
Abstract
Purpose:
To investigate differences in the incidence of retinal fluid subtypes among different subtypes of macular neovascularization (MNV) and evaluate the influence of the presence of retinal fluid subtypes on visual outcome in each subtype of MNV.
Methods:
This retrospective study included 248 patients (248 eyes) diagnosed with treatment-naive neovascular age-related macular degeneration and polypoidal choroidal vasculopathy (PCV). The incidence of retinal fluid subtypes at diagnosis and during the 24-month follow-up was compared among the different subtypes of MNV. In addition, visual acuity was compared between patients with and without the retinal fluid subtypes.
Results:
At diagnosis, there was a significant difference in the incidence of subretinal fluid (SRF), intraretinal fluid (IRF), and subretinal pigment epithelial fluid among type 1 MNV, type 2 MNV, type 3 MNV, and PCV (P < 0.001). The incidence of SRF (P < 0.001) during follow-up also differed among the 4 groups. In patients with type 1 MNV and IRF, the visual acuity at diagnosis (P = 0.004) and at 24 months (P < 0.001) were significantly worse. However, the presence of SRF was not associated with poor visual acuity. In type 3 MNV, there was no significant difference in visual acuity between patients with and without SRF/IRF.
Conclusion:
The results of this study indicate that the clinical significance of retinal fluid subtypes may differ in different subtypes of MNV, suggesting the need for analysis in isolation of each MNV subtype in fluid-based prognostication.
Introduction
While treating neovascular age-related macular degeneration (AMD), various types of retinal fluid, including subretinal fluid (SRF), intraretinal fluid (IRF), and subretinal pigment epithelial (RPE) fluid can be encountered. 1 Because retinal fluid has generally been considered to reflect disease activity, the main purpose of treatment is resolving fluid based on optical coherence tomography (OCT)-guided measurements.2,3 In addition, fluid resolution is currently used as an important index to evaluate the response to anti-vascular endothelial growth factor (VEGF) treatment.4,5
With an increasing number of studies investigating the nature and clinical significance of retinal fluid, the influence of different types of retinal fluids on visual outcomes have been elucidated.1,6,7 For example, IRF has been associated with an unfavorable visual prognosis, whereas SRF is associated with a relatively favorable visual prognosis.1,7,8 Guymer et al. showed that small amounts of remaining SRF do not significantly influence the visual outcomes in a treat-and-extend regimen. 9
Despite progress in understanding the clinical significance of retinal fluid, the significance of retinal fluid subtypes in different types of macular neovascularization (MNV) has not yet been fully elucidated. However, because different types of MNV have different characteristics, it is possible that the clinical significance of retinal fluid subtypes could also differ among the different types of MNV. Recently, Sharma et al. also suggested that the significance of IRF and SRF in type 3 MNV may differ from that in other types of MNV. 10
In this study, we investigated the differences in the incidence of retinal fluid subtypes among different subtypes of MNV. In addition, the influence of the presence of retinal fluid subtypes on visual outcome was analyzed separately for each MNV subtype.
Methods
This retrospective observational study was conducted in a single center (Kim's Eye Hospital, Seoul, South Korea). The study was approved by the Institutional Review Board of Kim's Eye Hospital and conducted in accordance with the tenets of the Declaration of Helsinki.
Patients and treatment
This study included treatment-naive patients diagnosed with neovascular AMD or polypoidal choroidal vasculopathy (PCV) between January 2017 and December 2017. Additional inclusion criteria were as follows: (1) initially treated with 3 loading injections of intravitreal ranibizumab (0.5 mg/0.05 mL of Lucentis®; Genentech, Inc., San Francisco, CA) or aflibercept (2.0 mg/0.05 mL of Eylea®; Regeneron, Tarrytown, NY); (2) follow-up period of at least 24 months; and (3) availability of indocyanine-green angiography (ICGA) result at diagnosis.
The exclusion criteria were as follows: (1) history of vitreoretinal or glaucoma surgery; (2) inability to accurately classify the subtypes of MNV on the basis of OCT and ICGA results; (3) having undergone vitreoretinal surgery during the 24 months follow-up period; (4) did not visit the hospital for more than 6 months; (5) persistent vitreous hemorrhage that precludes accurate OCT examination; and (6) development of retinal detachment or macular hole. An eye with prior treatment was included when both eyes met the eligibility criteria.
Patients were initially treated with 3 loading injections of intravitreal ranibizumab or aflibercept. After the initial treatment, re-treatment was performed on an as-needed basis. One of 3 anti-VEGF agents ranibizumab, aflibercept, or bevacizumab (1.25 mg/0.05 mL of Avastin®; Genentech, Inc.) was used for re-treatment. In some patients, the treatment regimen was changed to treat-and-extend at the discretion of the attending physician.
Classification of MNV and retinal fluid subtypes
The type of MNV was classified based on OCT as follows (Fig. 1): type 1 MNV = sub-RPE MNV; type 2 MNV = subretinal MNV; and type 3 MNV = intraretinal MNV. Patients showing both type 1 and type 2 MNV features were classified as having type 2 MNV. Angiography images were used as adjuncts for this classification. PCV cases were identified based on the results of ICGA examination and analyzed separately. Retinal fluids at the fovea were classified based on OCT images as SRF, IRF, and sub-RPE fluid (Fig. 2). The presence of sub-RPE fluid was defined by the presence of serous PED. All the images were analyzed by a single experienced examiner (J.H.K.).

Representative fluorescein angiography
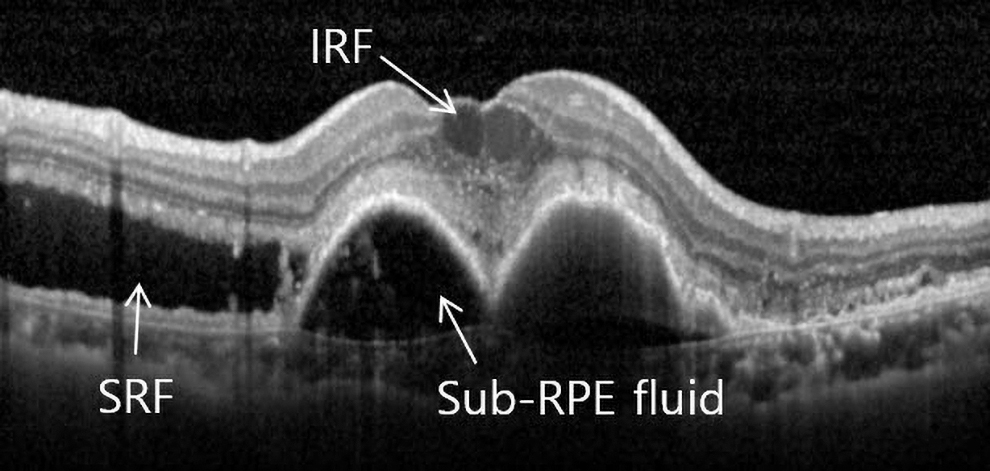
Representative figure showing IRF, SRF, and sub-RPE fluid. IRF, intraretinal fluid; SRF, subretinal fluid; RPE, retinal pigment epithelial.
Outcome measures
The incidence of each retinal fluid subtype (SRF, IRF, and sub-RPE fluid) at diagnosis and the proportion of retinal fluid subtypes on OCT examinations during follow-up were compared among the MNV types. The proportion was calculated as follows: the number of OCT examinations in which the presence of retinal fluid was identified/total number of OCT examinations performed during the follow-up period. In this analysis, OCT images obtained at diagnosis were excluded. Best-corrected visual acuity (BCVA) at diagnosis and at 24 months was compared between patients with and without each retinal fluid subtype. This analysis was undertaken for each type of MNV.
Patients who were initially treated with ranibizumab were included in the ranibizumab group, whereas those who were initially treated using aflibercept were included in the aflibercept group. The BCVA at diagnosis and that at 24 months were compared between groups.
To evaluate factors associated with visual outcome at 24 months, patients were divided according to the BCVA at 24 months into BCVA 20/40 or better versus BCVA worse than 20/40 groups. The association of the following factors with BCVA at 24 months was analyzed: type of fluid at baseline (presence of SRF vs. other), type of anti-VEGF agent for initial treatment, number of anti-VEGF injections during 24 months, and duration between the last injection and month 24.
Statistical analysis
Data are presented as mean ± standard deviation or number (%), where applicable. Visual acuity was measured using a decimal visual acuity chart and transformed to logarithm of minimal angle of resolution (logMAR) values for analysis. According to the suggestion of Holladay, 11 counting finger and hand motion visual acuities were transformed into logMAR values 2 and 3, respectively. Statistical analyses were performed using a commercially available software package (Statistical Package for the Social Sciences, SPSS, for Windows, version 21.0; IBM, Armonk, NY).
Comparisons among different MNV groups were undertaken using the Kruskal–Wallis test or chi-square test. Comparisons of visual acuity between patients with and without retinal fluid and between the ranibizumab and aflibercept groups were evaluated by the Mann–Whitney U-test with Bonferroni correction. The multivariate analysis was performed using binary logistic regression. Statistical significance was set at P < 0.05.
Results
During the study period, 380 patients were diagnosed with treatment-naive neovascular AMD and PCV and received 3 loading injections of anti-VEGF. Among them, 132 (34.7%) were excluded for the following reasons: follow-up period less than the specified duration of 24 months (70 patients), unavailability of ICGA results or inability to accurately classify the subtype of MNV based on OCT and angiography results (45 patients), history of vitreoretinal surgery or glaucoma surgery (2 patients), having undergone vitreoretinal surgery during the 24 months follow-up period (4 patients), did not visit the hospital for >6 months (8 patients), persistent vitreous hemorrhage that precludes accurate OCT examination (2 patients), development of macular hole (1 patient).
Ultimately, the results were analyzed for 248 patients (248 eyes) who satisfied the inclusion criteria (Table 1). The mean age of the patients was 70.6 ± 8.4 years. Seventy-nine (31.9%) patients were diagnosed with type 1 MNV, 45 (18.1%) had type 2 MNV, 26 (10.5%) had type 3 MNV, and 98 (39.5%) were diagnosed with PCV.
Baseline Characteristics of Patients Included in the Study (N = 248)
MNV, macular neovascularization; RPE, retinal pigment epithelium; logMAR, logarithm of minimal angle of resolution; VEGF, vascular endothelial growth factor.
Figure 3 shows the incidence of each retinal fluid subtype at diagnosis according to the type of MNV. In type 1 MNV, SRF was noted in 45 patients (56.9%), IRF in 10 patients (12.7%), and sub-RPE fluid in 29 patients (36.7%). Whereas the number of patients with type 2 MNV in these 3 subtypes was 13 (28.9%), 16 (35.6%), and 5 (11.1%), respectively, there were 3 (11.5%), 23 (88.5%), and 10 (38.5%) patients with type 3 MNV, respectively. One patient exhibited SRF without IRF. In the PCV group, the subtype was seen in 64 (65.3%), 10 (11.2%), and 25 (25.5%) patients, respectively. There was a significant difference in the incidence of SRF at diagnosis among the 4 MNV types (P < 0.001). The incidence of IRF at diagnosis (P < 0.001) and sub-RPE fluid at diagnosis (P = 0.011) also significantly differed among the 4 MNV types.
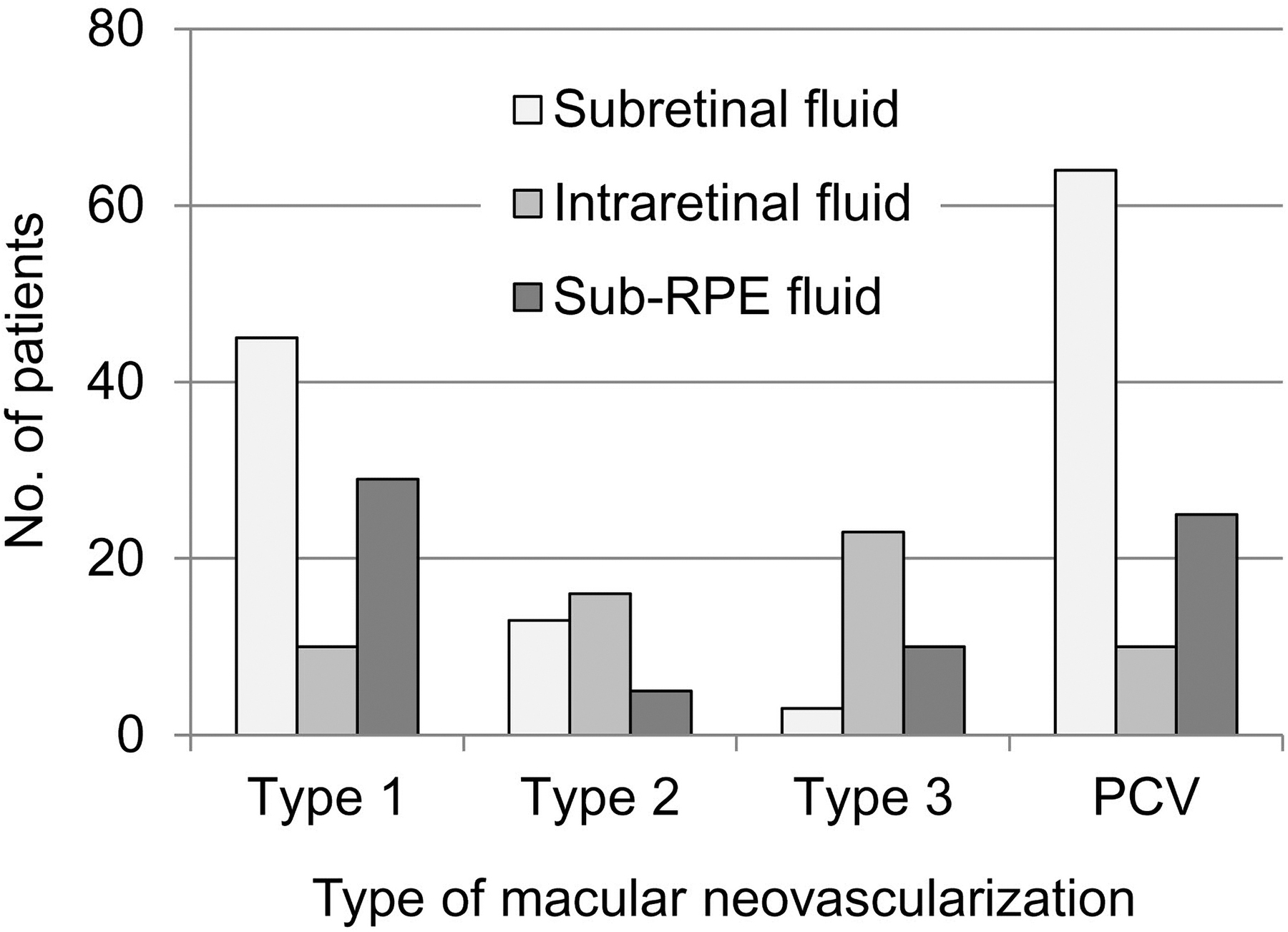
Incidence of retinal fluid subtypes, according to the type of macular neovascularization. PCV, polypoidal choroidal vasculopathy.
At 3 months, the mean logMAR BCVA was measured as 0.39 ± 0.39. All SRF, IRF, and sub-RPE fluids were completely resolved in 185 patients. Among the remaining 63 patients, SRF, IRF, and sub-RPE fluid remained in 43 (68.3%), 8 (12.7%), and 27 (42.9%), respectively. During the 24-month follow-up period, a mean 6.6 ± 3.0 anti-VEGF injections were performed per patient. Among them, 61 received only 3 anti-VEGF injections and the remaining 187 patients received a mean 7.8 ± 2.5 injections during the follow-up period. The mean duration between the last injection and month 24 was 9.2 ± 8.4 months.
Fluid status at 24 months was as follows. In patients with type 1 MNV, SRF was noted in 29 (36.7%), IRF in 11 (13.9%), and sub-RPE fluid in 11 (13.9%). In patients with type 2 MNV, SRF was noted in 9 (20.0%), IRF in 15 (33.3%), and sub-RPE fluid in 2 (4.4%). In patients with type 3 MNV, SRF was noted in 2 (7.7%), IRF in 2 (7.7%), and sub-RPE fluid in 1 (3.8%). In patients with PCV, SRF was noted in 38 (38.8%), IRF in 19 (19.4%), and sub-RPE fluid in 16 (16.3%).
During the 24 months follow-up period, mean 11.8 ± 2.9 OCT examinations were performed in type 1 MNV, 9.8 ± 3.4 in type 2 MNV, 11.2 ± 3.3 in type 3 MNV, and 10.6 ± 3.1 in PCV. Table 2 summarizes the proportion of the presence of each retinal fluid subtype during the follow-up period. The proportion of SRF was 25.8% ± 29.8% in type 1 MNV, 12.3% ± 19.8% in type 2 MNV, 6.3% ± 19.4% in type 3 MNV, and 24.4% ± 28.6% in PCV. The proportion of IRF was 8.5% ± 15.6% in type 1 MNV, 11.5% ± 18.9% in type 2 MNV, 15.0% ± 15.7% in type 3 MNV, and 10.3% ± 21.3% in PCV. The proportion of sub-RPE fluid was 13.8% ± 26.2% in type 1 MNV, 0.2% ± 1.3% in type 2 MNV, 5.2% ± 7.6% in type 3 MNV, and 8.3% ± 20.7% in PCV.
Difference in the Proportion of Presence of Retinal Fluid Subtypes in Follow-Up Optical Coherence Tomography Examinations Among the Different Types of Macular Neovascularization
Kruskal–Wallis test.
Values represent mean ± standard deviation.
PCV, polypoidal choroidal vasculopathy.
As seen in the table, there was a significant difference in the proportion of the presence of SRF during the follow-up period among the 4 MNV types (P < 0.001). The proportion of patients with sub-RPE fluid also significantly differed among the 4 MNV types (P < 0.001). However, the difference in the proportion of patients with IRF among the 4 MNV types was not significant (P = 0.084).
In type 1 MNV, BCVA at diagnosis were significantly better in patients with SRF than in those without it (P = 0.002). The BCVA at 24 months was also significantly better in patients with SRF (P = 0.014) (Table 3). The BCVA at diagnosis was significantly better in patients without IRF than in those with it (P = 0.004). The BCVA at 24 months was also significantly better in patients without IRF (P < 0.001). Regarding type 2 MNV, BCVA at diagnosis was significantly better in patients with SRF than in those without it (P = 0.012) (Table 4). However, for type 3 MNV, there was no significant difference in BCVA between patients with and without each retinal fluid subtype (Table 5). In patients with PCV, the BCVA at diagnosis was significantly better in patients with SRF than in those without it (P < 0.001) (Table 6).
Comparison of Best-Corrected Visual Acuity Between Patients With and Without Each Retinal Fluid Subtype at Diagnosis in Type 1 Macular Neovascularization (n = 79)
Visual acuities are presented as logarithm of the minimal angle of resolution value.
Mann–Whitney U-test with Bonferroni correction.
Values represent mean ± standard deviation.
RPE, retinal pigment epithelium.
Comparison of Best-Corrected Visual Acuity Between Patients With and Without Each Retinal Fluid Subtype at Diagnosis in Type 2 Macular Neovascularization (n = 45)
Visual acuities are presented as logarithm of the minimal angle of resolution value.
Mann–Whitney U-test with Bonferroni correction.
Values represent mean ± standard deviation.
Comparison of Best-Corrected Visual Acuity Between Patients With and Without Each Retinal Fluid Subtype at Diagnosis in Type 3 Macular Neovascularization (n = 26)
Visual acuities are presented as logarithm of the minimal angle of resolution value.
Mann–Whitney U-test with Bonferroni correction.
Values represent mean ± standard deviation.
Comparison of Best-Corrected Visual Acuity Between Patients With and Without Each Retinal Fluid Subtype at Diagnosis in Polypoidal Choroidal Vasculopathy (n = 98)
Visual acuities are presented as logarithm of the minimal angle of resolution value.
Mann–Whitney U-test with Bonferroni correction.
Values represent mean ± standard deviation.
Ninety-three patients were included in the ranibizumab group versus 155 patients in the aflibercept group. In the ranibizumab group, the mean logMAR BCVA was 0.52 ± 0.45 at diagnosis versus 0.49 ± 0.45 at 24 months. In the aflibercept group, the values were 0.59 ± 0.49 and 0.49 ± 0.47, respectively. There was no intergroup difference in the BCVA at diagnosis (P = 0.470) versus at 24 months (P = 1.000).
In the multivariate analysis, the duration between the last injection and month 24 was significantly associated with BCVA at 24 months (P = 0.032) in type 1 MNV. There were no other significant factors. In type 2 MNV, type 3 MNV, and PCV, no factor was significantly associated with BCVA at 24 months.
Discussion
The primary findings of this study were 2-fold. First, it was observed that there was a difference in the incidence of retinal fluid subtypes both at diagnosis and during follow-up among the different types of MNV. Second, the findings suggested that the influence of the presence of the retinal fluid subtype on visual outcome differed among the different types of MNV.
It is well known that the retinal fluid subtypes are associated with different visual outcomes. This difference was particularly noted between SRF and IRF. In a study by Jaffe et al., 7 patients with foveal SRF showed relatively better visual acuity than in those without it. In contrast, as compared with patients without foveal IRF, a relatively inferior visual acuity was seen in patients with foveal IRF. This trend continued throughout the 52-week follow-up period. In a study by Regillo et al., the presence of SRF at baseline was associated with better visual acuity at 12 months. 12 In another study the presence of SRF was associated with favorable visual outcomes, and IRF was linked with unfavorable visual outcomes. 13
More recently, Saenz-de-Viteri demonstrated that patients with SRF at the loading phase showed better visual outcomes than patients with IRF, 14 and the persistence of SRF did not affect visual outcomes. It has also been documented that the visual acuity was well maintained in patients with SRF refractory following monthly injections of ranibizumab. 15 However, patients with refractory IRF had a higher risk of visual deterioration. A recent clinical trial by Guymer et al. demonstrated that treating patients using a treat-and-extend regimen and allowing ≤200 μm of foveal SRF did not significantly influence treatment outcomes. 9
Based on these observations, the concept “Small amount of SRF can be tolerated” has been proposed,7,9 and is currently one of the important issues in retinal research.16,17 However, several recent studies also showed that the SRF was related to poor visual outcomes.18,19 To date, consensus is lacking about whether SRF can be tolerated.
For this study, the influence of retinal fluid subtypes at diagnosis on visual outcomes was analyzed separately according to the subtype of MNV. In type 1 MNV, the better visual acuity at diagnosis and 24 months in patients with SRF and those without IRF were in agreement with those reported in previous studies. With respect to type 3 MNV, however, neither SRF nor IRF could be significantly associated with visual outcome. Unlike type 1 or 2 MNV, which originate from the choroid, type 3 MNV originate from the retina.20,21 Thus, IRF can develop before the development of SRF, suggesting that the presence of IRF may not indicate advanced disease and profound retinal damage.
Recently, Sharma et al. discussed this issue and suggested that type 3 MNV need to be separately analyzed in fluid-based prognostication in neovascular AMD. 10 We believe that the results of this study support this suggestion.
As type 3 MNV originates from the retina and progresses toward the choroid, the presence of sub-RPE fluid indicates the advanced from of the disease. 22 In this study, however, no difference in visual outcomes was noted between patients with and those without sub-RPE fluid at diagnosis. We postulate that the study design influenced this result. Because only the subfoveal fluids were evaluated in this study, the presence of sub-RPE fluid without foveal involvement was considered an absence of sub-RPE fluid.
As type 3 MNV lesions usually develop at the extrafoveal location, 23 sub-RPE fluid may not always involve the fovea. For this reason, the results of this study may not accurately reflect the degree of disease progression. Sharma et al. recently reported an association between isolated IRF and good visual acuity in type 3 MNV. 24 In that study, all fluids were evaluated regardless of location. We believe that this difference in study design explains the variation in the results between this study and that of Sharma et al. 24
In this study, the incidence of each retinal fluid subtype in PCV was similar to that observed in type 1 MNV. This is not surprising as PCV can be included in the spectrum of type 1 MNV. 25 Similar to type 1 MNV patients, PCV patients with SRF showed significantly better BCVA at diagnosis than those without SRF.
In addition to its association with a relatively favorable visual outcome compared with IRF, SRF has also been found to be associated with a low risk of macular atrophy (MA).26,27 Although the exact reason for these associations is unclear, several investigators have suggested that SRF is protective against the development of MA or it contains neuroprotective substances.26,28
In this study, the incidence of SRF at diagnosis was markedly higher in type 1 MNV than in type 2 or type 3 MNV. In addition, in type 1 MNV, SRF was found to be the main type of retinal fluid observed during the follow-up period. Although, in type 2 MNV, the proportion of SRF was comparable with that of IRF in lesion reactivation, in type 3 MNV, IRF was the main type observed during the follow-up period. Collectively, these findings suggest that when all types of MNV are analyzed together, the nature of type 1 MNV can influence the outcomes of analysis related to SRF.
In general, type 1 MNV shows relatively favorable visual prognosis and less progression of MA than other types of MNV.29,30 Investigators have suggested that the presence of type 1 MNV itself or its evolution into a multilayered pigment epithelial detachment (PED) may support the outer retina and decrease the risk of MA.31–33 Because SRF is frequently noted in type 1 MNV, it is possible that the nature of type 1 MNV may have some influence on the association of SRF with favorable visual outcome and low risk of MA. We suggest that separate analysis within each type of MNV be undertaken for a better understanding of the clinical significance of retinal fluid subtypes.
When compared with SRF and IRF, the clinical significance of sub-RPE fluid has not yet been fully established. In general, sub-RPE fluid is not considered to be closely associated with visual outcomes. In the study by Jaffe et al., patients with and without sub-RPE fluid showed similar visual acuity, 7 whereas in another study, 34 PED status and height at baseline did not significantly influence the visual outcome. A recent review compiled on previous PED studies recommended treatment of cases in which IRF and/or SRF were concurrently detected. 35 Although the clinical significance of PED, such as the association between an increase in PED and secondary cystoid degeneration has been demonstrated by several researchers, 36 there is no firm evidence to suggest any positive or negative impact of sub-RPE fluid on visual outcome. In this study, sub-RPE fluid was most frequently noted in type 1 MNV, followed by type 3 MNV. However, there was no difference in visual outcome according to the presence of sub-RPE fluid in all types of MNV.
In the multivariate analysis, the duration between the last injection and month 24 was significantly associated with BCVA at 24 months in type 1 MNV. Patients without lesion reactivation after the initial loading injections may show a longer duration between the last injection and month 24 than patients with lesion reactivation. This may influence the association found in the multivariate analysis.
This study has some limitations. First, this was a retrospective study based on data from a real-world setting. Thus, the treatment and follow-up schedules could not be controlled, and some of our patients might have been undertreated. Second, although the total number of patients was sufficiently large, a relatively small number of patients were included in each MNV group, especially in the type 2 and type 3 MNV groups. Thus, the results for type 2 and type 3 MNV groups obtained in this study need to be verified by further studies with larger study populations in each group. Third, a substantial number of patients (34.7%) were excluded from the study for various reasons, suggesting that selection bias may have influenced the study results. Fourth, a single examiner performed all the image analyses. Therefore, the influence of bias in image analysis cannot be ignored.
Fifth, different types of anti-VEGF agents were used. However, because the treatment outcomes were generally similar among the different anti-VEGF agents, 37 utilization of a different agent might not significantly influence the study result. Sixth, in this study, the presence of a certain fluid type was identified regardless of presence of other fluid types. For this reason, the association of isolated SRF, IRF, or sub-RPE fluid with visual outcomes could not be analyzed. Finally, all included patients were Korean. Because the proportion of each type of MNV may differ across different ethnic groups, further studies with other ethnic groups are warranted to verify whether the conclusions drawn from this study can be broadly adopted.
In summary, this study evaluated the differences in the incidence of retinal fluid subtypes and their association with visual outcomes among different types of MNV. The incidence of SRF at diagnosis and during the follow-up period was markedly higher in type 1 MNV than in type 2 or type 3 MNV. In addition, the association between the visual acuity and the presence of each retinal fluid subtype differed among the different MNV types. The results suggest that the clinical significance of retinal fluid subtypes may differ among different subtypes of MNV. The results also highlight the requirement of isolated analysis of each type of MNV in fluid-based prognostication.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Kim's Eye Hospital Research Center.