
Abstract
Purpose:
Our aim was to evaluate the effects of topical antiglaucomatous medications on conjunctival thickness using anterior segment optical coherence tomography (AS-OCT).
Methods:
Thirty eyes of 30 patients with primary open angle glaucoma, who had never used any antiglaucomatous medications, enrolled in this prospective study. Followed by a full ophthalmologic examination, the conjunctival thickness was measured before treatment and at 1, 3, and 6-month post-treatment by AS-OCT. Measurements were taken from the superior bulbar conjunctiva, 3–4 mm from the limbus.
Results:
The mean age of patients was 67.7 ± 8.6; fourteen cases (46.7%) were given latanoprost, 2 cases (6.7%) brinzolamide+timolol, 2 cases (6.7%) betaxolol, 4 cases (13.3%) travoprost, and 8 cases (26.7%) brimonidine. The mean baseline conjunctival thickness was 222.9 ± 38 μm, while the mean conjunctival thickness was 212.8 ± 36.0 μm in the first month, 198.2 ± 35.8 μm in the third month, and 187.5 ± 40.2 μm in the sixth month. Decrease in conjunctival thickness at each examination was statistically significantly compared to baseline. (P < 0.05) Decrease in conjunctival thickness in Latanoprost subgroup was statistically significant, whereas the decreases in other active ingredients were not.
Conclusion:
Topical antiglaucomatous medications especially prostaglandin analogs may affect conjunctival thickness even during the first few months. This thinning effect may be crucial for the conjunctiva, as the basis of the possible filtration surgery.
Introduction
Glaucoma is a multifactorial, progressive optic neuropathy and is one of the most common causes of irreversible blindness. 1 Intraocular pressure (IOP) is the major manageable risk factor for glaucomatous optic nerve damage - so the primary goal of glaucoma treatment is to reduce IOP.1,2
However, adverse effects of topical antiglaucomatous medications on the ocular surface have been demonstrated in many studies.3–6 As is known, the conjunctiva is a passive, semipermeable, natural barrier for topical medications. 3 The factors associated with these medications, such as type of active compound and preservative, duration of treatment, frequency of application, and physical properties (temperature, concentration, pH value, toxicity), have well-known effects on the conjunctiva. 6
It is observed that long-term usage of topical antiglaucomatous medications increases the risk of subconjunctival fibrosis, given the effect of the active compound and/or the drug preservative, such that bleb life is shortened in eyes undergoing glaucoma filtration surgery. 5
Anterior segment optical coherence tomography (AS-OCT) was used in the diagnosis and follow-up of glaucoma, including corneal and conjunctival diseases. It can be used for the follow-up of trabeculectomy bleb morphology, diagnosis and follow-up of keratoconus, evaluation of intracorneal ring position, and diagnosis of corneal dystrophies.7–14
In this study, we used AS-OCT in newly diagnosed glaucoma patients to analyze the effect of antiglaucomatous medications on the conjunctiva, with a large area on the ocular surface, which acts as a base for filtration surgery.
Methods
This prospective study was conducted in the Glaucoma Department of the University of Health Sciences, Turkey; Beyoglu Eye Training and Research Hospital; and in accordance with the principles of the Declaration of Helsinki. Informed consent was obtained from all patients. The study was approved by the University of Health Sciences, Istanbul Training and Research Hospital Ethics Committee, Decision no. 1845.
Case selection
Consecutive patients with newly diagnosed primary open angle glaucoma (POAG) were included in the study between May 2018 and May 2019.
Patients who received any eyedrops, including antiglaucomatous treatment beforehand, patients using steroids or had previous ocular surgery (including cataract surgery), or those with conjunctival pathology, pseudoexfoliation, uveitis, and patients whose refractive error was outside ±3.00 diopter were not included in this study. Patients prescribed additional topical medication or switched to another drug due to an allergic effect or those who underwent ocular surgery in the follow-up period were excluded. Only one eye of each patient was included in the study.
Routine ocular examination, including determination of the best-corrected visual acuity with a Snellen chart, slit-lamp examination, IOP measurement with the Goldmann applanation tonometry, and a dilated fundus examination with a 90 D lens were performed, and an automated static visual field test, along with cornea, conjunctiva, and peripapillary retinal nerve fiber layer thickness measurements, was evaluated using OCT at each visit.
OCT analysis
Superior bulbar conjunctival thickness (epithelium and stroma thickness) at a distance of 3–4 mm from the limbus was measured by AS-OCT before treatment and at 1, 3, and 6 months after initiation of antiglaucomatous eyedrop treatment. Three measurements were taken from the superior bulbar conjunctiva at 12 o'clock meridian, and the mean value was recorded (Fig. 1). We used the Spectralis OCT (Heidelberg Engineering GmbH, Torrance, CA) device and could obtain high-resolution measurements by adapting the add-on lens of the anterior segment module to the device. 15 All measurements were taken by a blinded physician (G.K.) who had no knowledge of the treatment of patients. Patients were asked to look down, after their chin and forehead were placed, with the upper eyelid retracted.
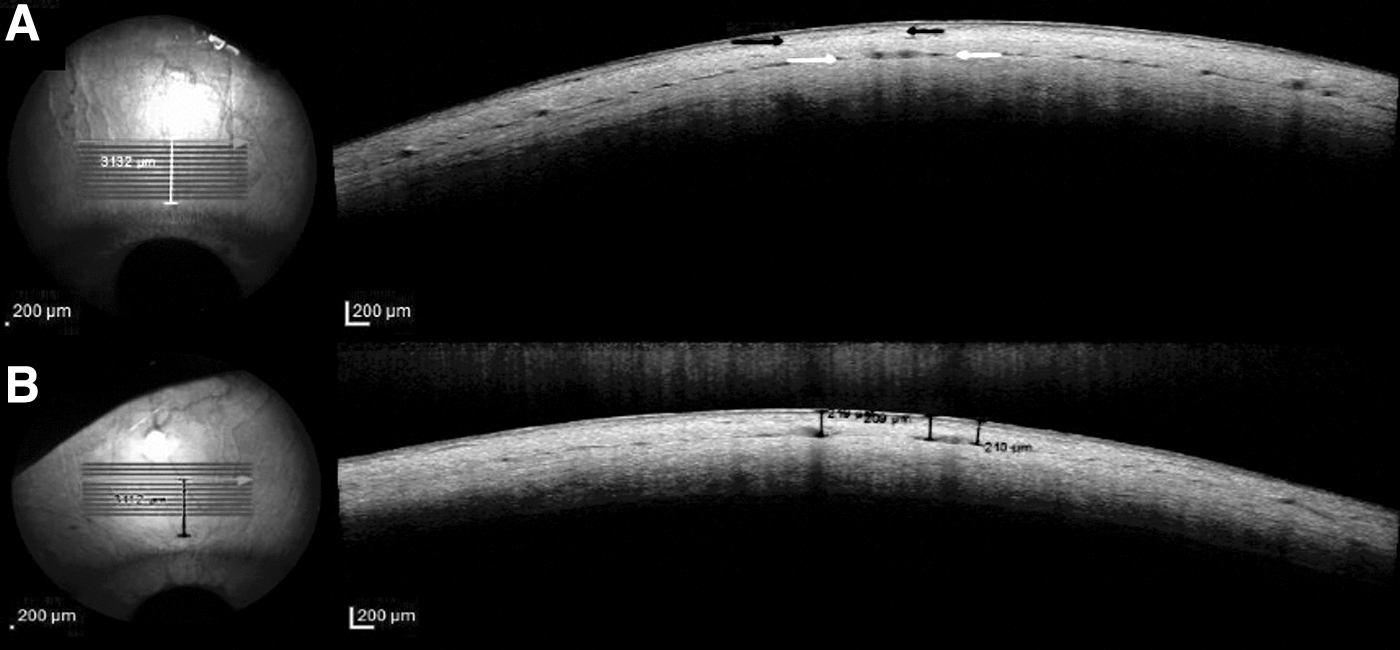
The conjunctival epithelium is observed as a slightly hyporeflective thin band beneath the tear film layer. The stroma, beneath the epithelium but above the Tenon, is more hyperreflective. The Tenon layer shows relatively lower reflectance compared to the conjunctival stroma. As shown in Fig. 1, we distinguish the stroma and Tenon layer from the thin demarcation line formed by loose connective tissue in between.16,17 The presence of cyst-like spaces helps find the posterior border of the stroma. 7
Statistical analyses
Statistical analyses were conducted with the SPSS (Statistical Package for Social Science) v. 22.0 (SPSS, Inc., Chicago, IL) program. In the descriptive statistics of the data is the mean, standard deviation, lowest median, highest frequency, and ratio value. The distribution of variables was measured by the Kolmogorov–Smirnov test. Wilcoxon test was used for analysis of quantitative dependent data. Mann–Whitney U test was used for analysis of quantitative independent data. Correlation of continuous variables was analyzed with Spearman's rho coefficient.
Results
Demographic and clinical data are summarized in Table 1. Mean age was 67.1 ± 8.6 years: 14 (46.7%) patients were female, 16 (53.3%) were male.
Demographics and Baseline Data
RNFL, retinal nerve fiber layer.
The mean IOP was 22.5 ± 7.4 mmHg before treatment. After antiglaucomatous treatment, the mean IOP was 14.6 mmHg at 1 month, 13.7 mmHg at 3 months, and 13.1 mmHg at 6 months. We reached the target IOP with first-line therapy in all cases during follow-up; cases receiving additional medications were excluded from the study. The distribution of active compounds of the drugs and preservatives are shown in Table 2. Latanoprost was the most used active substance, while benzalkonium chloride (BAC) was the most used preservative in the study.
The Distribution of Antiglaucomatous Eyedrops
Conjunctival thickness measurements during the follow-up period are shown in Table 3 and Fig. 2. The mean conjunctival thickness was 222.9 ± 38 μm before treatment, 212.8 ± 36.0 μm at 1 month, 198.5 ± 35.8 μm at 3 months, and 187.5 ± 37.7 μm at 6 months. A scatter plot regarding the conjunctival change of 30 patients at each period is represented in Fig. 3.
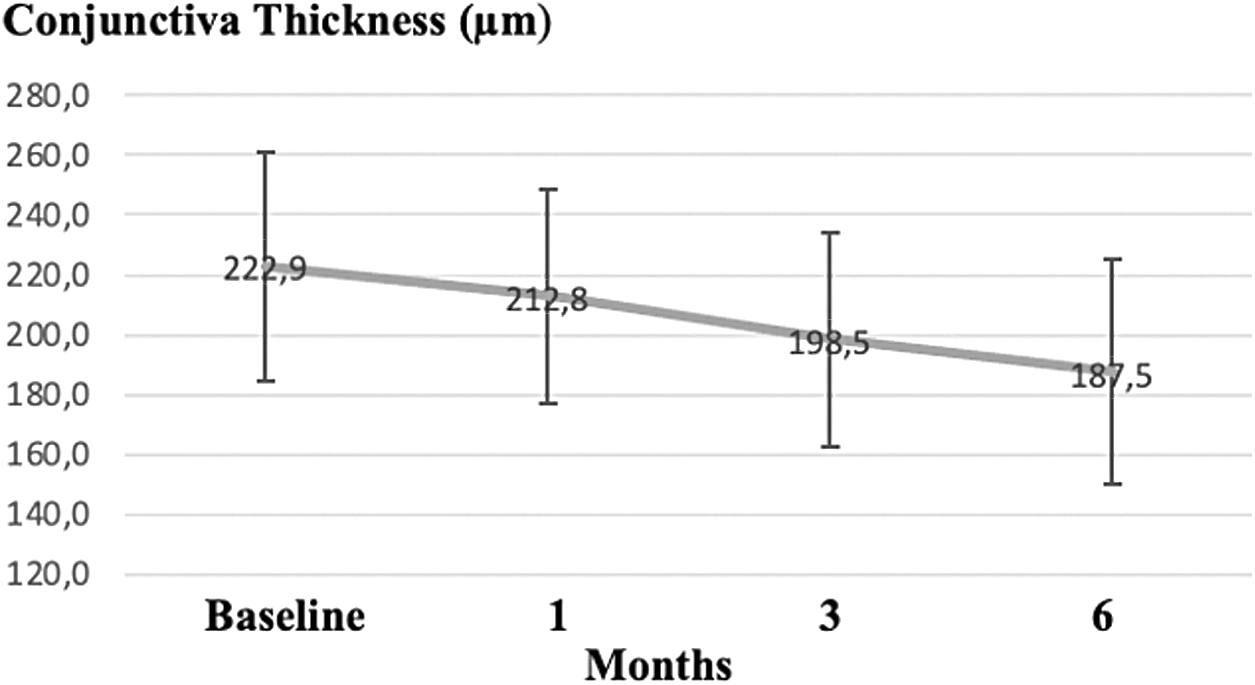
Total conjunctival thickness change over time.
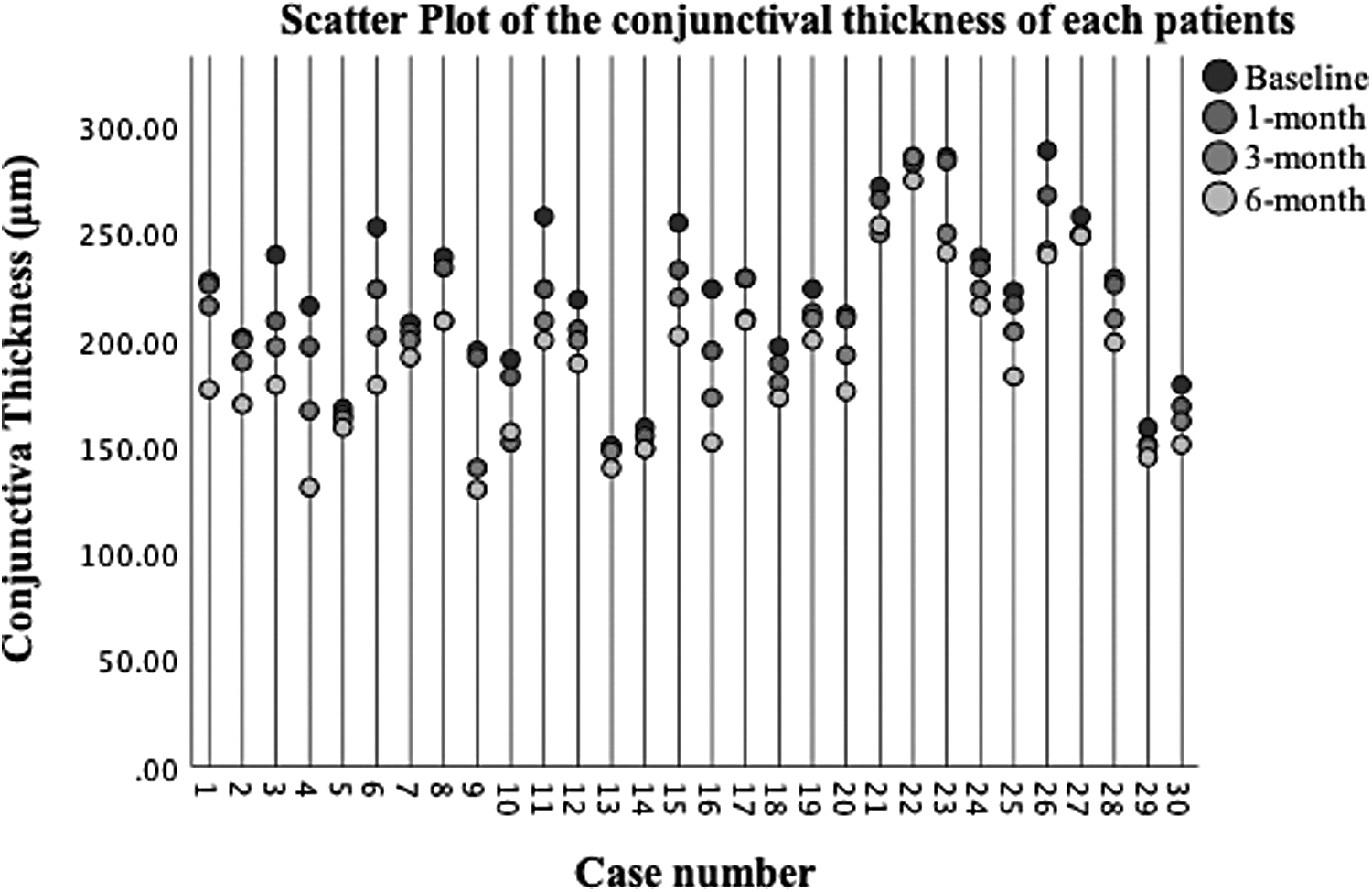
A scatter plot of the conjunctival thickness of each patient.
Total Conjunctival Thickness Measurements
Wilcoxon test.
Difference compared to baseline.
Difference compared to previous value.
SD, standard deviation.
The full thickness of the conjunctiva decreased significantly (P < 0.05) at 1, 3, and 6 months compared to baseline. We observed a significant decrease at 3 months compared to 1 month and also at 6 months compared to 3 months. (P < 0.05)
The correlation analysis was performed, and no statistically significant correlation was found between IOP change and conjunctival thickness change at 1, 3, and 6 months.
Descriptive statistics of medications with baseline and 6-month relative results are given in Table 4. There was a statistically significant decrease in total conjunctival thickness in Latanoprost group and no statistically significant change in other medications.
Descriptive Statistics of All Medications with Baseline and 6-Month Conjunctival Thickness Measurements
Wilcoxon Signed Rank Test.
As shown in Table 5, we divided into 2 subgroups: Prostaglandin (PG) analogues and Other drugs and observed a significant decrease in 6 months compared to baseline in both groups.
Baseline and 6-Month Conjunctival Thickness Measurement Statistics of Prostaglandin Analogs and the Other Drugs
Mann–Whitney U test.
Wilcoxon test.
We divided the preservative contents into subgroups as BAC and others (purite, polyquad). In both subgroups, the full thickness decreased significantly at 1, 3, and 6 months compared to baseline (Table 6).
Preservative Grouping as: Benzalkonium Chloride and Others
Mann–Whitney U test.
Wilcoxon test.
The correlation analysis was performed, and no statistically significant correlation was found between IOP change and conjunctival thickness change at 1, 3, and 6 months.
Discussion
With widespread use of AS-OCT, it is possible to provide noncontact high axial resolution images of anterior segment tissues, such as the conjunctiva, to observe its layers. 15 In this study, we measured the sum of the conjunctival epithelium and stromal thickness using AS-OCT in POAG cases in whom antiglaucomatous medication was first initiated and compared during the follow-up. Although there are a few studies comparing the conjunctival thickness of glaucoma patients to the healthy control group, we aimed to compare the measurements of the same patient before and at 1, 3, and 6 months of treatment.7,18
In this prospective study, we observed a statistically significant decrease in the conjunctival thickness at each examination compared to the baseline.
There are many studies in the literature showing effects of topical antiglaucomatous medications on the conjunctiva and ocular surface.3–6,19,20 Sherwood et al. reported a significant increase in the number of macrophages, lymphocytes, mast cells, and fibroblasts and a significant decrease in epithelial Goblet cells in the conjunctiva and Tenon in the group receiving antiglaucomatous eyedrops on a long-term basis. 5
In the study of Broadway et al. 3 it was observed that beta blockers as monotherapy had little effect on conjunctival cell profiles: they observed a significant increase in epithelial macrophages, fibroblasts, and mast cells in the substantia propria, following the combination with pilocarpine. Inflammatory effects were significantly increased with triple combination therapy, in which sympathomimetics were added 3 ; they could affect conjunctival structure and resistance, as they could also impact its thinning.
It has been reported that the effects of antiglaucomatous eyedrops on the ocular surface are also related to the balance between matrix metalloproteinases (MMP) and tissue inhibitors of MMP, causing extracellular matrix (ECM) degradation. 21 In a study of Mietz et al., MMP-3 upregulation was observed in latanoprost-treated eyes, which may cause ECM degradation. 22 In another immunohistochemical animal study for 3 months, it was observed that subepithelial collagen was greater in the group treated with antiglaucomatous drops, combined with preservatives. 23 The majority of patients used antiglaucomatous drops containing BAC as a preservative in the present study. In both BAC and other preservatives groups, the full thickness decreased significantly at 1, 3, and 6 months compared to baseline.
In a retrospective study by Tekin et al., conjunctiva full thickness of 49 eyes in 31 patients on antiglaucomatous medications for at least 6 months, compared to 51 eyes in the healthy control group, was compared by AS-OCT. In their study, the mean conjunctival thickness was 182.76 ± 26.77 μm in the patient group and 235.02 ± 26.26 μm in the control group. 18 The mean conjunctival thickness at last follow-up (6 months) was 187.5 ± 37.7 μm in our study. However, this was similar to the patient group average, but is a bit higher in our study. This may be related to the longer duration of treatment in their study (22.2 ± 7.4 months).
Despite reporting an inverse relationship between the duration of eyedrop use and total conjunctival thickness, it is unclear how it may decrease with long-term use. 18 In our clinical opinion, it may remain constant after reaching a certain level. This may explain why the mean thickness at last follow-up in our study versus Tekin's patient group average was close, although drug exposure was much longer in their study.
Zhang et al. measured bulbar conjunctival epithelial, stromal, and full thickness using AS-OCT and investigated whether these values varied with age and gender. 16 The average patient age in their study was 46.5; the mean conjunctival epithelial thickness was 42.46 ± 7.4 μm; stromal thickness was 197.76 ± 32.5 μm; and full thickness was 240.16 ± 29.8 μm. They observed that epithelial, stromal, and total bulbar conjunctival thickness did not show a significant difference between male and female groups, as stromal and total thickness of the conjunctiva gradually decreased with age. 16 In the present study, the mean conjunctiva full thickness before treatment (222.9 ± 38 μm) was thinner than theirs. With regard to this study, the higher mean age (67.1 ± 8.6) may support our lower baseline values. Increased inflammatory cells and metalloproteinase activity in the conjunctival stroma, with aging, may similarly increase proteolytic activity and lead to apoptosis. 24
In a prospective study involving 67 eyes of 67 patients, preoperative conjunctival thickness of glaucoma patients, undergoing filtration surgery, was measured using AS-OCT, with the relationship between surgical results analyzed. In the case group, filtration surgery failed; conjunctival epithelium, stroma, and full thickness were lower than other groups. Yet, the conjunctival epithelium was thicker, while the stroma was thinner in the study group, compared to the healthy control group in their study. 7
Previous retrospective studies show the increase of conjunctival epithelial thickness and the decrease of stromal and full thickness in glaucoma patients.7,18 Nuzzi et al. reported a significant increase in conjunctival epithelial thickness and number of epithelial layers in the group using antiglaucomatous medications. 25 This suggests that epithelial thickening is due to epithelial spongiosis and increased mitosis. They observed an increase in the number of fibroblasts in the subepithelial and deep connective tissue, with changes in collagen structure. 25 Increased fibroblastic activity in collagen organization may lead to remodeling, causing stromal thinning.
Li et al. reported a significant decrease in conjunctival thickness with long-term use of Latanoprost. 26 In the present study, we observed a statistically significant decrease in conjunctival thickness in Latanoprost group. The decrease in other medications was not statistically significant. However, we observed a value (0.068) very close to the significance level in Travoprost group. This may be attributed to the low number of patients in Travoprost group. Thus, it may be declared that PG analogs take the lead in the conjunctival thinning.
Recent AS-OCT studies show that long-term use of antiglaucomatous drops may change conjunctival structure and increase bleb failure.6,7,18 Mastropasqua et al. reported new predictive values: preoperative conjunctival thickness and higher reflectivity-indicating collagen fiber density in AS-OCT for filtration surgery outcomes. Full conjunctival thickness was the strongest predictor, with about an 8% increased risk of failure for each micron decrease in total thickness. 7 Reduced preoperative conjunctival thickness and an altered cellular conjunctival profile may cause bleb failure in filtration surgery.
However, this study has some limitations. The sample size was limited due to the selection of naive POAG cases who did not undergo any surgery or use topical medications in advance. The most suitable treatment was initiated for patients, depending on their clinical history and ophthalmological examinations. There was also a wide choice of drugs; a study with a larger group could provide effective results. Since preservative-free antiglaucomatous medications are not available in our country, all patients used drugs that were combined with preservatives.
Since the drug we use most in this study was latanoprost which contains BAC as a preservative, the separate effect of the preservative in drops on conjunctival thickness is not yet known. Moreover, the baseline values were statistically different in the preservative subgroups. Therefore, the preservative subgrouping does not provide any valuable data in this study.
Recently, evaluation of conjunctival structure using AS-OCT has been a topic of interest. Although the previous studies have shown the microscopic structural changes in conjunctiva with long-term use of topical antiglaucomatous drops, this study contributes to the literature in terms of comparing the pre- and postmedication conjunctival thickness of each newly diagnosed glaucoma patient.
Regardless of the follow-up period, there was a statistically significant decrease in conjunctival thickness compared to baseline, in the present study.
In conclusion, we emphasize that antiglaucomatous drugs, PG analogs in particular, which are thought to have a thinning effect in long-term use, can also decrease the conjunctival thickness even in the early stages. These early and structural changes may be crucial for the conjunctiva, which is essential for possible filtration surgery in POAG patients.
Ethics Statement
This study was approved by the University of Health Sciences, Istanbul Training and Research Hospital Ethics Committee, Decision No. 1845, May 24, 2019, in accordance with the Declaration of Helsinki.
Footnotes
Author Disclosure Statement
The authors declare that there is no conflict of interest.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.