
Abstract
Purpose:
To evaluate 5-year reactivation after ranibizumab or aflibercept treatment for neovascular age-related macular degeneration (AMD) and polypoidal choroidal vasculopathy (PCV).
Methods:
This retrospective study included 192 patients (192 eyes) who had been diagnosed with neovascular AMD or PCV and treated with ranibizumab or aflibercept. The incidence and timing of lesion reactivation during the 5-year follow-up period were evaluated, and the factors associated with reactivation were also investigated.
Results:
During the follow-up period, lesion reactivation was noted in 156 patients (81.3%) at a mean of 9.5 ± 10.5 months after the third antivascular endothelial growth factor injection. The incidence of reactivation was 59.9% during the first 12 months, 33.7% during ≥12 and <24 months, 11.8% during >24 and ≤36 months, 15.5% during >36 and ≤48 months, and 5.3% during >48 and ≤60 months. There was a significant difference in the incidence among the 5 periods (P < 0.001). The proportion of PCV was significantly higher in patients experiencing reactivation (51.9%) than in those who did not (30.6%) (P = 0.021).
Conclusions:
During the 5-year follow-up, lesion reactivation was noted in approximately four-fifths of the patients. The incidence of lesion reactivation was highest during the first 12 months and decreased thereafter. The incidence was higher in patients with PCV than in those with neovascular AMD, especially after 12 months.
Introduction
Antivascular endothelial growth factor (VEGF) is an effective treatment for neovascular age-related macular degeneration (AMD) and polypoidal choroidal vasculopathy (PCV).1–3 Since the duration of efficacy of anti-VEGF agents is usually limited to several months, 4 long-term continuous anti-VEGF injections are generally necessary to maintain vision.5–7 Discontinuation of treatment, despite active disease, often leads to profound vision loss. 8
However, in some patients, reactivation of the lesion, which is characterized by reaccumulation of subretinal fluid (SRF)/intraretinal fluid (IRF) on optical coherence tomography (OCT), or development of retinal hemorrhage is not noted after initial treatment.9–14 It is unclear whether this phenomenon is mainly derived from the nature of the disease itself or the prolonged effect of anti-VEGF. In previous studies, various factors and morphologic biomarkers, including age, sex, polyp configuration, size of pigment epithelial detachment (PED), and development of retinal pigment epithelial (RPE) atrophy, were found to be associated with non-reactivation.11–13
Data regarding the incidence, timing, and factors associated with reactivation are important because they can help determine appropriate treatment regimens, such as “as-needed” and “treat-and-extend.” In addition, it can also be utilized when discussing patients for their prognosis as well as determining follow-up schedule. To date, several studies have focused on this subject. However, the follow-up period was mainly limited to 2 years in these studies,11–14 and long-term reactivation after initial treatment remains to be elucidated.
In this study, the 5-year long-term incidence and timing of reactivation after initial anti-VEGF treatment were evaluated in patients with neovascular AMD and PCV. Incidence of lesion reactivation according to the follow-up period and factors and morphologic biomarkers predictive of non-reactivation were also investigated.
Methods
This retrospective observational study was conducted in a single center (Kim's Eye Hospital, Seoul, South Korea). The study was approved by the Institutional Review Board of Kim's Eye Hospital and was conducted following the tenets of the Declaration of Helsinki.
Patients
This study included treatment-naive patients diagnosed with neovascular AMD or PCV between January 2014 and October 2015. Additional inclusion criteria were as follows: (1) initially treated with 3 loading injections of ranibizumab (0.5 mg/0.05 mL of Lucentis®; Genentech, Inc., San Francisco, CA) or aflibercept (2.0 mg/0.05 mL of Eylea®; Regeneron, Tarrytown, NY); (2) follow-up period at least 5 years; and (3) available indocyanine-green angiography (ICGA) result. The exclusion criteria were as follows: (1) residual intraretinal/SRF after initial treatment; (2) treatment using a treat-and-extend (TAE) regimen before the first reactivation; (3) did not visit the hospital for more than 10 months; and (4) history of vitreoretinal surgery or glaucoma surgery. An eye with prior treatment was included when both eyes met the eligibility criteria.
Treatment
Patients were initially treated with 3 loading injections of intravitreal ranibizumab or aflibercept. After initial treatment, regular follow-ups were performed without additional treatment until lesion reactivation was noted. Lesion reactivation was defined as the reaccumulation of SRF/IRF, or development of subretinal/intraretinal hemorrhage. Clinical examination results, OCT images, and fundus photographs were reviewed to identify reactivation. The presence of outer retinal tubulation or cystoid macular degeneration alone was not considered to be a lesion reactivation. After initial treatment, the patients were scheduled to follow-up every 1–2 months. During the first year, the follow-up interval was extended to 3 months at the discretion of the treating physician. In patients without lesion reactivation for a long period, the follow-up interval was extended up to 4–6 months.
Outcome measures
The incidence and timing of the first reactivation during the 5-year follow-up period after initial diagnosis were evaluated. The entire follow-up period was divided into 5 periods: <12 months, ≥12 and <24 months, >24 and ≤36 months, >36 and ≤48 months, and >48 and ≤60 months. The incidence of lesion reactivation was estimated during each period. In addition, an evaluation of whether there was a difference in the reactivation rate among the different periods and the incidence of lesion reactivation among patients who did not experience activation was analyzed. Patients were divided into 2 groups according to the development of reactivation: the reactivation group versus the non-reactivation group.
The following baseline parameters were compared between the 2 groups: age (<70 years vs. ≥70 years), sex, diabetes mellitus, hypertension, lens status (phakia vs. pseudophakia), type of neovascularization (neovascular AMD vs. PCV), type of fluid (SRF alone vs. IRF alone vs. other types of fluid), the presence of epiretinal membrane (ERM) or vitreomacular traction, foveal involvement of the fluid, best-corrected visual acuity (BCVA) at diagnosis (logarithm of the minimal angle of resolution [logMAR] 0.4 [Snellen equivalents = 20/40] or better vs. worse than logMAR 0.4), and type of anti-VEGF agent (ranibizumab vs. aflibercept). Multivariate analysis was also performed using the aforementioned parameters to identify factors and morphologic biomarkers associated with reactivation after initial treatment. In the non-reactivation group, the incidence of RPE atrophy was compared between patients with neovascular AMD and PCV. RPE atrophy was considered present when complete RPE and outer retinal atrophy 15 were noted on OCT images.
The BCVA measurements were collected at diagnosis and 1, 2, 3, and 5 years. When BCVA was not measured at the exact time point, the values measured at the closest time point were used for analysis. The degree of changes in BCVA during the 5-year period was compared between the reactivation and non-reactivation groups. In addition, the VAs measured before the reactivation, when the reactivation was noted, and after treatment for the reactivation were obtained. The proportion of patients who failed to completely recover the pre-reactivation VA after the reactivation was estimated. Since BCVA was measured at all the 3 time points in only select patients, naked eye VA was used for analysis in most patients, and BCVA was used only when measured at all the 3 time points.
Statistical analyses
The data are presented as mean ± standard deviation or as a number (percentage), wherever applicable. The BCVA was converted to logMAR values for analysis. Statistical analyses were performed using a commercially available software package (SPSS version 18.0; IBM Corporation, Armonk, NY). Comparisons between 2 different groups were performed using the chi-square test with or without linear-by-linear association or Fisher's exact test. Multivariate analysis was performed using binary logistic regression analysis. A P value of <0.05 was considered statistically significant.
Results
During the study period, 670 patients were diagnosed with treatment-naive neovascular AMD and PCV and were treated with ranibizumab and aflibercept (Fig. 1). Among them, 302 patients completed the 5-year follow-up. Among the 302 patients, 110 were excluded for the following reasons: lack of ICGA results = 39, residual intraretinal/SRF after initial treatment = 47, treated with TAE regimen before the first reactivation = 14, did not visit the hospital for more than 10 months = 6, and history of vitreoretinal surgery or glaucoma surgery = 4. A total of 192 patients (192 eyes) were included in the study. Table 1 summarizes the baseline characteristics of the included patients.

Study flowchart showing the number of excluded patients and reasons for exclusion. AMD, age-related macular degeneration; ICGA, indocyanine-green angiography; PCV, polypoidal choroidal vasculopathy; TAE, treat-and-extend.
Baseline Characteristics of the Included Patients (n = 192)
Data are presented as mean ± standard deviation or number (percentage) when applicable.
Snellen equivalents.
AMD, age-related macular degeneration; BCVA, best-corrected visual acuity; PCV, polypoidal choroidal vasculopathy; IRF, intraretinal fluid; logMAR, logarithm of the minimal angle of resolution; SRF, subretinal fluid.
Ranibizumab was used as the initial treatment in 128 patients (66.7%), whereas aflibercept was used in the remaining 64 patients (33.3%). During the follow-up period, lesion reactivation was noted in 156 patients (81.3%) at a mean of 9.5 ± 10.5 months after the third anti-VEGF injection (Fig. 2). Table 2 summarizes the incidence of reactivation according to the follow-up period. The incidence of reactivation was 59.9% during the first 12 months, 13.5% during ≥12 and <24 months, 3.1% during >24 and ≤36 months, 3.6% during >36 and ≤48 months, and 1.0% during >48 and ≤60 months. There was a significant difference in the incidence among the 5 periods (P < 0.001). The incidence of lesion reactivation among patients who did not experience activation was 59.9% during the first 12 months, 33.7% during ≥12 and <24 months, 11.8% during >24 and ≤36 months, 15.5% during >36 and ≤48 months, and 5.3% during >48 and ≤60 months. There was a significant difference in the incidence among the 5 periods (P < 0.001).
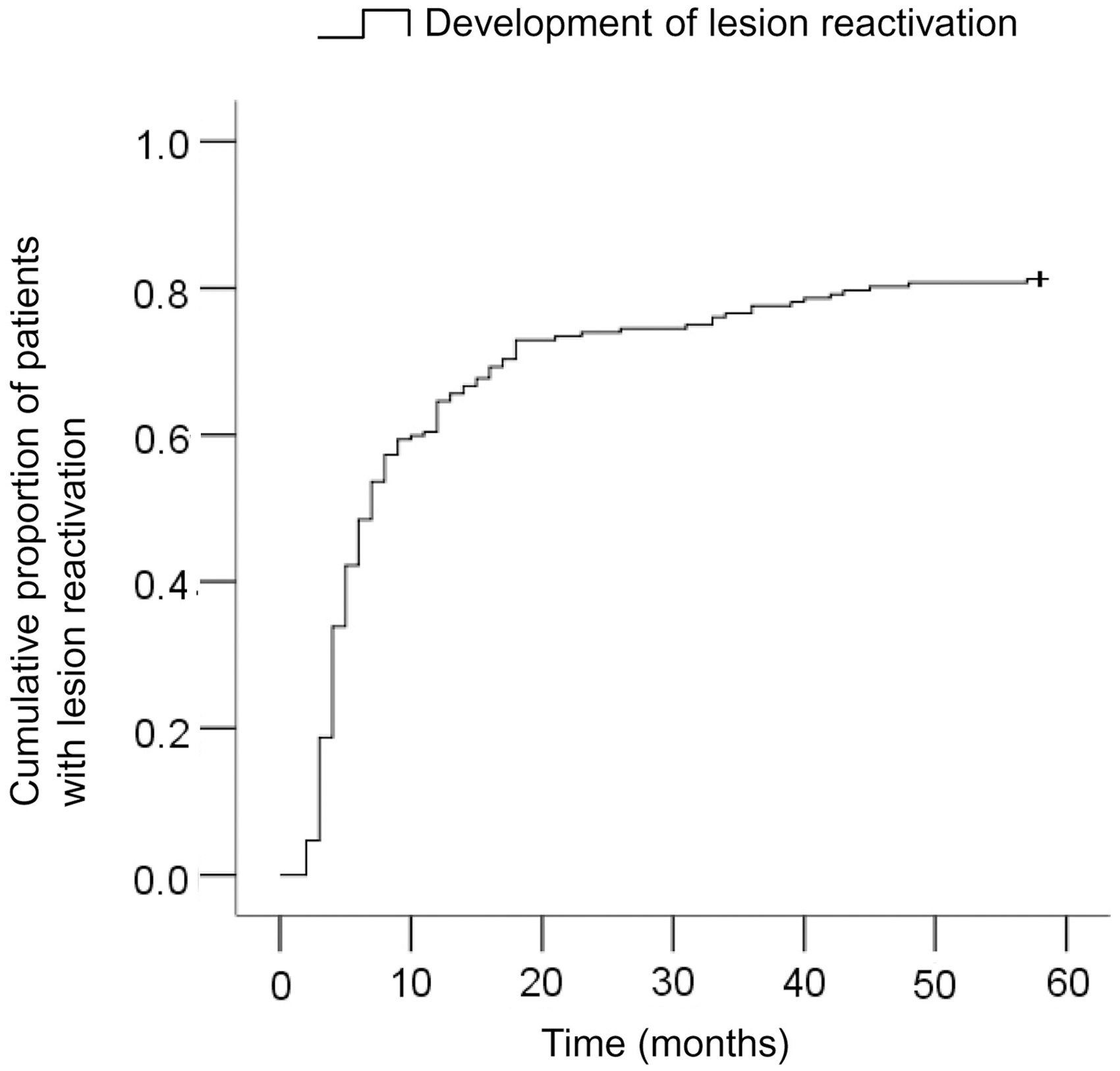
Cumulative proportion of patients with lesion reactivation, according to time after the third anti-vascular endothelial growth factor injection.
Incidence of Lesion Reactivation According to the Follow-Up Period
Chi-square test with linear-by-linear association.
Among the 192 patients included in the study, cataract surgery was performed during the follow-up period in 15 patients (7.8%; 12 in the reactivation group and 3 in the non-reactivation group). The mean period between the diagnosis and cataract surgery in the reactivation group was 38.8 ± 11.3 months. All the cataract surgeries were performed after the first reactivation.
One hundred fifty-six patients (81.3%) were included in the reactivation group, and the remaining 36 patients (18.8%) were included in the non-reactivation group. Figure 3 shows a representative case of a patient who did not experience lesion reactivation during the 5-year follow-up. When comparing the reactivation and non-reactivation groups (Table 3), there was a significant difference in the type of neovascularization and BCVA between the 2 groups. The proportion of PCV was significantly higher in the reactivation group than in the non-reactivation group (51.9% vs. 30.6%, P = 0.021). There was no difference in age (P = 0.517), sex (P = 0.378), diabetes mellitus (P = 0.200), hypertension (P = 0.471), type of fluid (P = 0.744), the presence of ERM or vitreomacular traction (P = 1.000), foveal involvement of the fluid (P = 0.771), BCVA (P = 0.219), and type of anti-VEGF agent (P = 0.433) between the 2 groups. In a multivariate analysis (Table 4), the type of neovascularization was found to be the only parameter associated with reactivation (P = 0.036).
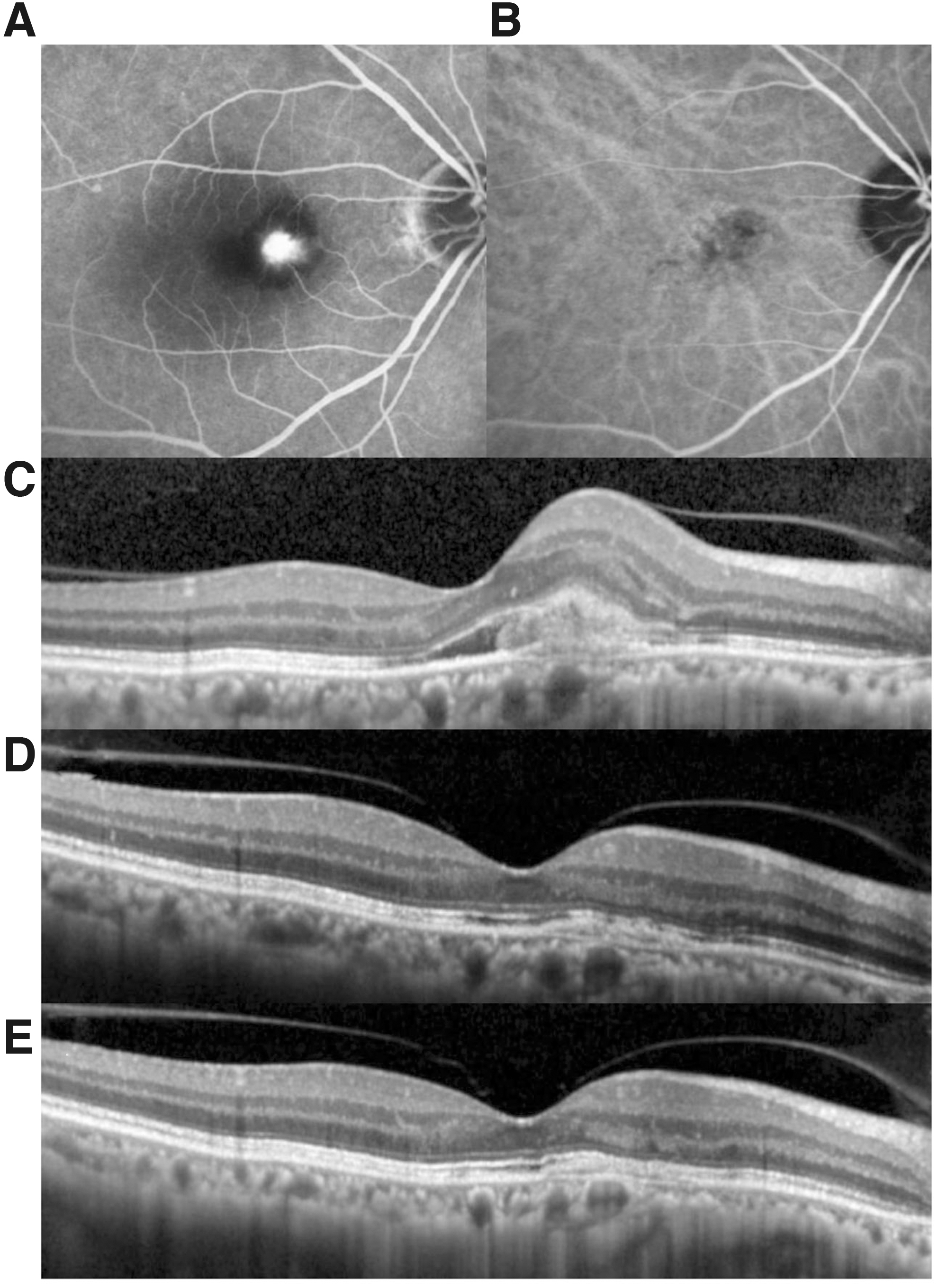
A representative case shows long-term no reactivation of the lesion in a patient diagnosed with neovascular AMD. After diagnosis
Comparison of Baseline Parameters and Morphologic Biomarkers Between the Reactivation Group and the Non-Reactivation Group
Data are presented as mean ± standard deviation or number (percentage) when applicable.
Chi-square test.
Fisher's exact test.
Snellen equivalent.
ERM, epiretinal membrane; VEGF, vascular endothelial growth factor.
Baseline Parameters and Morphologic Biomarkers Associated with Reactivation After Initial Treatment
Binary logistic regression.
CI, confidence interval.
Among the 100 patients with neovascular AMD, reactivation was noted in 75 patients (75.0%). Among the 92 patients with PCV, reactivation was noted in 81 patients (88.0%). Figure 4 shows the difference in the trend of lesion reactivation between neovascular AMD and PCV. In neovascular AMD, the timing of lesion reactivation was <6 months in 42 patients (42.0%), ≥6 months and <12 months in 18 patients (18.0%), and ≥12 months in 15 patients (15.0%). In PCV (n = 81), the timing of lesion reactivation was <6 months in 39 patients (42.4%), ≥6 months and <12 months in 17 patients (18.5%), and ≥12 months in 25 patients (27.2%).

Kaplan-Meier graph showing the difference in the trend of lesion reactivation between neovascular AMD (solid line) and PCV (dotted line), according to time after the third anti-VEGF injection.
Among the 36 patients in the non-reactivation group, RPE atrophy was noted at the final follow-up in 13 of 25 patients (52.0%) with neovascular AMD and 3 of 11 patients (27.3%) with PCV (P = 0.277) (Fig. 5).

A representative case shows the development of RPE atrophy in a patient diagnosed with neovascular AMD. After diagnosis
During the follow-up period, a mean of 3.0 anti-VEGF injections was administered to the non-reactivation group and a mean of 11.1 ± 5.6 anti-VEGF injections was administered in the reactivation group. Figure 6 shows the time-dependent changes in BCVA in the non-reactivation and reactivation groups. In the non-reactivation group, the BCVA was 0.81 ± 0.58 at diagnosis, 0.69 ± 0.61 at 1 year, 0.66 ± 0.62 at 2 years, 0.64 ± 0.63 at 3 years, and 0.72 ± 0.68 at 5 years. In the reactivation group, the values were 0.59 ± 0.51, 0.47 ± 0.44, 0.58 ± 0.53, 0.70 ± 0.60, and 0.86 ± 0.76, respectively. During the 5-year follow-up period, a mean improvement of 0.11 ± 0.47 in BCVA was noted in the non-reactivation group, whereas a mean deterioration of 0.26 ± 0.69 in BCVA was noted in the reactivation group. There was a significant difference in the change in BCVA between the 2 groups (P < 0.001).
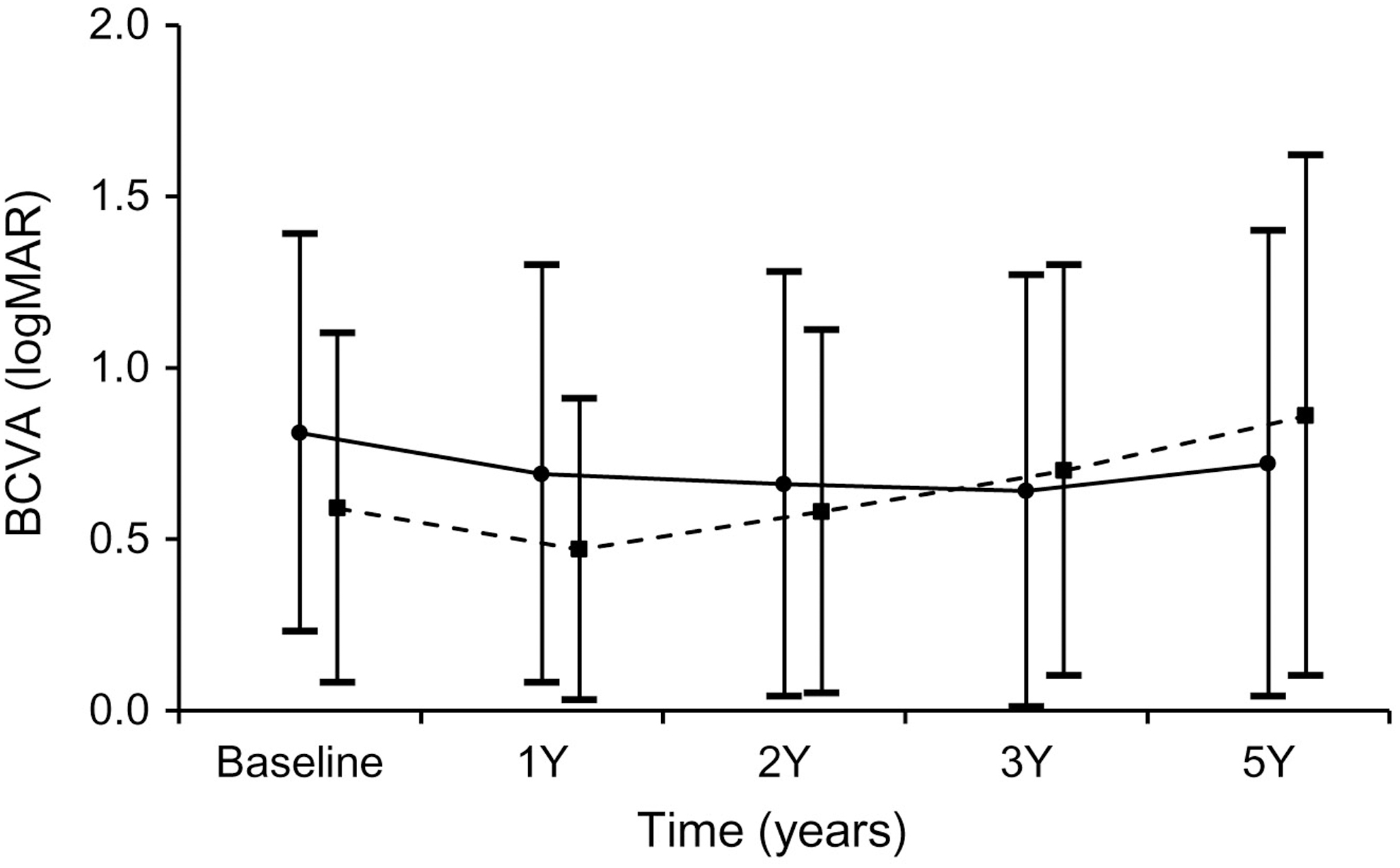
Time-dependent changes in BCVA in the non-reactivation (closed circle, solid line) and reactivation (closed square, dashed line) groups. logMAR, logarithm of the minimal angle of resolution; BCVA, best-corrected visual acuity.
When the first reactivation was noted, the type of fluid on OCT was as follows: SRF alone in 57 patients (36.5%), IRF alone in 38 patients (24.4%), subretinal hyperreflective material alone in 8 patients (5.2%), and mixed fluid types in 53 patients (33.9%). RPE rip was noted in 4 patients. A mean of 1.5 ± 0.8 injections was administered to treat the reactivation. In 96 patients (61.5%), only a single anti-VEGF injection was administered. In the remaining 60 patients (38.5%), 2 to 4 consecutive injections were administered to treat the reactivation. The fluid or hemorrhage was completely resolved after treatment for the first reactivation in 141 patients (90.4%). Among them, the second reactivation was noted during the follow-up period in 129 (91.5%) patients. The VA was 0.51 ± 0.45 before the reactivation, 0.69 ± 0.49 when the reactivation was noted, and 0.59 ± 0.47 after the treatment. Fifty-two patients (33.3%) failed to recover the pre-reactivation VA after treatment. After the first reactivation, 150 patients (96.2%) were still treated using an as-needed regimen and the treatment regimen was switched to TAE in the remaining 6 patients (3.9%).
Discussion
In this study, lesion reactivation was noted in 81.3% of patients who were initially treated with 3 loading injections of anti-VEGF. The majority of the reactivation was noted within 12 months of treatment. The incidence of lesion reactivation tended to decrease with time. In addition, there was a significant difference in the incidence of neovascular AMD and PCV.
It is well known that lesion reactivation does not occur in some patients treated with 3 loading injections of anti-VEGF. The incidence during the first year after diagnosis was reported to be between 62.5% and 72.5%.9,11,14 In the study by Kuroda et al., lesion reactivation was noted in 65.7% of patients during the first 12 months and 74.8% during the 24 months after diagnosis, suggesting that the incidence of reactivation may decrease with time. In this study, we attempted to identify whether this trend actually occurs during the long-term follow-up period by analyzing the incidence of lesion reactivation among patients who did not experience reactivation. As a result, a time-dependent significant decreasing tendency of lesion reactivation was noted. During the first year, the incidence of lesion reactivation was 59.9%. However, the incidence decreased to 5.3% in the fifth year. This result suggests that if there is no reactivation during the long period after the initial treatment, it is likely to maintain a stable status in the future.
In a previous study, the incidence of lesion reactivation during the first year after diagnosis was slightly higher in PCV than in neovascular AMD. 14 However, this difference was not statistically significant. In our patients, the long-term incidence of reactivation was significantly higher in PCV than in neovascular AMD. The incidence during the first year was comparable between neovascular AMD (60.0%) and PCV (60.9%). However, the incidence after 12 months was almost twofold higher in PCV (27.2%) than in neovascular AMD (15.0%). This result suggests that when using an as-needed regimen, PCV patients should be closely followed up even when lesion reactivation is not noted for a long period after initial treatment. The exact reason for this difference in late reactivation between the 2 groups is unclear. We postulate that the difference in the incidence of RPE atrophy between the 2 groups may partially influence this difference.
RPE atrophy is a frequently observed phenomenon during anti-VEGF therapy for neovascular AMD. The incidence of macular atrophy was reported to be between 43% and 44.4% during the 5-year treatment of neovascular AMD.16,17 A recent study demonstrated that RPE atrophy is also noted in approximately one-tenth of PCV. 18 RPE atrophy is generally considered a poor prognostic morphologic biomarker because it is associated with decreased visual acuity. 16 However, several investigators have demonstrated that it is also associated with decreased reactivation rate.19,20 Decreased VEGF secretion due to reduction of RPE cells and photoreceptors was suggested as a potential explanation for this phenomenon.19,20
In this study, the incidence of RPE atrophy at the final follow-up was almost 2 times higher in neovascular AMD (52.0%) than in PCV (27.3%). Although the difference was not statistically significant between the 2 groups, it is possible that this nonsignificant result was mainly due to the small sample size. The lack of RPE atrophy suggests that RPE and photoreceptors are generally preserved. Recently, Chen et al. demonstrated that type 1 macular neovascularization can sustain RPE and decrease the extent of overlying photoreceptor atrophy. 21 PCV is generally considered type 1 macular neovascularization. 22 Thus, it is possible that the RPE and photoreceptors in our patients with PCV, but without definite RPE atrophy, may be relatively preserved. Since RPE and photoreceptors can be a source of VEGF secretion, preservation of these tissues may lead to late reactivation of the lesion.
In this study, patients without reactivation showed better visual outcomes than those with reactivation. In addition, one-third of the patients with reactivation failed to recover VA before the first reactivation even after successful treatment of the reactivation. Moreover, the second reactivation developed in most patients who experienced the first reactivation. This result suggests that, to minimize visual deterioration, complete suppression or minimization of the reactivation episode would be of value. The TAE regimen is one of the widely used treatment regimens, characterized by the performance of continuous injections, regardless of lesion reactivation, with adjustment of injection intervals. 23 Since the TAE regimen can minimize damage accumulations due to multiple reactivations, the treatment outcomes of the TAE regimen are generally superior to the as-needed regimen. 24
However, 1 limitation of the TAE regimen is that it generally requires more frequent injections than an as-needed regimen.3,24 For cost-effective treatment, applying an as-needed regimen in patients with a low risk of reactivation and a TAE regimen in patients with a high risk of reactivation would be a plausible approach. However, we were unable to reveal any baseline factor predictive of long-term reactivation in this study, suggesting that predicting the reactivation is not an easy task. Thus, to achieve a better visual outcome, administering a TAE regimen immediately after diagnosis can be a plausible treatment strategy. Midena et al. recently reported that 77% of patients reduced or ceased daily activities, such as reading and driving, despite having undergone anti-VEGF therapy. 25 This suggests the importance of achieving the best visual outcome in neovascular AMD and highlights the usefulness of the TAE regimen. Recent advancements in artificial intelligence (AI) have aided in predicting future outcomes of AMD, such as the risk of conversion to neovascular AMD. 26 We postulate that further AI studies may help predict the reactivation after initial treatment.
Recent OCT angiography studies have shown that anti-VEGF therapy can alter the structure of macular neovascularization. In the study by Miere et al., vascular flow remodeling was noted after anti-VEGF treatment and this change was associated with treatment response. 27 In addition, anti-VEGF therapy also changes the PED. Javaheri et al. reported that flattening of the PED was noted after ranibizumab therapy. Although the flattening of PED is not significantly associated with visual outcomes, it has been associated with a lesser injection frequency during a 24-month follow-up period. 28 In this study, OCT angiography was not routinely performed. In addition, the change in PED was not assessed. Thus, we could not identify whether the vascular remodeling or flattening of PED after initial anti-VEGF therapy is associated with the lesion reactivation. Further studies are needed to address this issue.
Outer retinal tubulation and cystoid macular degeneration are well-known OCT findings that can be misdiagnosed as active exudation from the neovascular lesion. Outer retinal tubulation is characterized by circular or oval hyperreflective bands around a hyporeflective core located in the outer nuclear layer, which is considered to be derived from a degenerative process of outer retinal reorganization. 29 Dolz-Marco et al. showed its development process and suggested that patients with outer retinal tubulation may not benefit from therapeutic interventions because the outer retina undergoes an irreversible degenerative process. 29 Cystoid macular degeneration is a finding mimicking IRF, which may correspond to Muller cell degeneration. 30 Querques et al. showed morphologic characteristics of cystoid macular degeneration distinguished from real exudation, and suggested that cystoid macular degeneration should not require prompt treatment. 30 We carefully reviewed OCT images to differentiate these 2 findings from real exudation by lesion reactivation in this study. Nevertheless, the possibility of confusing these findings with real exudation should not be ignored.
Lim et al. recently demonstrated the difference in the efficacy of ranibizumab with or without photodynamic therapy for PCV. 31 In their report, the combination therapy group received fewer ranibizumab injections than the ranibizumab monotherapy group throughout a 24-month follow-up period. 31 This result suggests that combination therapy may decrease the risk of lesion reactivation. In this study, all patients were treated with anti-VEGF monotherapy. Thus, we could not determine whether the incidence of lesion reactivation differs between patients treated with anti-VEGF monotherapy and those treated with combination of anti-VEGF and photodynamic therapy. Further controlled studies are needed to identify any difference in lesion reactivation between 2 treatment modalities.
The strength of this study was that the 5-year long-term incidence and timing of reactivation were evaluated. In addition, differences in reactivation between neovascular AMD and PCV have been reported. However, this study has obvious limitations. First, it was retrospective, and patients lost to follow-up before 5 years were excluded from the study. Therefore, selection bias may have influenced the study results. Second, the follow-up intervals were not strictly controlled. Thus, the timing of reactivation may have been overestimated in some patients. Third, OCT angiography was first introduced at our institution in 2016; it was not a routinely performed examination even after its introduction. Previous studies have shown the usefulness of OCT angiography findings in prediction of lesion reactivation.32,33 However, we were unable to perform OCT angiography-based prediction of lesion reactivation due to the aforementioned reasons. Finally, all included patients were Korean.
In summary, we evaluated the 5-year duration of long-term lesion reactivation after the initial treatment. Lesion reactivation was noted in 81.3% of the patients who were initially treated with 3 loading injections of anti-VEGF. The incidence of lesion reactivation was highest during the first 12 months and decreased thereafter. The incidence was higher in patients with PCV than in those with neovascular AMD, especially after 12 months. Further studies are required to verify whether long-term no reactivation may ultimately lead to a cure for neovascular AMD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Kim's Eye Hospital Research Center.