
Abstract
The Pandora's box myth addresses the evilness in the world that undisputedly nowadays is identified in severe acute respiratory syndrome (SARS)–Coronavirus 2 (CoV-2), formerly known as Covid-19, which belongs to coronaviridae family, identified in Wuhan, Hubei district of the Republic of China in December 2019. Since then, SARS-CoV-2 has affected ∼180 million people and made almost 4 million victims, with a mortality rate of 6.1%, which is 6 times higher than influenza virus. However, coronaviruses are well known in the ophthalmology field because they were used in the so-called experimental coronavirus retinopathy model. That model certainly brings intriguing concepts for understanding coronavirus pathophysiology, which may have important implications on treatment strategies. Certainly, the recent availability of vaccines gives hope on the control of virus spreading; however, vaccines might create immune reactions involving the eye structure. In this study, we reviewed the literature and elaborated the available data to speculate on possible new interpretation of both pathophysiology and treatment of SARS-CoV-2.
Introduction
The Pandora's myth is a theodicy addressing the question of why there is evil in the world. Pandora is a character of the ancient Greek's mythology who was molded by Hephaestus and endowed with gifts by all the other Olympian gods as per Zeus instructions. Pandora opened a jar, the infamous Pandora's box, releasing all the evils of humanity.
Nowadays the evil is undisputedly represented by severe acute respiratory syndrome (SARS)–Coronavirus 2 (CoV-2), formerly known as Covid-19, 1 a coronavirus variant that was identified in Wuhan, Hubei district of the Republic of China in December 2019 (Fig. 1).
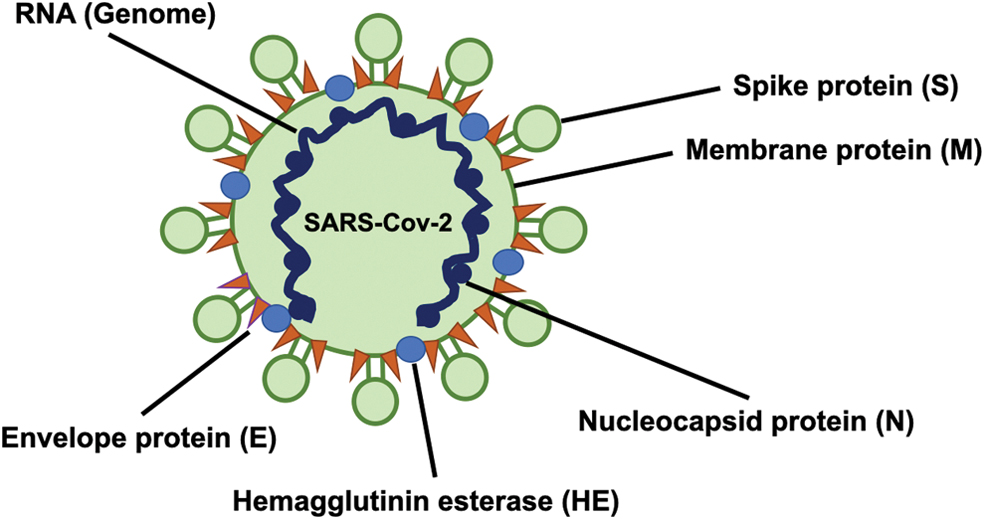
SARS-CoV-2 structure. Spike protein (S) is the main component that has been identified as interacting with angiotensin-converting-enzyme-2 receptor. SARS-CoV-2, severe acute respiratory syndrome-coronavirus 2. Color images are available online.
SARS-CoV-2 is just the last of the 7 types of coronaviruses (CoV), which are recognized as potential threat for humans: 229E (alphacoronavirus), NL63 (alphacoronavirus), OC43 (betacoronavirus), HKU1 (betacoronavirus), MERS-CoV (betacoronavirus), SARS-CoV (betacoronavirus), and SARS-CoV-2 itself.
Its outbreak affected ∼80,000 people leading to 3,000 deaths owing to severe pulmonary complications. 1 In the following months SARS-CoV-2 rapidly spread all over the world and was recognized as a pandemic by the World Health Organization (WHO) on March 11, 2020. 2
After more than 1 year, on an official report released on June 29, 2021, the disease was detected in ∼180 million and the number of global deaths reached almost 4 million, with a higher incidence in elderly and compromised patients. SARS-CoV-2 carries a mortality rate of 6.1%, compared with influenza that is ∼1%. 3
Countries are still encountering massive and dramatic problems in terms of prevention and sustainability of pharmacological treatments of complicated cases.
However, there was in the past year a rally by researchers to find a way to prevent or, at least, limit the severe complications of SAR-CoV-2: different vaccines were produced and distributed, and a worldwide vaccination campaign represents a tangible hope for the entire world.
CoV represent an old acquaintance for ophthalmology researchers. In this review, we will apply the scientific concepts learned to create a model for understanding pathophysiology, treatment, and interaction with the ocular structures of SARS-CoV-2. Last but not the least, we will go through the recent vaccines and on how they might create immune reactions involving the eye structure.
In this review we elucidate on how the eye might represent a novel Pandora's box: we will go through the ocular manifestations, the animal models, and see that vaccines might be a trigger of the eye immune response.
SARS-CoV-2 and the Eye: Controversies and Updates
CoV are an eclectic family of viruses, which are prone to affect not only the respiratory tract, but also other organs, such as gastrointestinal tract, 4 as well as the ocular structures. 5 It is important to point out that the involvement of other organs is not an irrelevant occurrence and it might have implications for the transmission of CoV: in 2003, when SARS-CoV outbreak occurred in Hong Kong, the local health authorities speculated that the infection was likely transmitted through the sewage system. 6
The eye represents another possible entry site for CoV and might contribute to its spreading thanks to tears production.
In 2004 HCoV-NL63 was identified in a 7-month-old infant and afterward isolated in 7 other patients. At the onset of the disease, the newborn presented bronchiolitis and conjunctivitis. 7 HCoV-NL63 was accordingly classified as a new human coronavirus.
One year later, a retrospective study in France reported data on children affected by respiratory illnesses who were tested by nasal swabs from 2000 to 2003 for HCoV-NL63. The study reported that 3/18 (17%) HCoV-NL63 patients had developed conjunctivitis. 8 Unfortunately, the pathogenic mechanisms of HCoV-NL63 in the infection of ocular tissues still remain unknown because no further studies/investigations were carried out.
Based on genomic and biostructural investigations, SARS-CoV-2 presents SARS-CoV receptor-binding motif-like structures. Such biologic properties allow SARS-CoV-2 to interact with angiotensin-converting enzyme-2 (ACE2) and, consequently, infect the host. 9 This is probably because of the polyvalent role played by the renin–angiotensin system (RAS), which does not have only an endocrine role in blood pressure regulation, but also express autocrine properties within certain organs.
The human eye expresses RAS that has been the target of researchers for the development of anti-glaucomatous drugs. In addition, ACE2 has been identified in the aqueous humor. 10 ACE2-receptor (ACE-R) expression in the anterior tissues, such as the cornea and the conjunctiva, represented a hot topic during the 2020 pandemic and has put the eye at the center of a lively debate. In one of its first reports, WHO listed conjunctival congestion as a manifestation in 0.8% of patients affected by SARS-CoV-2, leading to speculation on a possible SARS-CoV-2 transmission through conjunctival tissue. 11
In August 2020, Colavita et al. 12 reported a case of SARS-CoV-2 associated with conjunctivitis. The authors performed ocular swab and were able to detect viral RNA. Subsequent ocular samples were collected on a daily basis and remained positive up to day 21, with a progressive improvement of the conjunctival inflammation that resolved within the following 3 weeks. However, SARS-CoV-2 RNA was still being detected in the ocular swab at day 27, which indicates a sustained replication in conjunctival tissue.
However, the conclusions proposed by Colavita et al. that ocular fluids may be a potential source of infection was questioned by other authors who challenged the real meaningfulness of conjunctiva as potential source of infection. In 2020, Lange et al. 13 collected a total of 38 conjunctival samples from 38 patients with various conjunctival pathologies: 12/38 healthy tissues, 12/38 melanomas, 7/38 squamous cell carcinomas, and 7/38 papilloma samples. Those tissues were analyzed by high-throughput RNA sequencing for assessing mRNA expression of the SARS-CoV-2 ACE2-R. Other ACE-2 coreceptors, such as alanyl membrane amicopeptidase (ANPEP), glutamyl aminopeptidase (ENPEP), transmembrane serine protease 2 (TMPRSS2), and dipeptidyl-peptidase 4 (DPP4), were studied. In addition, the authors checked the expression of ACE2 in 8 healthy conjunctival tissues by immunohistochemistry. After that analysis, SARS-CoV-2 ACE2-R was not significantly expressed in conjunctival samples on the mRNA and protein levels. Such result matched the transcription of the other studied molecules mentioned previously. The authors concluded that no significant expression of either ACE2-R or of its ancillary molecules could be detected in the analyzed conjunctival tissues. The authors concluded that conjunctival infection with SARS-CoV-2 appears to be very unlikely through such cells' mediators. On the contrary, the controversies on this specific issue do not allow us to be conclusive on the possible risk of transmission of the virus through ocular route. Therefore, a careful behavior is recommended until further clarification will give undisputed evidence.
SARS-CoV-2 and Systemic Complications: The Eye as an Inspirational Model
During the dramatic surge of severe life-threatening cases of SARS-CoV-2, many researchers started looking for a potential rescue treatment. Although the management of SARS-CoV-2 infection is mostly supportive, series of therapeutic approaches were proposed to minimize both the severity of the disease and its high mortality rate. The real challenge is represented by cases turning to the more aggressive form of SARS-CoV-2 interstitial pneumonia, with fatal acute respiratory distress syndrome (ARDS). 14
SARS-CoV-2 is prone to aggressively involve not only lungs, 15 but also skin, 16 central nervous system (CNS), 17 gastrointestinal tract, 18 as well as the eye. 1
A combination of hydroxychloroquine and azithromycin was first hypothesized as a possible treatment protocol, 19 but later it was found to be of no significant scientific value. 20
The off-label use of monoclonal antibodies targeting biologic players that implement the hypercytokinemia, which leads to multiorgan failure, 21 has been the core treatment for the severe complication of ARDS. Tocilizumab [Actemra; Roche Pharma (Schweiz) Ltd., B2084B21], an anti-interleukin-6 receptor (anti-IL-6-R) monoclonal antibody, was the first biologic agent used as a potential rescue therapy for severe SARS-CoV-2 cases presenting the so called “cytokine storm syndrome,” name first coined in 1991 for a similar condition seen after muromonab-CD3 infusion. 22
Although more than a year has passed since the outbreak of SARS-CoV-2 and despite a number of vaccines been approved under emergency protocol by the drug agencies in all the continents, many countries worldwide are still struggling with novel virus mutations 3 and the challenge they impose on the health care systems. One of the main issues is the high percentage of cases turning to the life-threatening condition known as hemophagocytic lymphohistiocytosis (sHLH), a hyper-inflammatory syndrome affecting primarily not only the lungs but also other organs, 21 in particular the CNS.
In 2 editorials published at the beginning of the pandemic in 2020, we speculated on a possible theory based on ocular immune system as a model upon which to rely a possible therapeutic strategy.23,24
Looking into the medical literature, we found that in 1990, Robbins et al. proposed an animal model for experimental retinitis by using John Howard Mueller (JHM) strain of mouse hepatitis virus (MHV): the authors reported that the inoculation of MHV induced an acute and long-lasting retinal inflammation. 25 Few years later, the definition of experimental coronavirus retinopathy (ECOR) was coined for such a model. 25
Evidence came from the same group that MHV is naturally prone to a specific retinotropism independently of the route of administration in the experimental animal (ie, the cornea, the anterior chamber, intravitreally, intracerebrally, or intranasally). 25
In particular, the virus provokes an insult to every single retinal structure, including retinal pigment epithelium (RPE) and photoreceptors, leading to a progressive impairment.
MHV viral antigens can be detected in the inner nuclear layer, photoreceptors, Muller cells, and RPE, but only in the ganglion cell layer they persist after 10 days from inoculation, thus indicating a trend for spontaneous virus clearance in the other retinal tissues. A further interesting aspect was the RPE fibrosis and the retinal atrophy that followed the retina infection, secondary to fibroblasts activation in the attempt to repair impaired retinal tissues.
SARS-CoV-2 seems to have the same neurotropism: several publications reported nervous system involvement where Guillan–Barrè syndrome seems to be the first manifestation of the disease. 26
Can ECOR represent a possible experimental model to help researchers approach severe SARS-CoV-2 systemic complications? In our previous publication and in this review we propose an insightful model for researchers.
Although the number of SARS-CoV-2-related articles is constantly growing in the medical literature, there is still lack of significant knowledge on the role played by the immune system in lungs involvement. Lungs histopathology shows moderate multinucleated giant cells, minimal lymphocytes, eosinophils, CD4-positive T cells, and neutrophils, 27 leading to edematous, widened, congested blood vessels of alveolar septum. A crucial role in the outcome of such a condition is the presence of hyaline thrombi in microvessels, as well as interstitial hemorrhages, intra-alveolar exudates, and interstitial fibrosis. This lungs polythrombosis observed in late stages of SARS-CoV-2 pneumonia is very similar to the vascular involvement in ECOR, where the massive inflammation at the ciliary body leads to veins wall damage characterized by loss of continuity and erythrocytes extravasation into the surrounding tissue. We hypothesized that both may be the result of interstitial inflammation leading to hyaline thrombi as consequence of perivasculitis. 27 However, all those are postmortem findings and there is still lack of knowledge on the different phases of the disease.
A second information we may gather from the ECOR model is the biphasic behavior of Coronavirus, with a first primary infection triggering the immune system, which then plays a crucial role in the second phase that looks like a tout court autoimmune disease.
As already mentioned, SARS-CoV-2 presents a high fatality rate despite prompt intervention, 28 particularly in elderly patients. 29 However, even young adults may have a dramatic clinical course with a progressive worsening of the disease caused by a massive immune response. That seems to be secondary to SARS-CoV-2-driven cytokine release syndrome (CRS) or sHLH. 21 sHLH represents a life-threatening hyper-inflammatory syndrome driven by a massive activation of macrophages (it is also known as macrophage activation syndrome [MAS]). 30
At the beginning of the pandemic, there was reluctance to use corticosteroids to prevent viral shedding, 31 although systemic steroids are the mainstay of treatment to prevent other severe viral complications such as Herpes disease 32 and Ebola virus disease 33 and for CNS involvement in the very same SARS-CoV-2 disease. 34 Recently, dexamethasone was successfully used and showed a clear reduction of mortality by one-third among critical SARS-CoV-2 patients, 35 thus confirming what similar viral models 23 previously showed.
As already mentioned, the surge of deaths owing to MAS in critical cases lead to the off-label use of tocilizumab, inspired by its use for CRS secondary to chimeric antigen receptor (CAR) T cell therapy. 36 Zhang et al. 37 used tocilizumab successfully as a rescue treatment for severe cases of SARS-CoV-2 interstitial pneumonia. After that first report, several case series hypothesized that IL-6 inhibition might represent a crucial immune checkpoint to achieve control of the disease.
What remains unexplained is why in humans SARS-CoV-2 does not present always the same level of virulence and why anti-IL-6 treatment does not always offer the same efficacy regardless of the severity of the disease. 38
Our group speculated that a specific immune genotype, combined with environmental factors and viral triggers 21 may lead to cytokine release 10 and escalation of the disease severity. The so-called “threshold model” (Fig. 2) might be applied to SARS-CoV-2 disease similarly to MAS, justifying such a dramatic, massive immune response in young adults. 39
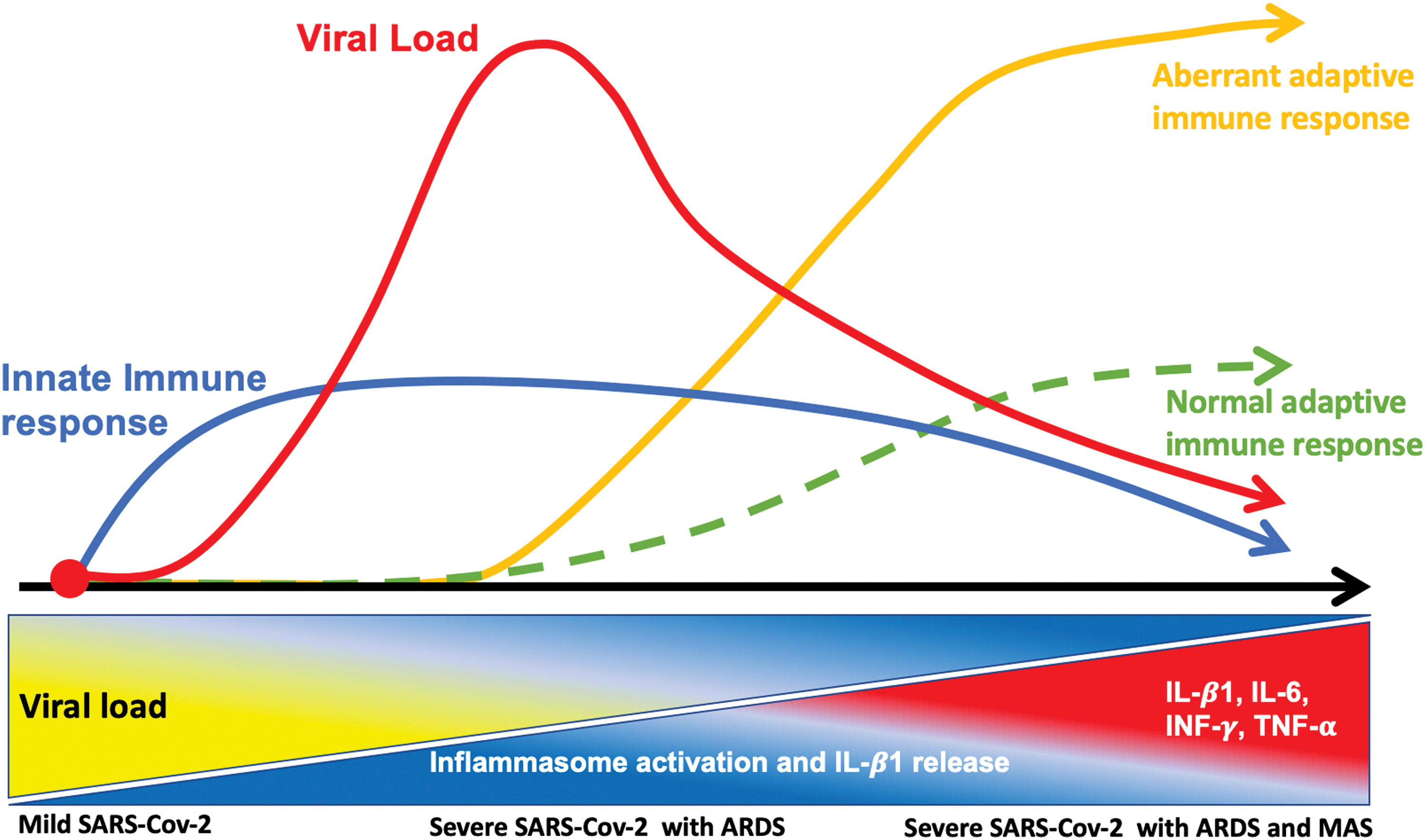
Model showing the triphasic hypothesis of the SARS-CoV-2 infection. When aberrant inflammasome response is activated there is an overdrive of the adaptive immunity (orange line) compared with the normal response (green dotted line). Color images are available online.
Once again, the eye immunity can represent a model to hypothesize the pathophysiology and therapy of SARS-CoV-2. Teoh et al. described a case of chronic infantile neurological cutaneous articular (CINCA) syndrome-associated uveitis 40 unresponsive to anti-Tumor Necrosis factor (TNF)-alpha treatment. The case highlighted the paradigm of tailored treatment, pointing out the improvement in understanding the polygenic nature of the inflammatory diseases and differentiating autoinflammation from autoimmunity. Indeed, CINCA syndrome-associated uveitis optimally responded to anti-IL-1β named Anakinra (Kineret™; Swedish Orphan Biovitrum, Stockholm, Sweden), proving once again that the treatment success is related to the nature of the disease. This result pairs the report by Dimopoulos et al. 41 who used Anakinra for MAS secondary to SARS-CoV-2 interstitial pneumonia. 42 Similarly, the authors speculated on tissue macrophages IL-1β overproduction triggering secondary MAS, which led to both hypercoagulation and, consequently, severe multiple organ impairment.
The positive outcome after anti-IL-1β therapy leads to hypothesize a specific role of autoinflammation in SARS-CoV-2 pathophysiology. The dramatic immune response and the occurrence of fatal events affecting young, otherwise healthy adults as well, might be generated by an immune genotype prone to such overactivated macrophages response. In a previous editorial we hypothesized that MAS may be the result of a series of events: impaired viral control, aberrant inflammasome activity, variable immune defects, and dysregulated metabolism. 30 The multiple combination of those factors might lead to MAS and, consequently, threaten the life of patients. We speculated on a possible interplay between inflammasome and SARS-CoV-2, which appears similar to its activity in ocular Behcet disease (BD), where the interplay between TLR2/4 and their ligands peptidoglycan (PGN)/lipopolysaccharide (LPS) leads to BD pathogenesis. 43
Our theory was recently confirmed by Ratajczak et al. 44 who demonstrated that in human very small embryonic-like stem cells and hematopoietic stem cells, the interaction of the ACE-R with the SARS-CoV-2 spike protein activates the nucleotide-binding domain (NOD)-like receptor protein 3 (NLRP3) inflammasome, which if hyperactivated may lead to cell death by pyroptosis. More specifically, NLRP3 plays a primary role in the control of viral activity, by recognizing different pathogen-associated molecular patterns, as well as danger-associated molecular patterns (DAMPs), which are the products of the viral replication. When not fully activated, NLRP3 has a sufficient low level without an overdrive of inflammasome activation. When viral insult leads to inflammasome activation by both viral components, 45 it provokes NLRP3 inflammasome activation and, consequently, IL-1β production, 46 which stimulates neutrophils recruitment. 47 Moreover, IL-1β induces adaptive immune response 45 that might overdrive the immune response toward SARS-CoV-2.
The hypothesis of a possible pathogenic variant of NLRP3 inflammasome genes might justify the higher risk of MAS activation is some subjects, 48 through IL-1β overproduction leading to cytokine storm driven by the SARS-CoV-2 insult. This hypothesis finds empirical evidence by looking at the favorable outcomes in severe cases treated with anti-IL-1β receptor therapy. 49
This theory led to revisiting SARS-CoV-2-associated MAS phases. The disease was supposed to be biphasic, with a first phase consisting of the viral insult and the second one in which the overdrive of immune system led to an autoimmune disease. We proposed that these phases should include an intermediate one where the immune system seems to be driven by an autoinflammatory response before autoimmunity is triggered.
Although this might seem just a semantic speculation, the difference might have dramatic implication in both interpreting the pathophysiology of SARS-CoV-2 disease as well as a more appropriate therapeutic approach.
Although the use of anti-IL-6 receptor has had positive effects on CAR-T-induced CRS, further studies on animal models showed that Anakinra presented a better outcome, whereas tocilizumab had lack of protection toward delayed lethal neurotoxicity. 50 Therefore, MAS induced by SARS-CoV-2 might be primarily endorsed by an aberrant autoinflammatory response. 30 In addition, pyroptosis-induced autoinflammation was identified, leading to the release of DAMPs, including ATP, nucleic acids, and ASC oligomers. 51
Moreover, the key role played by NLRP3 inflammasome in Kawasaki disease (KD) pathophysiology might explain the increasing number of pediatric cases of KD like SARS-CoV-2-associated disease.52,53
As a consequence of that, the core role played by autoinflammation in SARS-CoV-2-associated MAS leads to revisiting the tailored supportive immunotherapy: serum cytokine profile in SARS-CoV-2 patients should be considered, providing a prompt and appropriate rescue treatment strategy. More importantly, the “threshold model” needs to be revised by putting IL-1β as the primary immune system driver, which changes the disease pathophysiology from biphasic to triphasic (Fig. 2).
The importance of inflammasome activation in SARS-CoV-2 disease and the role played in the immune reaction indicates the need for further investigations that would lead to an optimization of the treatment strategy, consequently preventing life-threatening complications.
SARS-CoV-2 and Vaccines
Since SARS-CoV-2 pandemic outbreak occurred, vaccines became the hottest topic among the scientific community. The current rally in vaccinating patients represents the response of the entire world to the dramatic situation created by SARS-CoV-2 pandemic: herd immunity represents the main goal to obtain protection against the virus. As per WHO's draft landscape of SARS-CoV-2 candidate vaccines, we know that 42 candidate vaccines are under clinical evaluation, whereas 151 are currently undergoing preclinical trials. To date, we can count on 6 vaccines with 3 different technologies.
Viral vectors, mRNA, and inactivated virus vaccines are the 3 leading categories of vaccines currently available and approved by the medical commissions under the regulation of emergency protocol. Although the registrations trials did not report organ-specific issues, side effects are starting to be reported, opening a new chapter for ophthalmology. 54 The medical literature shows many cases of vaccine-associated ocular inflammatory diseases 55 and the possible occurrence of relapse/de novo ocular inflammations would not represent a novel complication.
Recently Pichi et al. published a series of 9 eyes presenting with ocular inflammation after the first inoculation of SARS-CoV-2 inactivated vaccine.
After the first dose, 2/9 eyes (22.2%) presented paracentral acute middle maculopathy (PAMM) and acute macular neuroretinopathy (AMN), respectively, such as it has been reported post-H1N1 vaccination. This seems to be aligned with the nature of both the vaccines 55 as observed for influenza 56 : inactivated/killed virus vaccines present a more unpredictable triggering of the native immune system through pattern-recognition receptors, which might induce more easily an overdrive of the immune response in several organs, including the eye.
Furthermore, Virgo and Mohamed 54 reported 2 patients with new paracentral scotoma secondary to AMN and PAMM 16 days after confirmed COVID-19 infections, which mirrors the data reported by Pichi et al. 55 The clinical occurrence of both PAMM and AMN might be induced by a possible neuroretinal inflammation, leading to the precapillary arterioles microvascular occlusion observed in ECOR model. 23 However, although less likely, a possible intravascular immune complex deposit might be a second reasonable hypothesis. Moreover, those findings recall the thrombotic microangiopathy associated with SARS-CoV-2 infection that has been associated with many severe cases.
Scleritis and episcleritis was reported in 4/9 (44.4%) of Pichi et al. cases after the first dose of the vaccine (Fig. 3). Despite no direct cause/effect proof might be identified, there are few reports of episcleritis and scleritis after administration of live, attenuated virus vaccinations, which might strengthen the hypothesis that such a vaccine might be more prone to incite the local immune system.56,57 However, vaccine-associated scleritis presented a mild severity and responded well to topical corticosteroids.
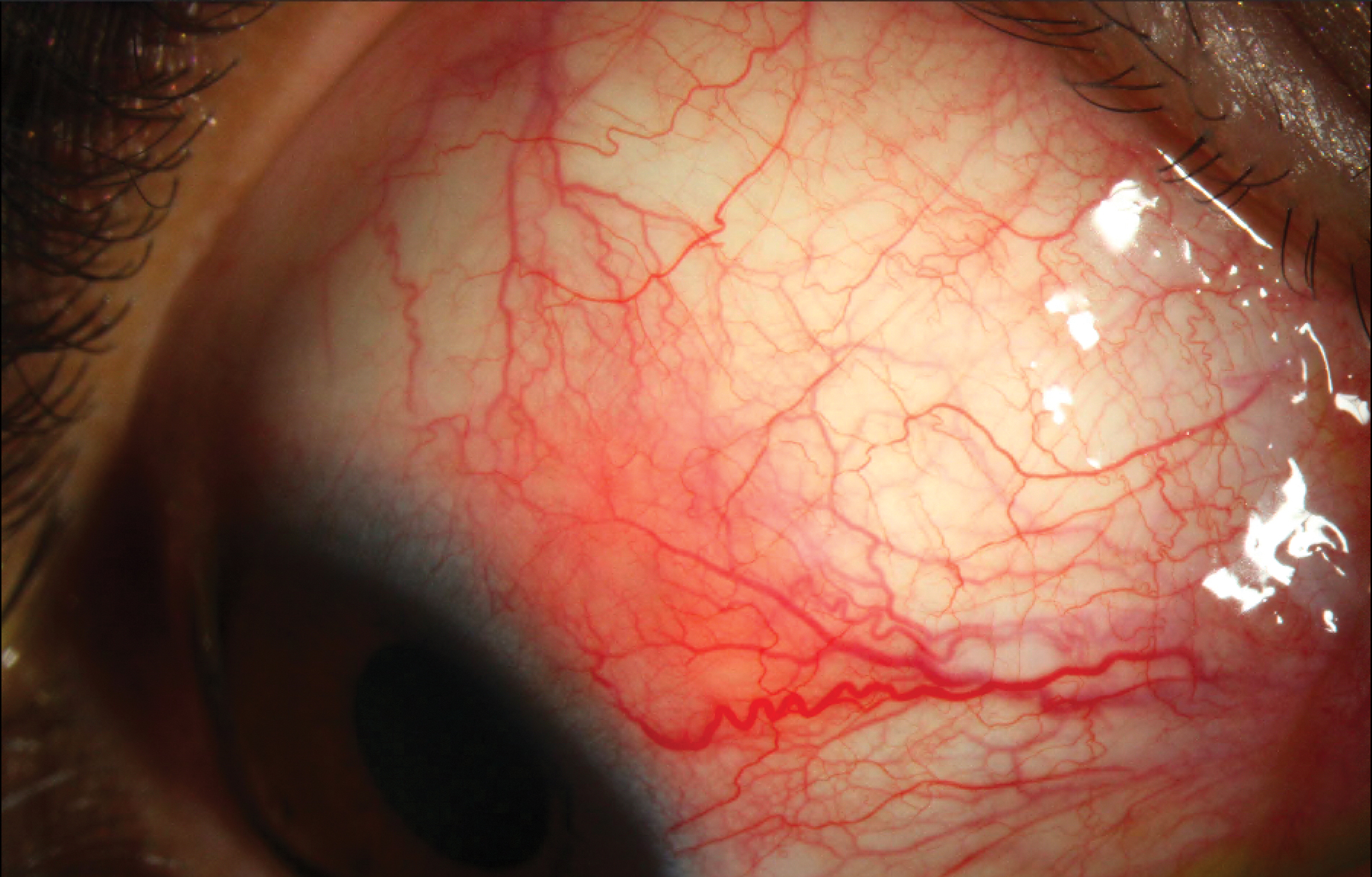
Unilateral nodular scleritis occurred 5 days after first dose of inactivated virus vaccine in a patient affected by systemic sarcoidosis. The patient was treated by topical corticosteroids and the scleritis solved within 2 weeks without recurring up to date. Color images are available online.
Indeed, as previously stated, vaccines might present a variety of posterior segment complications, including Vogt–Koyanagi–Harada, 58 AMN, 59 and multiple evanescent white dot syndrome. 60 In addition, post-mRNA vaccination has been associated with acute-onset central serous chorioretinopathy, 61 which might be owing to the interaction of vaccine antigens with the RPE inducing its impairment. This appears aligned to our speculations on the retinotropism of the coronaviridae and the ECOR model: vaccines might mimic the biologic behavior of the virus and incite the local immune system accordingly. Therefore, although the exact pathogenesis of vaccine-related ocular inflammation remains still unclear, molecular mimicry and antigen-specific cell and antibody-mediated hypersensitivity reactions seems to be the most accredited hypothesis.62,63
In addition to potential retinal immune system incitement, extracellular naked RNA has been associated with venous thrombosis, including retinal veins. Such an adverse event has been addressed by the Royal College of Ophthalmology of United Kingdom in a note published online on May 13, 202164 alerting the possible event of central retinal vein occlusion and issuing new guidelines to implement the safety measures.
These reports, although anecdotal, suggest to carefully review the medical history of patients and point out possible previous immune comorbidities: this might put a warning for specific patients and make them aware of the need for a prompt consultation with uveitis specialist to manage unpredicted, but possible side effects. In addition, as the urge for a broad vaccine campaign against SARS-CoV-2 continues, we might expect a possible increasing number of uveal tract inflammation. We stress the importance of a precise report of those events, and we wish for a possible database collection, to involve the entire scientific community in this important discussion.
Conclusions
CoV family is an old acquaintance of the eye immunity: ECOR model represents more than an inspirational model for the understanding of SARS-CoV-2 immunology and offers for sure interesting similarities that may inspire scientist on how to approach severe cases specifically.
Although it was supposed that SARS-CoV-2 might have a biphasic behavior, recent hypothesis lead to consider the disease characterized by 3 phases.
SARS-CoV-2 has CNS tropism and may induce several neurological manifestations, showing neuroinvasive properties, 65 including the eyes. The role of NLRP3 inflammasome has been identified as a possible trigger of inflammation of both the retina and the uveal tract, such as uveitis. 43 It was also observed that IL-1β, among other proinflammatory mediators, was produced in SARS-CoV-infected ACE2-R 66 and this might happen in organs such the eye because of its neurotropism, explaining the reason why uveitis might occur both in post-SARS-CoV-2 infection 67 and vaccinations as well. 55 This may give more value to the theory that SARS-CoV-2-induced NLRP3 overdrive might play a significant role in MAS occurrence and, consequently, immunotherapy should consider anti-IL-1β agents as valid rescue treatments.
The potential core role played by autoinflammation in SARS-CoV-2-associated MAS rewrites the story: the therapeutic stepladder should be reconsidered and the supportive immunotherapy for severe cases should be tailored differently. As consequence of that, a possible study of serum cytokine profile in SARS-CoV-2 patients may offer an oriented, prompt, and appropriate rescue treatment. In addition, the “threshold model” should be replaced by the triphasic model where IL-1β is identified as the primary player for immune system triggering (Fig. 2). The relevance of inflammasome activation and its role in SARS-CoV-2 immune reaction might be worthy of further investigations and may represent a perspective for the optimization of its treatment, to prevent life-threatening cases.
In addition, the possible role played by IL-1β might explain why different immune phenotypes of SARS-CoV-2 disease may be the expression of the same immune genotype, putting forward the reasonable hypothesis of a predominant role of inflammasome-driven MAS in the phase 2 of SARS-CoV-2 disease. The treatment approach should be revised consequently, as it happened for autoinflammatory diseases involving the eye such as CINCA syndrome. 40
The introduction of vaccines represents a breakthrough and the only way to prevent the disease and lead to herd immunity. However, vaccines might either trigger or reactivate inflammatory diseases of the eye that were described in the past for other vaccines, particularly the attenuated/deactivated virus ones.
In conclusion, the eye represents both a model and target for immune system, a Pandora's box that should never be opened.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.