
Abstract
Purpose:
To determine the pharmacokinetics of a proprietary liposomal sirolimus (LS) formulation in ocular tissues and plasma following a single subconjunctival (SCJ) injection in Dutch belted rabbits (DBR). Analytical methods for detection of LS in plasma, aqueous humor (AH), vitreous humor (VH), retina, combined retina/choroid/retinal pigment epithelium, sclera, and iris/ciliary body were developed to examine samples.
Methods:
Thirty male DBR were subconjunctivally injected in both eyes with 0.1 mL of LS of 1,000 μg/mL. At selected times post-injection, ocular tissues and whole blood samples were obtained. Sirolimus concentrations were measured using liquid chromatography/tandem mass spectrometry.
Results:
No LS was detected in serum or AH at any time. All other examined ocular tissues had quantifiable amounts of LS at all times. LS levels were highest in sclera and lowest in VH, suggesting LS followed the supraciliary and suprachoroidal spaces to reach the posterior segment. Vitreous peak of sirolimus levels occurred at 2 h, and the sclera adjacent to the injection peaked at both 2 and 96 h. LS levels in remaining ocular tissues peaked at 6 h and decreased with time, persisting at presumed therapeutic levels on day 22.
Conclusions:
LS can quickly diffuse into posterior intraocular tissues after SCJ injection without reaching quantifiable levels in AH or serum in DBR. Peak levels occurred in posterior intraocular tissues at 6 h and persisted in all tissues after 3 weeks. SCJ LS in DBR is safe, has a stable pharmacokinetic profile, and should be considered for further study in human trials for autoimmune ophthalmopathies.
Introduction
Vision impairment
The eye can be divided into anterior segment (AS) and posterior segment (PS). The AS includes the cornea, conjunctiva, aqueous humor (AH), iris/ciliary body (ICB), and lens, and the PS consists of the sclera, choroid, retinal pigment epithelium (RPE), neural retina, optic nerve (ON), and vitreous humor (VH).
Many of these tissues are transparent, allowing photons to be refracted on the retina where they stimulate an electrical impulse that is transmitted through the ON to the central nervous system (CNS). Transparency requires a high level of metabolic energy derived from high-volume blood flow of the ICB and choroid. As part of the CNS, the eye is an immune privileged site.
Vision impairment can result from infection, inflammation, metabolic alterations, immune dysregulation, mutations, and trauma.
The eye has characteristics that make it an excellent target for selective drug delivery, ideal for monitoring the effectiveness of new therapies. Targeted therapy of the cornea, ICB, retina, and ON to reduce toxic side effects in adjacent tissues is highly desired in ocular microenvironment therapy.1,2
Sirolimus
Sirolimus, or rapamycin, has primarily immunosuppressive functions.3–5 It works by inhibiting T cell proliferation induced by activation of the mammalian target of rapamycin pathway, blocking lymphocyte activation and interleukin-dependent plasma cell differentiation. 6 Sirolimus' physicochemical properties include almost complete insolubility in water, high lipid solubility, and instability in ionic media. These properties result in low corneal penetration, which is one of the primary obstacles in treating ocular surface disorders. 3
Sirolimus has a safe side effect profile even when combined with other immunosuppressants. 4 This has been especially helpful when combining sirolimus with synergistic medications such as cyclosporine A (CSA). 4
These potent treatment strategies are relevant in clinical practice due to the poor visual prognosis that comes with the undertreatment of autoimmune ocular disorders. 3 However, sirolimus has high variability in concentration levels, making extended-release formulations an attractive option.
Our team, as well as others, has proven that intravitreal (IVT) and subconjunctival (SCJ) administration of sirolimus pose no ocular toxicity to human and animal models even at relatively high doses.7–10 Furthermore, sirolimus can be used as a corticosteroid-sparing agent, reducing steroid-related toxic effects such as cataracts and glaucoma. 11
Liposomes
Liposomes act like cell membranes, creating a polar aqueous center and a nonpolar lipidic double layer. These particles are artificially designed to contain hydrophilic or hydrophobic drugs. Liposomal configuration not only protects drugs from degradation but also increases solubilization and bioavailability. 12
Liposomes accumulate in inflamed tissues, promoting high local drug concentrations following a small dose administration. Once in the target tissue, liposomes can act as a depot constantly releasing the drug at therapeutic, but nontoxic drug levels over time. 3 Delivered drug concentration can vary depending on whether the target tissue is infected, inflamed, or neoplastic.
The liposome preparation used in this study has been previously described.3,13,14 Sirolimus content was 1 mg/mL. Liposomes are 200 nm in diameter and were composed of phosphatidylcholine and cholesterol. Lipid dispersions were hydrated with phosphate-buffered saline and heated to 70°C, while stirring at a gravitational force of 55 g in an N2 atmosphere for 30 min. The mixture was then left at room temperature for 30 min. The dispersion was filtered through a 0.45 mm membrane and collected in amber vials. The vials were freeze dried, and the final lyophilizate was sterilized by gamma irradiation at a 10 kGy dose. Vials were kept under refrigeration until use. Before administration, the lyophilizate was reconstituted with sufficient water for injection in aseptic conditions. This method is proprietary to the authors and has a U.S.-issued patent.13,14
SCJ versus IVT drug administration
SCJ injections can be utilized when systemically and topically administered medications are not effective. They are safe, provide direct access to the sclera with its higher level of molecular permeability and reduced protease activity, and allow drugs to bypass the corneal-conjunctival epithelial barrier for entry to the cornea, to provide high concentrations of medications to the AS. SCJ medications can also diffuse through ciliary muscle fibers to reach the supraciliary and suprachoroidal (SCS) spaces of the uveoscleral pathway to the retina and choroid to deliver prolonged PS drug levels.1,2,15–20 Some systemic drug exposure occurs due to drug absorption into venous circulation. 2
The SCJ route reaches the supraciliary and SCS spaces. The supraciliary space is between the ciliary body and sclera. 20 The SCS is a potential space between the sclera and choroid that traverses the PS of the eye. This makes it an attractive site for drug delivery to the choroid, RPE, and retina due to selective high bioavailability to these areas, 18 and has a nominal thickness of 35 μm to allow movement of the choroid against the sclera during accommodation. 18
The SCS is prominent in animal eyes with passage of 3 μm microspheres noted in 1 horse study. 21 It is also part of the unconventional AH outflow pathway. Fluids can accumulate here; however, in contrast to the subretinal space, the SCS is not immune privileged since it is located outside the blood–retinal barrier. Drug delivery to the SCS has been achieved by sclerotomy, microinjection, and microcannulation with rapid levels of drugs reaching the retina, choroid, and RPE.18,19 SCS therapy is used in humans for retinal vein occlusion, diabetic macular edema, noninfectious uveitis, age-related macular degeneration (AMD), and choroidal melanoma. 19
IVT therapy is highly effective for the treatment of many retinal diseases.16,22 The vitreous acts as a drug depot, slowly releasing drugs over drug-dependent time periods. AMD, diabetic retinopathy, and retinal vein occlusion are treated with IVT anti-Vascular Endothelial Growth Factor (VEGF) drugs. IVT corticosteroids and anti-VEGF agents are used in diabetic retinopathy, retinal vein occlusion, and uveitis to help reduce leakage from blood vessels. Antibiotic, antifungal, and antiviral drugs are also used to treat endophthalmitis and retinitis. Although rare, potentially devastating complications such as endophthalmitis and retinal detachment are present. Also, treatment burden for patients from numerous injections, cost to health care systems, and impact on workflows have been substantial. 22
To better challenge the systemic concentration and potential side effects of our formulation, the SCJ route was used because it provides higher systemic absorption in small animals than the IVT route.
Immunomodulator therapy in animals with spontaneous inflammatory eye disease
Immune-mediated eye disease is very common in animals. Keratoconjunctivitis sicca (KCS) in dogs is most commonly associated with lymphocytic attack to the lacrimal glands. 23 Immune-mediated keratopathies in horses are common and increasing in frequency.24,25 Equine Recurrent Uveitis is a T cell-mediated disease of the ICB and choroid, and is the most common cause of blindness in adult horses. 26
A number of spontaneous animal models have shown striking efficacy with immunomodulator therapy. Topical CSA and tacrolimus have radically improved immune-mediated KCS prognosis in dogs. 26 Using a silicone-based implant of CSA episcleral matrix, drug delivery was dramatically effective in a canine model of immune-mediated KCS. 27 SCJ CSA implants are also commonly used to treat all forms of immune-mediated keratitis in horses.24,25 Equine recurrent uveitis is commonly treated with CSA implants in the SCS. 26
In vivo testing of liposomal sirolimus (LS) formulations in the spontaneous KCS dog model has produced promising results, showing improvement with the 1 mg/mL SCJ LS product.4,13 Dogs with KCS nonresponsive to topical CSA or tacrolimus improved lacrimal production, reduced corneal vascularization and pigmentation, and improved clarity of vision following subconjunctivally administered sirolimus at 2 different concentrations with 2 different preparation techniques. 4
The objective of this study was to determine the pharmacokinetics of the proprietary LS in ocular tissues and plasma following a single SCJ injection in Dutch belted rabbits (DBR).
Methods
Test system species, husbandry, and experimental design
Experiments were approved by the Absorptions Systems California (ASC) Institutional Animal Care and Use Committee (IACUC) and adhered to the Association for Research in Vision and Ophthalmology (ARVO) Statement for the Use of Animals in Ophthalmic and Vision Research. Thirty healthy, male Oryctolagus cuniculus DBR weighting 2.0–4.0 kilograms at study start were used. Housing was done in sanitized cages with filter tops containing absorbent, autoclaved Sani-Chip bedding within the same room. Animals were single housed to avoid injury or surgical site interference by others. Primary enclosures were as specified in the United States Department of Agriculture (USDA) Animal Welfare Act. No other species were housed in the same room. The room was well ventilated (>10 air changes per hour) with at least 60% fresh air. A 12-h light/12-h dark photoperiod was maintained, except when rooms were illuminated during the dark cycle to accommodate study procedures. Animals had ad libitum access to species-specific rabbit chow.
ASC is accredited by AAALAC International. During the study, the care and use of animals was conducted in accordance with the regulations of the USDA Animal Welfare Act (i.e., relevant sections of Section 9, Parts 1, 2, and 3, of the Code of Federal Regulations) and in compliance with ASC's Animal Welfare Assurance (D16-00645 [A4282-01]) filed with the National Institutes of Health (NIH). Treatment of the animals was in accordance with ASC SOPs and the conditions specified in the Guide for Care and Use of Laboratory Animals (NRC, 2011, National Academy Press). 28 Procedures involving the care or use of animals in this study were reviewed and approved by ASC's Institutional Animal Care and Use Committee (IACUC) prior to the initiation of such procedures (i.e., prior to the start of the study for most protocol-specified procedure).
LS was supplied as lyophilized stock. Before dosing, reconstitution was done by ASC personnel. The external vial closure was sanitized with alcohol before perforation. Vial contents were reconstituted with 1 mL of water for injection. The vial was vigorously mixed for 1 min using a vortexer set to 3,500 rpm. Once reconstituted, the test article was stored, refrigerated, and protected from light until use. Immediately before dosing, the test article was brought to room temperature. After each round of dosing, remaining test article was quickly returned to refrigeration. Reconstituted test article could be used for up to 3 months if stored, refrigerated, and protected from light. During this time, the reconstituted test article was permitted to be brought to room temperature intermittently for brief intervals.
Experimental procedures
Study design is found in (Table 1) and includes injection times and tissue collection.
Three animals were euthanized at the following time points following SCJ injection: 2, 4, 6, and 8 h postdose, day 3 (48 h postdose), day 4 (3 days postdose), day 6 (5 days postdose), day 8 (7 days postdose), day 15 (14 days postdose), and day 22 (21 days postdose).
Each animal underwent slit-lamp biomicroscopy and indirect ophthalmoscopy before the study. Findings were scored according to a modified McDonald-Shadduck Scoring System. The acceptance criteria were scores of “0” for all variables.
Animals were anesthetized with an intramuscular (IM) injection of ketamine hydrochloride (up to ∼50 mg/kg) and xylazine (up to ∼10 mg/kg) or dexmedetomidine (0.25 mg/kg). Glycopyrrolate (∼0.01 mg/kg, IM) was also administered concurrently. Atipamezole hydrochloride (up to 1 mg/kg IM) was used as a reversing agent. A thermal heating pad was used to help maintain body temperature, and vital signs were monitored throughout anesthesia and recovery. One to 2 drops of topical proparacaine hydrochloride anesthetic (0.5%) were applied to the animal's eyes. Additional topical ocular anesthesia dosing could be utilized during the procedures if needed.
LS was administered through SCJ injection into both eyes (OU) of all study animals on day 1 according to the study design in Table 1. Animals were anesthetized as described. A 5% povidone iodine solution was used to clean the eye and surrounding area, after which the eye was rinsed with balanced salt solution and the surrounding area wiped with gauze. One to 2 drops of topical proparacaine hydrochloride anesthetic (0.5%) were applied.
Using Castroviejo or Kelman-McPherson forceps, the conjunctiva was gently pulled up until the junction with the sclera was exposed. A 27–31G needle was inserted laterally into the eye at the junction and advanced ∼4–5 mm into the SCJ space tangential to the corneal limbus. One hundred microliters of LS was injected and the needle was removed. Animals were monitored during recovery. Antibiotic ophthalmic ointment was administered to each eye after injection. One perioperative injection of buprenorphine (0.02–0.05 mg/kg IM/SC) was given.
Clinical ophthalmic examinations were performed on OU of all study animals at baseline (before test/control article administration). On days 3 and 15 ± 1, the clinical ophthalmic examinations consisted of slit-lamp and indirect ophthalmoscopy only. Ocular findings were scored according to a modified McDonald-Shadduck Scoring System.
Blood was collected from all animals immediately before euthanasia. At least 1 mL of whole blood was collected into tubes containing dipotassium ethylenediamine tetraacetic acid (EDTA) as anticoagulant, inverted several times to mix, and kept on wet ice until centrifugation. Blood samples were centrifuged at 4°C, at ∼3,000g, for 5 min. The resultant plasma (at least 400 μL) was separated within ∼30 min after centrifugation. Plasma was snap frozen on dry ice and placed in a freezer set to maintain −60 to −80°C.
A total of 30 plasma samples were transferred on dry ice to ASC's analytical department in San Diego for liquid chromatography-mass spectrometry (LC-MS)/MS analysis. A total of 30 plasma samples were collected and submitted for analysis. Samples were delivered in batches following completion of collection on study times 2, 4, 6, and 8 h postdose, day 3 (48 h postdose), day 4 (3 days postdose), day 6 (5 days postdose), day 8 (7 days postdose), day 15 (14 days postdose), and day 22 (21 days postdose).
Three animals were euthanized at each time period by an intravenous injection of a commercial barbiturate-based euthanasia solution (∼150 mg/kg body weight) or KCl (up to 150 mg/kg or 2 mEq/kg to effect), while under anesthesia depending on availability. The euthanasia procedure was performed in compliance with the American Veterinary Medical Association (AVMA) Guidelines for Euthanasia of Animals: 2020 Edition. 29
Tissue collections occurred immediately following euthanasia. OU were harvested from all study animals, obtaining the following: AH, ICB, VH, retina/choroid/RPE, sclera at the dosing site, and neurosensory retina. ON samples from each eye remained separated and unpooled. The weight of each sample (except AH and VH) was recorded.
The samples were flash frozen in liquid nitrogen and placed on dry ice until storage in a freezer set to maintain a temperature of −80 ± 10°C. Samples were transferred on dry ice to ASC's analytical department in San Diego for LC-MS/MS analysis. A total of 60 AH, 60 ICB, 60 VH, 60 retina/choroid/RPE, 60 sclera, and 60 ON samples were collected and submitted for analysis. Samples were delivered in batches following completion of collection on study days 1, 3, 4, 6, 8, 15, and 22. Plasma, AH, VH, retina/choroid/RPE, sclera, ON, and ICB samples were received for LC-MS/MS analysis at ASC.
Procedures for qualification
The specificity, accuracy, and precision of the method for test article in DBR plasma, composite ocular tissue, and AH/VH were evaluated by a single-day prestudy qualification. A single standard curve and quality control (QC) sample at 3 levels with 6 replicates each were extracted and analyzed for each analyte. Calibration standards and QC samples were prepared from independently prepared or verified stock solutions.
Acceptance criteria for method qualification
One 8-point standard curve and 3 levels of QC samples with 6 replicates each were analyzed. At least 75% of standards must be accurate to within ±15%, except at the lower limit of quantification, where ±20% is acceptable. Two-third of the batch QCs must have accuracy within ±15% of nominal and at least two-third QCs must pass at each level in order for the run to be accepted. The intra-assay coefficient of variation of the replicate QC determinations must not exceed 15% and the accuracy of the mean value for each QC level must be within ±15% of the theoretical value. At least 4 of 6 QC determinations at each level must be available to calculate the statistics. Specificity was assessed by analysis of blank matrix.
Liposome sirolimus
Sterile liposomal dispersions with sizes ranging from 140 to 211 nm were successfully obtained. High entrapment efficiency of 93%–98% was achieved at sirolimus loading doses of 1 mg/mL and 0.4 mg/m.12,30 The heating method allowed an easier production of liposomes with high entrapment efficiency, to significantly shorten production time and the elimination of the use of alcohol. The poor stability of the obtained liposomes in aqueous dispersion made the inclusion of a lyophilization step necessary to the manufacturing process.
Sample analysis
LC-MS/MS methods were used to analyze plasma, AH, VH, retina/choroid/RPE, sclera, ON, and ICB samples for the presence of LS.
Results
Method qualification results
The accuracy and precision of the method met acceptance criteria in plasma, AH/VH and composite ocular tissue. All QCs were within ±15% of nominal or between 85% and 115%.
Sample analysis results
Plasma and tissue samples were extracted by protein precipitation and analyzed. Individual and mean plasma concentrations and resulting pharmacokinetic parameters for LS are shown in Tables 2–7. Samples that were below the limit of quantification (0.5 ng/mL) plasma, AH, and VH were excluded from the calculation of mean values. Samples that were below the limit of quantification (5 ng/g) for ocular tissue were excluded from the calculation of mean values. Mean concentrations versus time data are plotted in (Figs. 1–5).
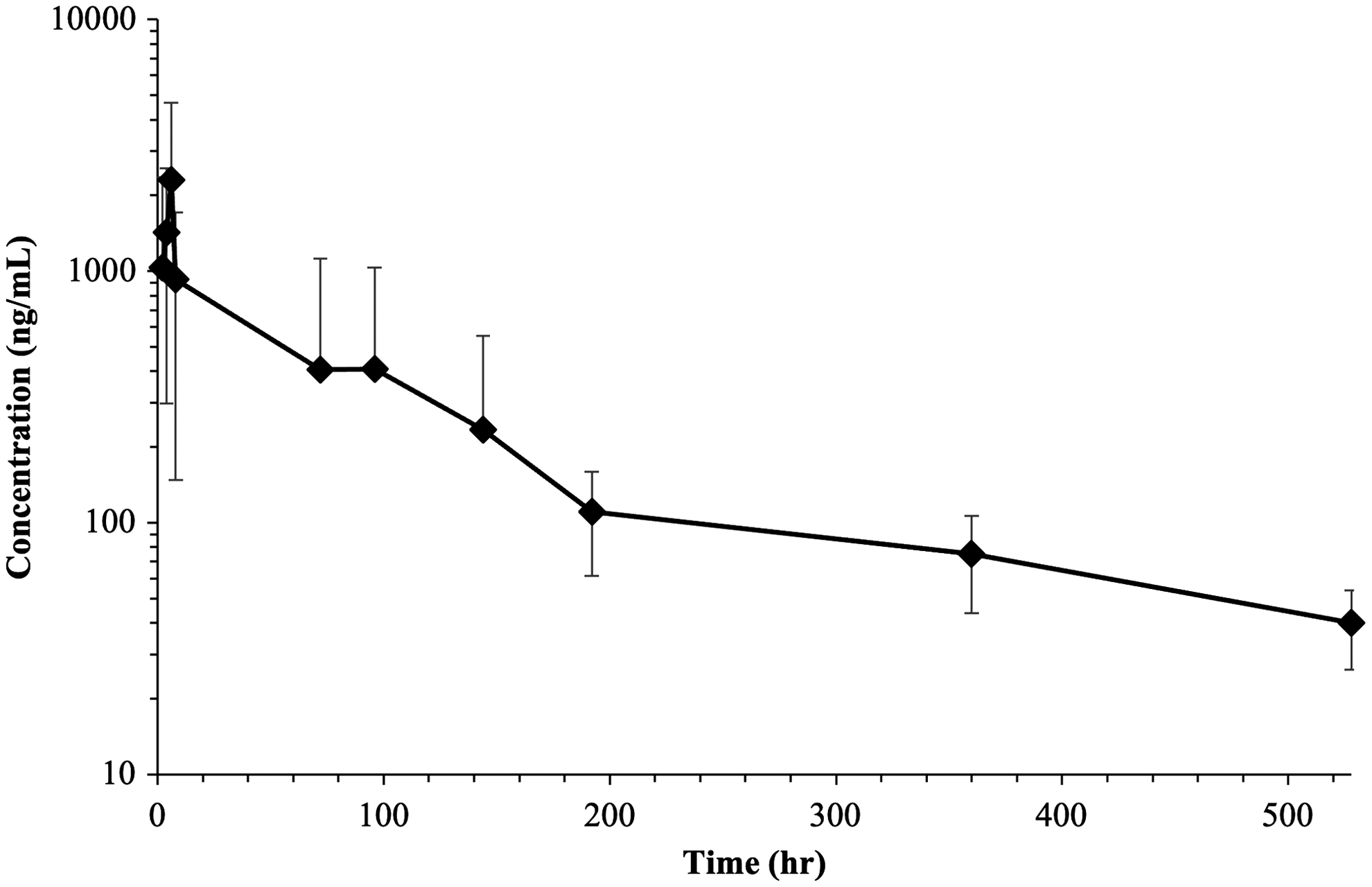
Mean retina/choroid/RPE (combined) concentration (ng/mL) of sirolimus (rapamycin) versus time (h) after SCJ injection (100 μg/eye) in Dutch belted rabbits. RPE, retinal pigment epithelium; SCJ, subconjunctival.
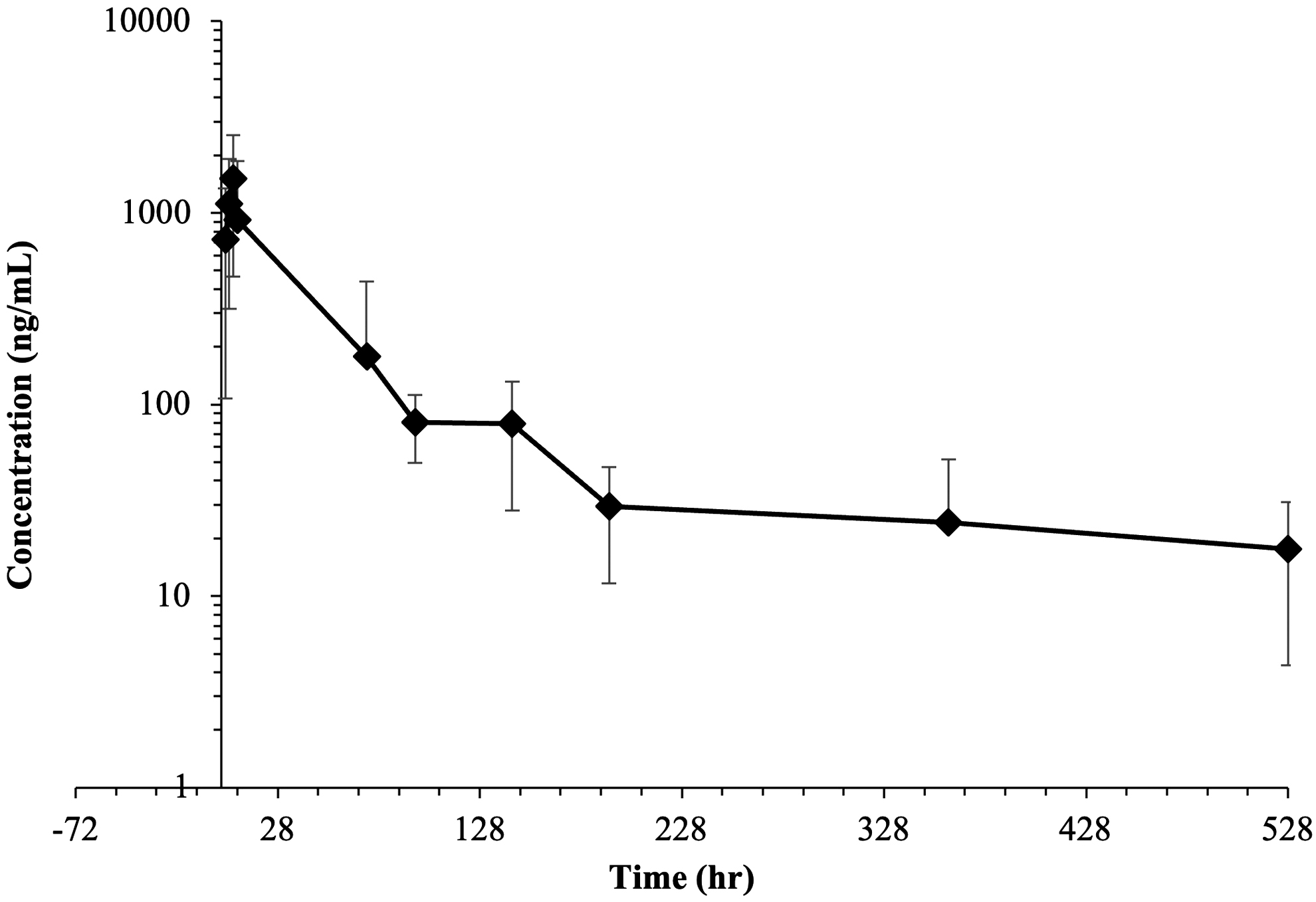
Mean iris-ciliary body concentration (ng/mL) of sirolimus (rapamycin) versus time (h) after SCJ injection (100 μg/eye) in Dutch belted rabbits.
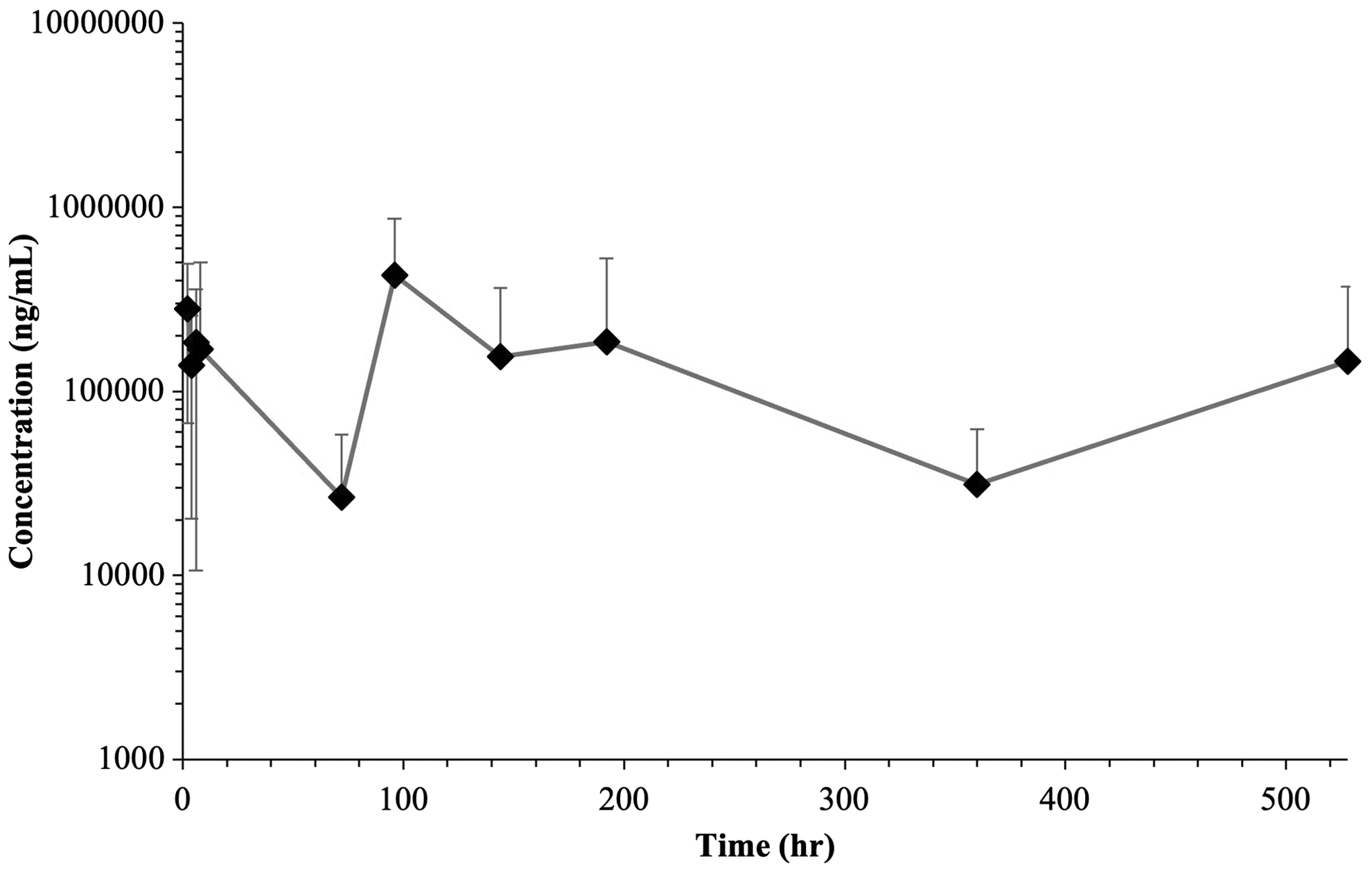
Mean sclera concentration (ng/mL) of sirolimus (rapamycin) versus time (h) after SCJ injection (100 μg/eye) in Dutch belted rabbits.
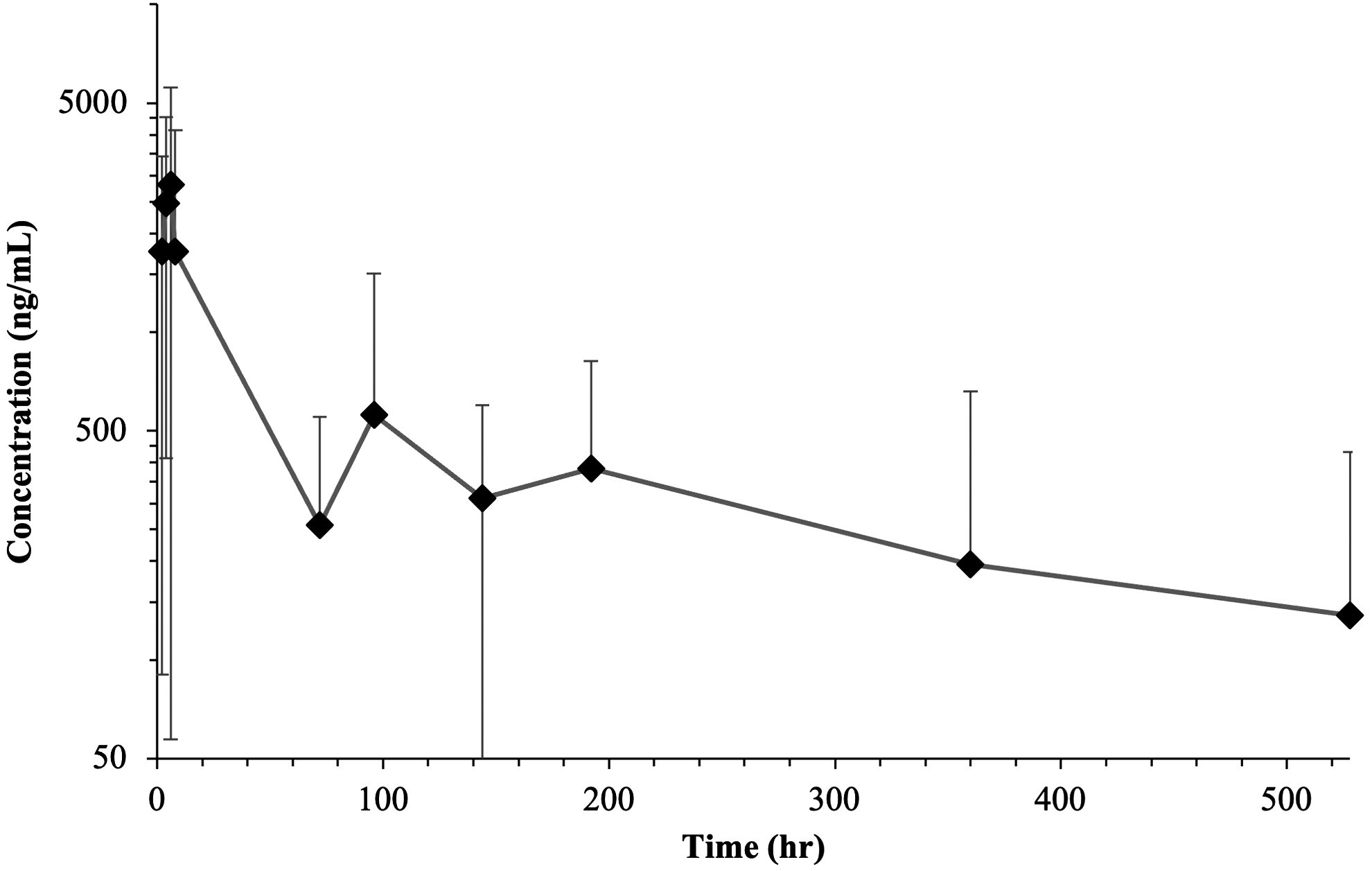
Mean ON concentration (ng/mL) of sirolimus (rapamycin) versus time (h) after SCJ injection (100 μg/eye) in Dutch belted rabbits. ON, optic nerve.
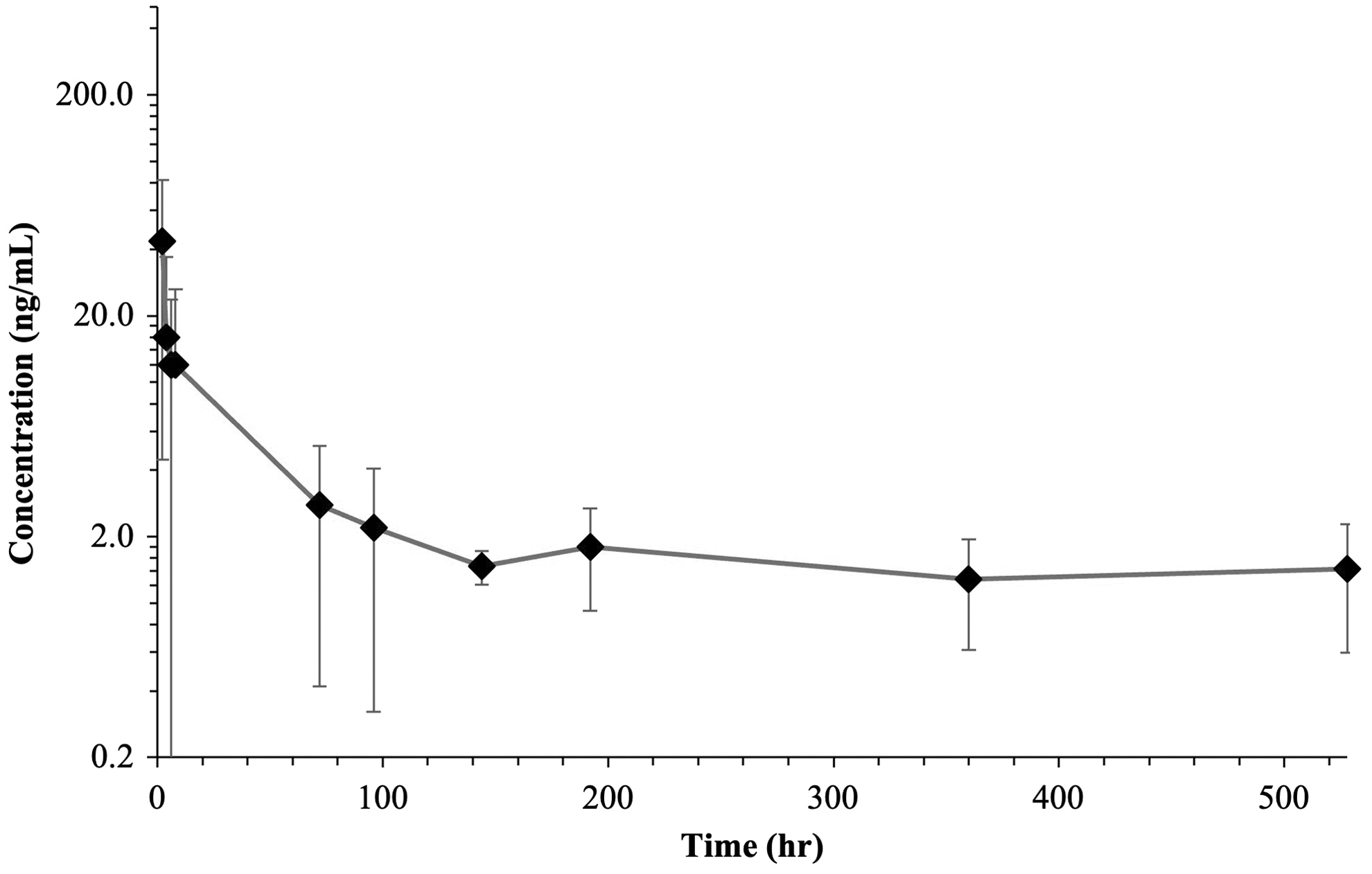
Mean VH concentration (ng/mL) of sirolimus (rapamycin) versus time (h) after SCJ injection (100 μg/eye) in Dutch belted rabbits. VH, vitreous humor.
Experimental Study Design with Times of Injections and Times of Tissue Collection
Baseline clinical ophthalmic examinations (slit-lamp, biomicroscopy and indirect ophthalmoscopy) were conducted by G.G.
The day 3 and 15 ophthalmic examinations (slit lamp and indirect only) were conducted by a Board Certified Veterinary Ophthalmologist.
AH, aqueous humor; ICB, iris/ciliary body; ON, optic nerve; OU, both eyes; RPE, retinal pigment epithelium; VH, vitreous humor.
Summary of Mean Pharmacokinetic Parameters for Sirolimus (Rapamycin) after Subconjunctival Injection (100 ug/eye) in Dutch Belted Rabbits
Not determined because the line defining the terminal elimination phase had an r2 of <0.85.
Not determined because the AUC∞ was a greater than 25% extrapolation above the AUClast.
AUC, area under the time-concentration curve; Cmax, maximum plasma concentration; MRT, mean residence time; ND, not determined; t1/2, plasma half-life; tmax, time to reach maximum plasma concentration.
Pharmacokinetic Parameters and Mean Retina/Choroid/RPE (combined) Concentrations for Sirolimus (Rapamycin) after Subconjunctival Injection (100 ug/eye) in Dutch Belted Rabbits
NA, not applicable; SD, standard deviation.
Pharmacokinetic Parameters and Mean Iris-Ciliary Body Concentrations for Sirolimus (Rapamycin) after Subconjunctival Injection (100 ug/eye) in Dutch Belted Rabbits
Pharmacokinetic Parameters and Mean Sclera Concentrations for Sirolimus (Rapamycin) after Subconjunctival Injection (100 ug/eye) in Dutch Belted Rabbits
Pharmacokinetic Parameters and Mean Optic Nerve Concentrations for Sirolimus (Rapamycin) after Subconjunctival Injection (100 ug/eye) in Dutch Belted Rabbits
Pharmacokinetic Parameters and Mean Vitreous Humor Concentrations for Sirolimus (Rapamycin) after Subconjunctival Injection (100 ug/eye) in Dutch Belted Rabbits
Not determined because the line defining the terminal elimination phase had an r2 of <0.85.
Not determined because the AUC∞ was a greater than 25% extrapolation above the AUClast.
Data analysis
Pharmacokinetic parameters were calculated from the time course of the plasma concentration with the Phoenix WinNonlin (v8.0) software using a noncompartmental analysis model. The maximum plasma concentration (Cmax) and the time to reach maximum plasma concentration (tmax) after dosing were calculated from the data. The area under the time-concentration curve (AUC) was measured using the linear trapezoidal rule with calculation to the last quantifiable data point (AUC0-last), and with extrapolation to infinity (AUC
Results of bioanalysis
All samples were received in good condition, stored at −80°C until analysis. The analytical methods for detection of LS in rabbit plasma, AH, VH, retina/choroid/RPE, sclera, and ICB tissues were developed. These methods were used to analyze plasma, AH, VH, retina/choroid/RPE, sclera, ON, and ICB samples. The accuracy and precision of the method met the acceptance criteria in plasma, AH/VH, and composite ocular tissue. All QCs were within ±15% of nominal or between 85% and 115%.
Bioanalysis of plasma and AH had no quantifiable amounts of LS observed at any time point. VH, retina/choroid/RPE, sclera, ON, and ICB had quantifiable amounts of LS at all time points (Table 2). Liposome with sirolimus levels was highest in sclera, then ON, then retina/choroid/RPE, ICB, and then VH. Vitreous peak of sirolimus levels occurred at the 2-h time point, and sirolimus levels in the sclera adjacent to the SCJ injection peaked at both 2 and 96 h with the highest level being at the 96-h time point following SCJ injection. The remainder of the ocular tissue, including retina/choroid/RPE, ON, and ICB, had the highest levels of sirolimus at the 6 h-time point, decreased with time, and was still elevated to presumed therapeutic levels at the 528-h (22 days) test time point following SCJ injection.
Results of clinical ophthalmic examinations
Slit-lamp biomicroscopy found no abnormality at baseline (all scores were zero). By day 3, 12 of the 15 animals showed mild bilateral conjunctival swelling (maximum score 1/4) and mild bilateral congestion (maximum score 1/4). One rabbit showed a focal area of faint opacity in the corneal epithelium localized to ∼3 mm area ventronasal quadrant peripherally, concomitant with some loss of cornea transparency (cornea score = 1) to less than 25% of the cornea (cornea surface area involved = 1) OS. In another rabbit, there was a mild degree of corneal opacification of the right eye, which resulted in mild loss of corneal transparency (OD cornea score=1), corresponding to less than 25% of the corneal surface (cornea surface area involved = 1). One rabbit showed a punctate axial anterior cortical lens opacity (lens score=1) of the left eye (OS).
Another rabbit showed a pinpoint anterior cortical axial lens opacity (lens score = 1) OS. In addition, 1 animal had bilateral punctate posterior cortical/polar opacities (lens score = 3) of both eyes (OU). By day 15, 4 of the 6 remaining animals showed bilateral mild conjunctival swelling (swelling above normal without eversion of the eyelids, maximum score 1/4), and mild congestion (maximum score 1/4). Indirect ophthalmoscopy throughout the course of the study found no abnormality of the fundus such that all scores were zero.
Discussion
LS is safe in a dose range from 40 to 440 μg/eye after SCJ or IVT injection in animal models. 3 In the toxicity study, no deleterious effect attributable to LS was found after SCJ and IVT rabbit trials. Micronucleus count was normal, and the overall irritation score showed no significant difference compared with the negative control. No sirolimus was found in blood, and no genotoxicity was noted. Histological, metabolic, biochemical, and hematological evaluations demonstrated no sirolimus-related harm after SCJ injection. In addition, conservation of retinal function after IVT injection was demonstrated. 3
This study sought to determine the pharmacokinetics of LS in selected ocular tissues and plasma following a single SCJ in DBR. Animals were assessed for overall health throughout this investigation. No serious abnormality due to this LS product was noted in bodyweight, cage-side observations, or detailed clinical observations. Slit-lamp evaluation found that 12 out of 15 animals showed very mild bilateral conjunctival swelling from day 3 to the end of the in-life phase (day 15).
In addition, 1 animal showed mild axial corneal haze on day 3, and another animal showed bilateral punctate posterior cortical/polar lens opacities by day 15. We found very mild conjunctival chemosis in 12/15 rabbit OU on day 3 following SCJ injection, which was noted in 4/6 rabbits on day 15 postinjection. A faint focal anterior subepithelial haze was present on day 3 in 1 eye of 2 rabbits. Punctate cortical lens opacities were present in 1 eye each of 2 rabbits, and posterior cortical lens opacities present in both eyes of a third rabbit. Indirect ophthalmoscopy evaluation found no abnormality in the initial toxicity study and this pharmacokinetic study. 3
Therapeutic plasma levels of sirolimus are reported to be 4–12 ng/mL in pediatric patients, 31 and 5–15 ng/mL in adult kidney transplant patients. 32 In this study, bioanalysis of plasma and AH found no quantifiable amount of LS observed at any time point. VH, retina/choroid/RPE, sclera, ON, and ICB had quantifiable amounts of LS at all time points. Peak vitreous LS levels occurred at 2 h, and the scleral peak was at both 2 and 96 h, with the highest level occurring at 96 h.
The SCJ scleral tissue, as expected, had the highest level of LS, which suggests that liposomes followed the SCS spaces from the tissues beneath the conjunctiva to reach the tissues of the PS.18,19 The remaining ocular tissues had the highest levels of sirolimus at the 6-h time point, which slowly decreased with time, and were still elevated to presumed therapeutic levels at the 528-h (22 days) time point following SCJ injection.
Levels of LS in tissues and VH in this study declined with time, but remained at levels greater than presumed therapeutic target levels for sirolimus at 22 days following SCJ injection with LS. SCJ LS is safe and effective in animals with spontaneous immune-mediated KCS and immune-mediated nonulcerative keratitis, and needs to be further evaluated for immune mediated PS disease in animals. It may also be useful for managing human patients with AS and PS eye diseases. In addition to these pathologies, future clinical applications for LS could include, but not be restricted to, cancer therapy, 33 complex vascular anomalies in children, 34 and antiatherosclerotic therapy. 35 LS should be included in further characterization studies to determine adequate routes of administration for these pathologies, as well as real-world scenario studies where long-term liposome stability is challenged to determine optimal sirolimus dosing.
Conclusions
Plasma and AH had no quantifiable amounts of LS at any time point. VH, retina/choroid/RPE tissue, sclera, ON, and ICB had quantifiable amounts of LS at all time points, indicating that SCJ LS is able to diffuse to the PS. The highest levels of LS occurred in PS tissues at the 6-h time point following SCJ injection. LS has pharmacokinetic and safety profiles that suggest it is favorable for treating inflammatory conditions of the AS and PS of the eye. Furthermore, it shows great potential to be proven in human clinical trials.
Footnotes
Acknowledgments
The authors wish to give a special recognition to Dr. Maria J. Bernad-Bernad, whose effort has been paramount in the design and development of the Sirolimus liposome formulation. We also want to thank all the team at Absorptions Systems in San Diego for their extraordinary work and dedication.
Authors' Contributions
D.B.: conceptualization, original draft preparation, and fund acquisition. M.A.L.-A.: investigation and methodology. R.G.-S.: original draft preparation, review, and editing. E.X.: conceptualization and methodology formal analysis. G.G.: conceptualization, methodology, and project administration. L.L.M.: conceptualization and methodology formal analysis. J.F.-F.: investigation and methodology. D.G.: funding acquisition and review. G.A.G.-S.: supervision, project administration, and funding acquisition.
Author Disclosure Statement
G.A.G.-S. owns the LS patent used in this study. The remaining authors have nothing to disclose.
Funding Information
No funding was received for this article.