth factor.
Surgical procedures and intraoperative complications
Table 2 presents the characteristics of the procedures and the complications. Compared with the postoperative group, the perioperative group showed a shorter surgical time (30.7 ± 6.9 vs. 49.2 ± 14.3 min, P < 0.001), lower frequency of retinotomy (5.6% vs. 35.0%, P < 0.05), lower frequency of perfluorocarbon use (11.1% vs. 35.0%, P < 0.05), and lower frequency of tamponade use, irrespective of the method (P < 0.05). There were no differences regarding cataract surgery, iatrogenic tear, and massive retinal hemorrhage.
Postoperative Conditions and Complications
Postoperative complications
Table 3 presents the postoperative status and complications. Compared with the postoperative group, the perioperative group showed smaller number of postoperative anti-VEGF injections (5.1 ± 0.8 vs. 8.0 ± 1.5, P < 0.05) and lower frequencies of early hyphema (1–7 days; 5.6% vs. 30.0%, P < 0.05), recurrent vitreous hemorrhage (11.1% vs. 30.0%, P < 0.05), second surgery (11.1% vs. 25.0%, P < 0.05), and postoperative PDT (11.1% vs. 30.0%, P < 0.05). There were no differences in choroid detachment, retinal detachment, RPE tear, neovascular glaucoma, and macular scar (all P > 0.05). A second operation was due to a large amount of anterior chamber hemorrhage or vitreous hemorrhage that could not be absorbed or retinal detachment.
Follow-Up
NVG, neovascular glaucoma PDT, photodynamic therapy; RPE, retinal pigment epithelium; VH, vitreous hemorrhage.
Changes in BCVA
The changes in BCVA in the 2 groups are presented in Fig. 1. There were no differences in LogMAR between the 2 groups before surgery (P = 0.512). LogMAR was smaller in the perioperative group compared with the postoperative group at 1 week, 1 month, and 3 months after PPV (all P < 0.05), but there were no differences at 6 months (P = 0.574) and at the last follow-up (P = 0.482).
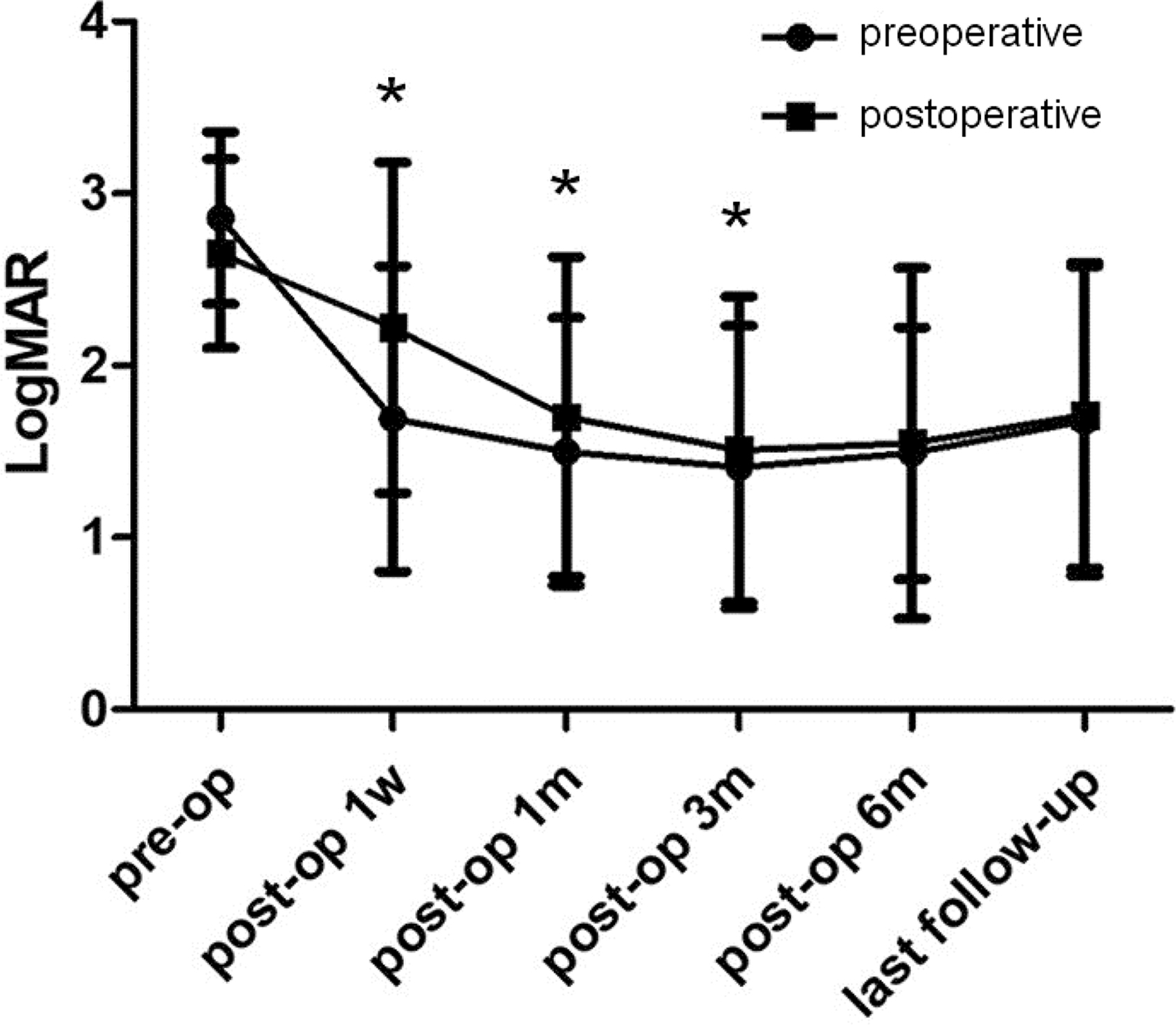
Postoperative BCVA of 2 groups (perioperative group vs. postoperative group). *P < 0.05. BCVA, best-corrected visual acuity.
Postoperative foveal thickness
The foveal thickness after PPV is presented in Fig. 2. Compared with the postoperative group, the perioperative group had thinner fovea at 1 week, 1 month, and 3 months (all P < 0.05), but the differences disappeared at 6 months (P = 0.753) and last follow-up (P = 0.618).
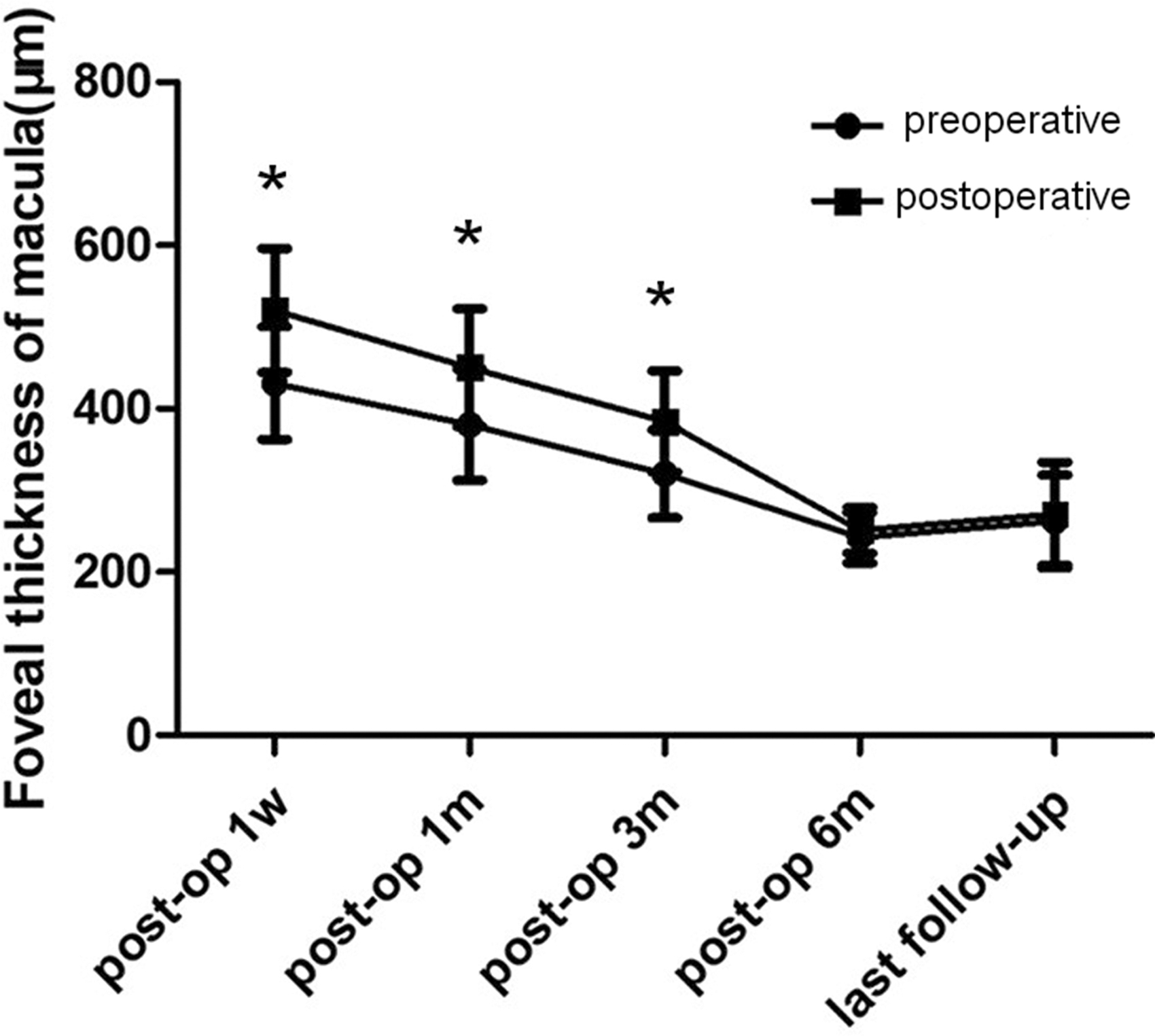
The postoperative foveal thickness of macula by OCT. (perioperative group vs. postoperative group). *P < 0.05. OCT, optical coherence tomography.
Discussion
The exact impact of the use of anti-VEGF drugs before and after PPV in patients with PCV and vitreous hemorrhage is poorly known. This study aimed to compare the clinical effects and complications of injection of anti-VEGF drugs before and after PPV in patients with PCV and vitreous hemorrhage. The results suggest that in patients with PCV and vitreous hemorrhage, the clinical benefits of anti-VEGF before and after PPV were better than for anti-VEGF after PPV, suggesting that anti-VEGF drugs could be first administrated for clinically suspicious or confirmed vitreous hemorrhage caused by PCV.
Vitreous hemorrhage is a common complication in patients with PCV.3,5,17 Uyama et al. classified PCV into 2 types: exudative and hemorrhagic type. The exudative type manifests as serous RPE detachment, and the hemorrhagic type is characterized by hemorrhagic RPE detachment and subretinal hemorrhage in the macula. 3 Massive vitreous hemorrhage is difficult to absorb in patients with PCV. 8 PCV is more prone to vitreous hemorrhage than wAMD. 18 Massive thick subretinal hemorrhage or vitreous hemorrhage can result in vitreous hyperplasia. PPV can remove not only the vitreous hemorrhage and neovascular membrane but also determine the cause of the vitreous hemorrhage. Presently, most authors believe that PPV should be performed as early as possible to remove hemorrhage in these patients.6,19
Studies demonstrated that the preoperative application of anti-VEGF drugs for diabetic retinopathy could reduce intraoperative bleeding and adhesion of proliferative membrane, shorten surgery time, alleviate iatrogenic injury, lower the risk of postoperative rebleeding, and relieve macular edema and iris neovascularization, thereby ensuring reduction rate and visual prognosis.20–22 In this study, the preoperative use of anti-VEGF drugs was associated with a shorter surgical time and lower frequencies of retinotomy, perfluorocarbon use, tamponade use, early hyphema, recurrent vitreous hemorrhage, a second surgery, and postoperative PDT. Those results are supported by the results observed with the preoperative use of such drugs in diabetic retinopathy.20–22 Although in a small number of patients who received preoperative bevacizumab, similar results were observed in patients with PCV. 7 Therefore, the perioperative use of anti-VEGF drugs can decrease the complications associated with PPV in patients with PCV-caused vitreous hemorrhage.
In this study, visual acuity improved in the 2 groups; this improvement was more important in the patients who received preoperative anti-VEGF drugs than in those who did not, but the difference disappeared at 6 months. This is supported by Lin et al., 7 who also observed that preoperative bevacizumab was not associated with the final BCVA, but they did not examine visual acuity as early as in this study. Lee et al. 23 showed that the use of aflibercept, without PPV, was able by itself to manage uncomplicated PCV. Therefore, using anti-VEGF agents, followed by PPV and continuing the anti-VEGF agent as needed, could be an option to improve the outcomes of patients with PCV and vitreous hemorrhage.
Regarding foveal thickness, anti-VEGF agents can decrease central foveal thickness in patients with PCV. 24 In this study, both strategies decreased foveal thickness, but as for visual acuity, the improvement was more important in the perioperative group than in the postoperative group, and the difference disappeared at 6 months. A study in diabetic retinopathy also reported a lack of difference between the perioperative and postoperative use of conbercept, but they did not assess foveal thickness early after PPV. 21 Anti-VEGF drugs can reduce the thickness of the fovea in patients with PCV.25,26 Mechanical removal of thick submacular hemorrhage alone does indeed lead to a reduction in the thickness of the fovea. Still, the 2 groups underwent postoperative OCT based on the actual situation and collected statistics; there were cases of mechanical removal of submacular hemorrhage between the 2 groups.
The results showed that there were no significant differences in visual acuity and OCT results after 3 months between the 2 groups, but the perioperative strategy could reduce the difficulty of surgery and improved the short-term results, which should also be worthy of clinical reference.
Limitations
This study has limitations. The sample size was small and from a single center. The retrospective nature of the study limited data that could be analyzed to those in the medical charts. Nevertheless, this study provides some bases for the design of a randomized controlled trial.
Conclusions
In patients with PCV and vitreous hemorrhage, compared with postoperative anti-VEGF, perioperative anti-VEGF could reduce the difficulty of surgery and reduce the occurrence of postoperative complications, but there were no differences in long-term vision and macular thickness after PPV.
Ethics Approval and Consent to Participate
This study was in compliance with the Declaration of Helsinki and was approved by the Ethics Committee of Ningbo Eye Hospital. The need for individual consent was waived by the committee.
Footnotes
Authors' Contributions
Q.Y.Y. substantially contributed to conception or design, drafted the article for important content, critically revised the article for important intellectual content, and gave final approval. L.H.Q., J.H.M., and X.X.F. contributed to acquisition, analysis, or interpretation of data. L.S.C. substantially contributed to conception or design. Q.G., S.S.W., W.D.L., and Y.Y.W. drafted the article for important content.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study is supported by the Natural Science Foundation of Ningbo City (2019A610351) and by the Projects of medical and health technology development program in Zhejiang province (2018KY735); the Natural Science Foundation of Guangdong Province (2018A030313935).