
Abstract
Purpose:
To evaluate the effect of reducing blood pressure (BP) by atenolol and amlodipine on (1) intraocular pressure (IOP) and (2) ophthalmic artery blood flow (OAF) velocity in new hypertensives.
Methods:
A prospective, observational cohort study conducted at a tertiary care center in India after IRB approval. New hypertensives treated with atenolol 25 mg or amlodipine 5 mg were divided into 2 groups of 30 patients each. BP, IOP by Goldmann applanation tonometry and OAF velocity by transcranial doppler sonography was performed before medication and post medication on day 1, 7, and 30.
Results:
There was a significant decrease in IOP with both drugs; the effect was greater with atenolol. Atenolol: premedication IOP - 16.06 ± 2.13 mmHg and day 30–12.46 ± 1.94 (22.4%) [P < 0.001], amlodipine: premedication IOP-15.13 ± 2.55 mmHg and day 30- 13.06 ± 2.14 (13.68%) [P < 0.001]. A decrease of 0.5 mmHg in IOP with every 10 mmHg (95% CI: 0.121–0.826, P value = 0.01) decrease in systolic BP was noted after oral atenolol. The OAF peak systolic velocity and mean flow velocity were equally reduced with both drugs (P < 0.001). The end-diastolic velocity, reduced only with atenolol (P = 0.049) but returned to baseline with amlodipine at 1 month.
Conclusions:
BP reduction by atenolol and amlodipine led to decreases in IOP and OAF velocity, greater with atenolol. The IOP decrease was likely due to reduced blood flow. A slight decrease in the diastolic flow of the ophthalmic artery was noted with atenolol.
Introduction
The pathogenesis of glaucomatous optic neuropathy has been linked to a balance between mechanical and vascular causes and has been intensely investigated.1,2 Though intraocular pressure (IOP) is still the only treatable risk factor for glaucoma, accumulating evidence suggests that blood pressure (BP) may be a modifiable risk factor.3–22 However, the mechanisms are not fully understood. It may be valuable to study the change in retrobulbar flow occurring with change in BP and its effect on IOP. The pharmacological decrease in BP by beta-blockers and calcium channel blockers, commonly used medications for systemic hypertension, presents an opportunity to study these changes physiologically in treatment naïve patients. 23 Both have demonstrated ocular hypotensive effects in clinic-based studies.24–31
Additionally, the use of beta-blockers was associated with lower IOP in population-based studies.5,32,33 The use of calcium channel blockers was associated with a higher risk of POAG incidence. 34 Atenolol is a relatively selective β1 blocker with low lipid solubility and partial β2 blocking activity, and amlodipine is a third-generation dihydropyridine calcium antagonist with a long duration effect.35,36
Although lowering the IOP would likely reduce the risk of glaucoma, reducing BP with β-blockers and calcium channel blockers may reduce perfusion to the optic nerve, which may increase the risk of optic nerve head ischemia. Hypotension due to the use of antihypertensive medication, in particular, has been implicated in the pathogenesis of primary open-angle glaucoma (POAG) and normal-tension glaucoma (NTG).4,9–12,15–17,19,21 Optic nerve head damage is associated with lower BP and lower blood flow.7,9,11,15,17,37,38
Experimentally, it was seen that optic nerve head blood flow is more susceptible to an ocular perfusion pressure decrease induced by lowering the BP than that induced by increasing the IOP in primates. 39 Also, the optic nerve head is shown to autoregulate its blood flow rapidly to experimental changes in perfusion caused by IOP elevations. 40 While studies relating to changes in IOP and ocular blood flow with experimental increase in BP have been undertaken; it is not possible to evaluate the changes associated with decreasing BP in normal subjects due to ethical reasons.41,42 The potential influence of systemic beta-blockers and calcium channel blockers as antihypertensive drugs on ocular circulation and IOP has not been studied sufficiently.
The findings may have implications for the management of glaucoma patients with comorbidity and may provide insight into the pathophysiological processes underlying IOP. We undertook to evaluate the effect of oral atenolol (beta-blocker) and amlodipine (calcium channel blocker) in patients with newly diagnosed systemic hypertension on BP, IOP, and ocular blood flow velocity in the ophthalmic artery measured by transcranial doppler (TCD) sonography. Transcranial pulsed-wave doppler sonography of the first part of the ophthalmic artery has demonstrated good reproducibility for measuring ophthalmic artery flow velocity.43,44
Methods
The study was conducted at Ophthalmology, Internal medicine, Cardiology, and Neurology departments after approval from Scientific Committee and Institute Ethics Committee and followed the tenets of the Declaration of Helsinki. Newly diagnosed systemic hypertension patients attending Internal Medicine services were assessed by the physician/cardiologist and recruited after informed consent. As a preliminary study comparing pharmacological effects of antihypertensive medications on IOP and ophthalmic artery blood flow (OAF) velocity, a sample size of 30 patients per group was determined. 45
Inclusion criteria
Patients with newly diagnosed systemic hypertension (BP >140/90 mmHg) by current clinical criteria, based on the average of 2 or more seated BP readings during each of 2 or more outpatient visits, were included in the study.46,47 Those eligible for drug therapy were started on either atenolol or amlodipine as per the treating physician's discretion. Only patients requiring monotherapy with one of these 2 antihypertensive drugs were included; group I - oral atenolol 25 mg (a beta-blocker): 30 cases and group II - oral amlodipine 5 mg (a calcium channel blocker): 30 cases.
Exclusion criteria
(1) Patients receiving other antihypertensive drugs (2) patients with any ophthalmic disorders (including glaucoma) (3) patients with systemic diseases requiring vasoactive pharmacotherapy affecting IOP or IOP measurements (4) patients with a history of glaucoma therapy (medical, laser, or surgical) (5) patients with hypertensive emergencies.
Methodology
All patients were examined before and after taking medication on day 1, 7, and 30 on treatment. A thorough evaluation of all the patients was done by taking a detailed history, followed by a general, systemic and ocular examination. The BP was measured in the right arm, sitting posture by the auscultatory method using a standard mercury sphygmomanometer. After a 15-min rest, 2 recordings of BP were taken at an interval of 15–20 min.
Ocular examination
Patients underwent complete ophthalmic evaluation before and after initiating drug therapy. (1) Best-corrected visual acuity testing using Snellen's chart (2) slit-lamp examination (3) IOP using Goldmann applanation tonometer (GAT) (4) fundus evaluation with +90 D lens (5) pachymetry using ultrasonic pachymeter (6) TCD sonography of the ophthalmic artery using a 2-MHz ultrasound probe (Recorders and Medicare Systems, Haryana, India).
The ophthalmic artery flow velocity was measured as per the technique described earlier. 43 Briefly, after applying a coupling gel, the ultrasound transducer was gently placed over the upper eyelid, tilted 20–30o, and pointed toward the orbital apex. Flow signals at a depth of less than 40 mm and toward the probe, with a higher resistance pattern representing the ophthalmic artery, were measured. A trained operator in Neurology performed all measurements.
Normal spectral waveform
The normal spectral waveform shows a systolic upstroke and stepwise deceleration with the positive end-diastolic flow. The variables noted on typical TCD spectra are peak systolic velocity (PSV) in cm/s, the first peak on a TCD waveform that refers to the highest blood flow velocity achieved during systole; End-diastolic velocity (EDV) in cm/s: the lowest velocity occurring during diastole; Mean flow velocity (MFV) in cm/s, calculated as EDV plus one-third of the difference between PSV and EDV; Resistivity index (RI) calculated as (PSV-EDV)/PSV.
Mean arterial pressure (MAP) was calculated as DBP +1/3(SBP-DBP). Mean ocular perfusion pressure (MOPP) was defined as 2/3(MAP-IOP).
The right eye from each patient was used for statistical analysis. The collected data were analyzed using both descriptive and inferential statistics. The independent samples t-test was used to evaluate the statistical significance of change between the 2 groups of each of the measured variables. Repeated measures analysis of variance (RM-ANOVA) was used to test the significant difference among the changes over time within the group and 2-way RM-ANOVA for differences between the 2 groups. Simple linear regression analysis was performed to predict the change in IOP for 10 mmHg change in BP. A P value of <0.05 was considered significant and highly significant when P < 0.001. All the analysis was carried out with SPSS version 19 software.
Results
Our study included 30 patients each on atenolol 25 mg and amlodipine 5 mg. There were no differences in age (amlodipine: 50.60 ± 9.65 years, atenolol: 51.70 ± 7.81 years, P = 0.62), gender (men/women - amlodipine: 13/17, atenolol: 16/14, P = 0.44), and pachymetry (amlodipine: 543.66 ± 11.35 μm, atenolol: 542.60 ± 12.72 μm, P = 0.73) between the groups. Hence, differences in IOP and blood flow between groups could be attributed primarily to the drug. We compared the effect of the drug premedication and postmedication on day 1, 7, and 30 on BP, IOP, and OAF in both the groups.
Effect on BP and IOP
Both groups had similar systolic and diastolic BP measurements before treatment, with an equal magnitude of decline in BP after antihypertensive treatment (Table 1). The mean IOP in the atenolol group at baseline was 16.06 ± 2.13 mmHg, and the amlodipine group was 15.13 ± 2.55 mmHg, (P = 1.30). The maximum reduction in mean IOP was observed with atenolol after 24 h of initiating medication, being 12.00 ± 1.74 mmHg ∼4 mmHg decline, significantly greater than that due to amlodipine, at the same time point (P = 0.01). It was sustained till the end of 1 month, 12.46 ± 1.94 mmHg, a 3.6 mmHg decline from baseline (P < 0.001).
Comparison of Blood Pressure and Intraocular Pressure Between the 2 Groups Over 1 Month
BP, blood pressure; IOP, intraocular pressure; MOPP, mean ocular perfusion pressure; SD, standard deviation.
The mean IOP at baseline in the amlodipine group was 15.13 ± 2.55 mmHg, and the maximum reduction observed at the end of 1 month was 13.06 ± 2.14, a 2.07 mmHg decrease (P < 0.001). We observed that the mean IOP reduction was ∼2 mmHg more with atenolol than amlodipine after 24 h of initiating antihypertensive medication. The mean difference remained ∼1.5 mmHg greater in the atenolol group than amlodipine, even at the end of 1 month. On simple linear regression, decrease in systolic BP of 10 mmHg on average reduced IOP by 0.5 mmHg (R 2 of 21.3%, 95% CI: 0.121–0.826, P value = 0.01), in the atenolol group (Fig. 1). There was no significant relationship for amlodipine.
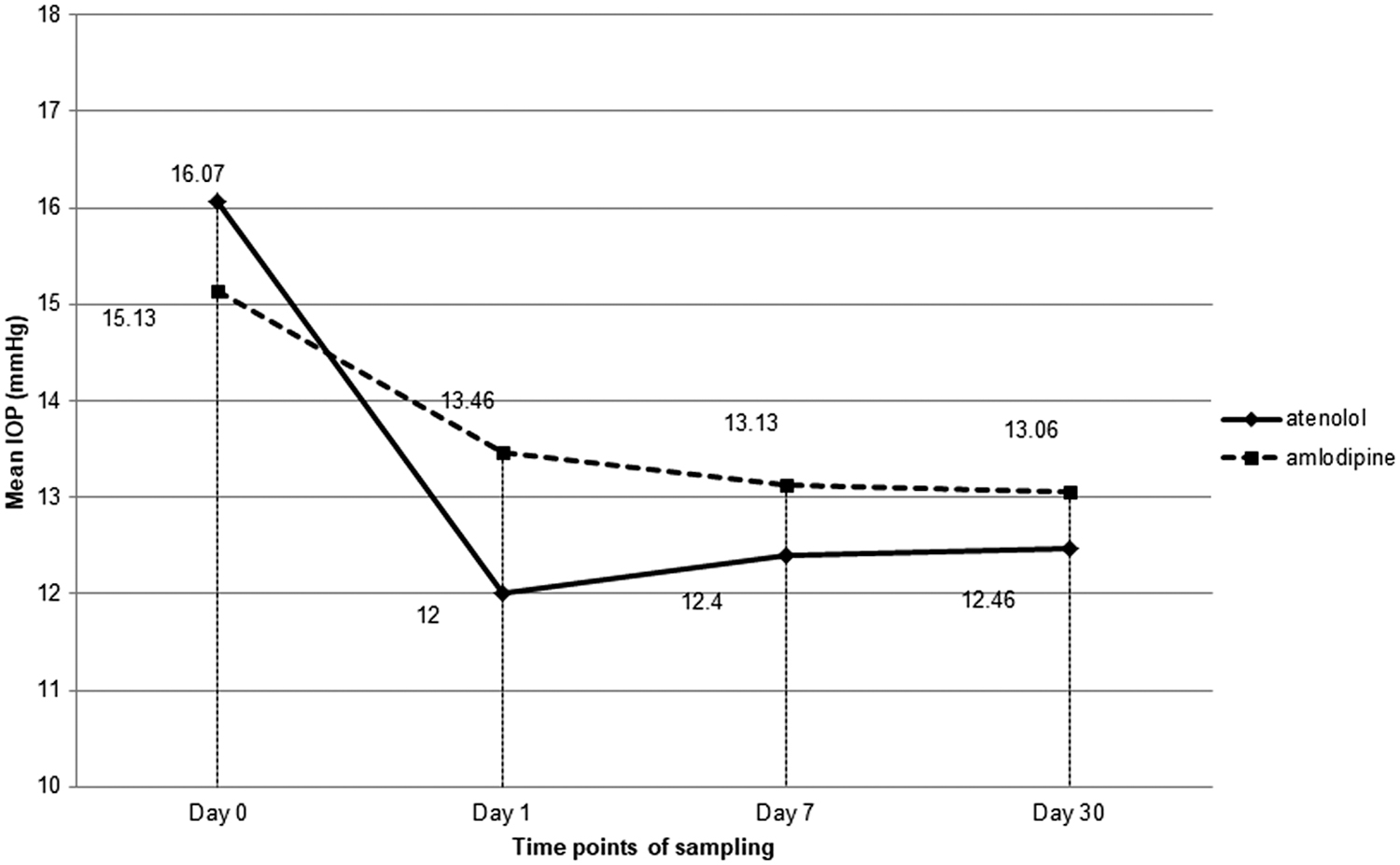
Comparison of IOP following oral atenolol and amlodipine in newly diagnosed hypertensives over 30 days. IOP, intraocular pressure.
Effect on OAF velocity parameters
The average PSV and MFV declined significantly over 1 month in both groups (Table 2). The average EDV showed an immediate decrease after 24 h of initiating antihypertensive treatment in both groups. This decline was sustained for atenolol till the end of the month (P = 0.049), 8.03 ± 1.71 cm/s, while it reverted to premedication levels for amlodipine by then. Both drugs reduced PSV and MFV, while amlodipine had a lesser effect on EDV at 1 month (Fig. 2).
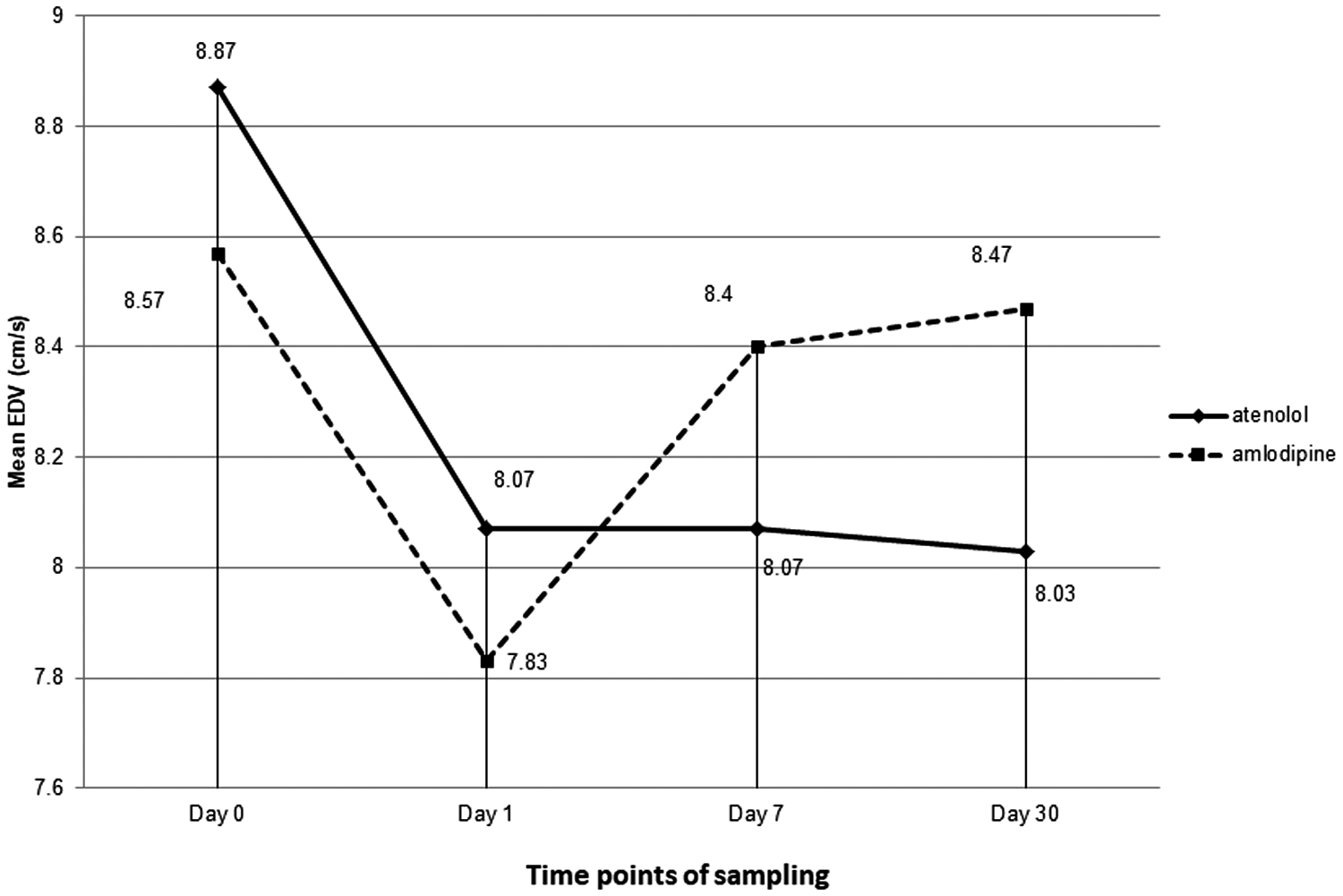
Comparison of EDV following oral atenolol and amlodipine in newly diagnosed hypertensives over 30 days. EDV, end diastolic velocity.
Comparison of Ophthalmic Artery Blood Flow Parameters Between the 2 Groups Over 1 Month
EDV, end diastolic velocity; MFV, mean flow velocity; PSV, peak systolic velocity; RI, resistivity index.
Discussion
BP has been positively associated with IOP, and high systolic BP has been consistently associated with increased IOP in several population-based studies.5,6,8,14,32,48–55 An increase in 0.21–0.33 mmHg of IOP for every 10 mmHg of systolic BP and 0.19–0.44 mmHg for every 10 mmHg of diastolic BP was reported, in cross-sectional studies.5,6,8,14,32
Our study showed systemic antihypertensive medications causing a reduction in both BP and IOP. This relationship is significant for beta-blockers and nonsignificant for calcium channel blockers. Investigators have speculated that the increased IOP observed with higher BP may result from increased aqueous production secondary to raised ciliary artery pressure, leading to increased passive transudative production of aqueous humor or increased sympathetic tone and elevated serum corticosteroid levels, leading to simultaneous increases in BP and IOP.56–58
In our study, antihypertensive therapy led to decreased BP and significantly lower OAF velocity, along with significant reductions in IOP. So, it follows that an overall reduction in blood flow velocity may be responsible for the modest, although significant, decrease in IOP. The decrease in PSV was greater with both the drugs than EDV. EDV returned to the premedication level at the end of 1 month, though IOP remained low with amlodipine. So, the effect of diastolic flow on aqueous production and, by extension, on IOP may be less than systolic flow. This is in concordance with the frequently reported association of systolic BP (reflecting systolic flow) with IOP in cross-sectional studies.5,6,8,14,32,47,48,50,51,54 Grunwald et al. have associated higher BP with higher flows, and Marjanović et al. have reported lower retrobulbar EDV among BP dippers.59,60
In our study, oral atenolol and amlodipine decreased BP and OAF velocities (PSV and EDV) equally. The mean IOP decrease was 1.5–2 mmHg greater with atenolol than amlodipine, significantly lower at Day 1 of administration. The use of beta-blockers has been associated with 0.45–0.92 mmHg lower IOP than other antihypertensive drugs in cross-sectional population-based studies.5,32–34 We found that oral atenolol caused a 0.5 mmHg decrease in IOP for every 10 mmHg drop in systolic BP. The more significant reduction in IOP in atenolol is probably due to decreased aqueous production at the level of the ciliary body. 61 Hence, in glaucoma patients with concomitant hypertension treated with beta-blockers, IOP may be lower due to aqueous suppression, and topical beta-blockers may be of limited value.
The lack of significant change with amlodipine may be due to the small sample size. Previous studies reported that calcium channel blockers have minimal effects on BP and IOP and no effect on ocular circulation.28–31,62,63 However, they were small studies on ocular circulation done in normotensive NTG patients administered the lowest daily dose of nifedipine (30 mg).62,63 In comparison, our study was conducted on early hypertensive patients using amlodipine (5 mg). This difference in study subjects and drugs may account for the differences in findings.
The decrease in BP after the medication was the same following both drugs, but EDV remained lower following atenolol than amlodipine. It returned to premedication levels in the amlodipine group at 1 month. Oral atenolol caused a slight but consistent decrease in diastolic flow throughout all observations. Our group consisted of early hypertensive patients on monotherapy, and we observed changes in the short term. It may be worthwhile to study the long-term changes in ocular blood flow in this group of patients, as current evidence suggests that lower EDV is associated with progressive glaucoma.7,37,38
Treated hypertensive patients with lower diastolic BP have demonstrably worse cup disc ratio and lower/progressive retinal nerve fiber layer (RNFL) loss.9,11,15,17 A higher detection rate of NTG among treated hypertensives screened for glaucoma is reported, with diastolic BP negatively correlating with RNFL. 17 NTG patients had lower PSV and EDV than POAG and normal controls. 64 Lower diastolic BP may be associated with lower EDV causing optic nerve ischemia, which is a further avenue of investigation.
An important limitation of our study is that we measured BP, IOP, and OAF velocity at a single time point during the day. There is evidence that BP variability and nocturnal hypotension, especially in treated hypertensives, play a role in the pathogenesis and progression of glaucomatous optic neuropathy and optic nerve ischemia.2–4,18,19,21 Hence, studies with 24-h measurements may be undertaken in future.
Another limitation is that color doppler imaging for estimating flow velocity has been criticized as a poor representation of actual flow as the diameter of the vessel is not measured. However, flow velocities measured by doppler were found to correlate well with blood flow in cerebral vessels, and hence our technique may be acceptable. 65 Though blood flow velocity is not a true measurement of flow volume, it may be the next best option due to the paucity of better techniques for retrobulbar flow measures.
Additionally, we did not study the smaller vessels (short posterior ciliary artery, central retinal artery) closer to the globe. It may be meaningful to evaluate any concomitant changes in the flow velocity of these vessels due to a decrease in the BP as a result of antihypertensive therapy. Our small sample size and short duration (1 month) of study is also a limitation. But since this was a preliminary evaluation, we plan to explore this further through more extensive studies.
The prevalence of systemic hypertension and glaucoma in the elderly is likely to increase as both increase with age.66–68 Our study suggests that a decrease in blood flow due to lowered BP contributed at least partially to a change in IOP, especially following oral beta-blockers. There is a chance these patients may be mislabeled as low-tension glaucoma. Further, these patients may require IOP monitoring on cessation or modification of antihypertensive treatment. Also, in patients already using oral beta-blockers for hypertension, topical beta-blockers may be of limited value due to the oral drug's beta-blockade activity at the ciliary body. The lower flow velocity in diastole following beta-blockers warrants further evaluation.
Our study focuses on a mechanistic background for the observed differences in ocular flow parameters and IOP related to aqueous humor production secondary to using 2 antihypertensives (atenolol and amlodipine). The use of antihypertensive medication may have broader effects on ocular perfusion and physiology beyond that suggested by our study, warranting further investigation.
Ethics Statement
The study was conducted after obtaining approval from the Institutional Ethics Committee of Indira Gandhi Government General Hospital and Post Graduate Institute (IGGGH&PGI), Puducherry, India (approval number: GHIEC2016), and it adhered to the tenets of the Declaration of Helsinki.
Consent to Participate/Publication
Informed consent was obtained from all individual participants included in the study. The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their clinical information to be reported for publication. The participants understand that their names and initials will not be published, and due efforts will be made to conceal their identity.
Data Availability Statement
Data pertaining to this study will be made available on request.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.