
Abstract
Purpose:
To compare the effectiveness of the topical use of cyclosporin A (CsA) 0.1%, diquafosol (DQS) tetrasodium 3% ophthalmic solution, and their combination in treating dry eye disease in a general health care setting.
Methods:
This prospective, nonrandomized, observational study analyzed 279 patients. Patients instilled topical CsA 0.1% (Ikervis®; Santen Pharmaceutical Co., Ltd., Japan) once daily and/or DQS tetrasodium 3% (Diquas-S®; Santen) six times a day for 12 weeks. Objective signs [tear break-up time (TBUT), National Eye Institute (NEI) corneal and conjunctival staining scores] and symptoms [Symptom Assessment in Dry Eye (SANDE) and Dry Eye-related Quality-of-Life Score (DEQS) questionnaires] were evaluated at baseline, week 4, and week 12.
Results:
Patients (n = 279) were mainly female (85.0%) with a mean (SD) age of 50.1 (14.8) years, and received CsA (n = 93), DQS (n = 99), or CsA/DQS (n = 87). Both monotherapies and CsA/DQS combination therapy significantly improved TBUT, NEI corneal and conjunctival staining scores, and SANDE and DEQS scores from baseline to week 12 (all P < 0.0001). The mean change in TBUT between baseline and week 12 was significantly higher in CsA/DQS combination therapy (2.13 ± 2.41 s) than in CsA monotherapy (1.07 ± 1.71 s; P = 0.0011).
Conclusions:
Monotherapy with CsA or DQS and CsA/DQS combination therapy all significantly improved the objective signs and symptoms of dry eyes during 12 weeks of treatment. CsA/DQS combination therapy provides an additional benefit in terms of TBUT compared with CsA alone; however, a randomized controlled trial still needs to be performed to confirm this result.
Introduction
Dry eye disease (DED) is a multifactorial disease of the tear film and ocular surface that can cause ocular discomfort and blurred vision.1–3 DED encompasses a spectrum of conditions ranging from aqueous-deficient dry eye (ADDE) to the more common evaporative dry eye (EDE). ADDE is principally caused by lacrimal gland dysfunction and includes DED caused by the autoimmune disorder Sjögren's syndrome (SS) and non-SS dry eye. EDE is caused by both eyelid-related abnormalities [e.g., Meibomian gland dysfunction (MGD)] and ocular surface-related changes (e.g., mucin deficiency or wearing contact lenses).2,4
DED has a measurable effect on several aspects of patients' quality of life (QoL), including pain, vitality, the ability to perform certain activities requiring sustained visual attention (e.g., reading and driving), and productivity in the workplace. These QoL effects of DED carry substantial economic effects.5,6
The mainstay of dry eye therapy is artificial tears, which mimic tears and improve the symptoms and signs of all DED subtypes due to their lubricant properties. However, artificial tears are not effective in all patients, especially those with moderate-to-severe disease; consequently, those patients need escalated therapy.3,7,8 Although topical corticosteroids are known to be effective for the symptoms and signs of dry eye, they are not suitable for long-term treatment because of side effects such as increased intraocular pressure and cataracts. 9 On the other hand, the use of immunosuppressive agents to control the inflammatory response is effective for controlling the symptoms and signs of DED. In particular, cyclosporin A (CsA) is known to be safe and effective for the long-term treatment of DED. 10 Recently, CsA 0.1% eye drops (Ikervis®; Santen Pharmaceutical Co., Ltd., Japan) have been marketed and shown excellent effects in treating DED.11–13
In addition to CsA, diquafosol (DQS) tetrasodium 3% ophthalmic solution (Diquas-S®; Santen) is a P2Y2 receptor agonist that has been approved for the treatment of DED in South Korea and Japan. After binding to P2Y2 receptors on the ocular surface, DQS stimulates tear fluid and mucin secretion by increasing the release of intracellular calcium ions.14,15 The safety and efficacy of DQS, in terms of both subjective symptoms and objective signs, have been demonstrated in randomized controlled trials16–21 and observational studies.22–24
Both CsA and DQS have been reported to be effective treatments for DED. However, no studies have compared the therapeutic effects of CsA and DQS monotherapies with those of the two drugs used together. The purpose of this study was to compare the effectiveness of CsA and DQS monotherapies with that of CsA/DQS combination therapy in a general health care setting.
Methods
This multicenter, prospective, nonrandomized, 12-week observational study in a general health care setting was conducted between August 2019 and June 2020 at 16 institutions in South Korea. The study was conducted in accordance with the ethical principles stated in the Declaration of Helsinki and Good Clinical Practice Guidelines. Before study initiation, the study was approved by the Institutional Review Board of each participating institution.
Study population
Subjects who met the inclusion and exclusion criteria were enrolled in each treatment arm based on the prescribed treatment according to typical clinical practice. All subjects provided informed consent before participation in the study. Subjects aged 19 to <80 years with DED [grade of corneal fluorescein staining ≤6 points according to National Eye Institute/Industry (NEI) scale and tear break-up time (TBUT) of ≤10 s) were included. Eye selection criteria were as follows: (1) the eye with the higher grade of corneal fluorescein staining according to the NEI scale was selected, or (2) if both eyes had the same corneal staining grade, the right eye was selected.
The main exclusion criteria were subjects who: used CsA ophthalmic solution, steroid ophthalmic solution, or antibiotics (ophthalmic solution) within 4 weeks or DQS tetrasodium ophthalmic solution within 2 weeks from the date of consent; were planning eye surgery (including LASIK/LASEK) during the study period; were pregnant, lactating, or planning to become pregnant; had a known hypersensitivity to the study drug(s) or were allergic to fluorescein or anesthetic eye drops; had worn contact lenses within 1 month of the examination time; had a history of ophthalmic surgery or trauma within the previous 6 months; currently used systemic medication that can affect the ocular surface, meibomian glands, and tear film layer, such as tetracycline derivatives, antihistamines, or isotretinoin;7,25–27 had been diagnosed with SS, severe obstructive MGD, or hypersecretory MGD; or were deemed otherwise ineligible by the investigator.
Study protocol
All participants completed medical history questionnaires. Subjective symptom scores and objective signs were evaluated at baseline (Visit 1), week 4 (Visit 2), and week 12 (Visit 3). Clinical measurements to observe the objective signs of dry eye were performed in the following order by a single principal investigator (PI) or a PI with a subinvestigator for each institution: (1) fluorescein TBUT; (2) ocular surface staining grade; (3) tear meniscus and lid margin investigation; and (4) tear volume measurement. Patients were treated with CsA 0.1% ophthalmic solution (Group 1: CsA group), DQS tetrasodium 3% ophthalmic solution (Group 2: DQS group), or combination therapy with both drugs (Group 3: CsA/DQS group) for 12 weeks. There was no intervention for assigning subjects to specific treatment groups; treatment was assigned at the discretion of the individual investigators in a general health care setting, with subjects purchasing the study drugs from an out-of-hospital pharmacy according to the investigator's prescription.
The level of dry eye was determined from I to IV, as defined by the Korean Corneal Disease Study Group guidelines.3,24 According to the main causative mechanism, dry eye was divided into four subtypes: short TBUT-type dry eye, ADDE, EDE, and abnormal tear distribution.28,29 ADDE was diagnosed when the tear volume measured with a strip meniscometry tube was 5 mm or less and the tear meniscus height was low and accompanied by conditions that could affect lacrimal gland function, such as non-SS dry eye.2,28–30 EDE was diagnosed when the causative mechanism of dry eye was an evaporative component such as visual display terminal work or MGD.2,31 Abnormal tear distribution was diagnosed when impaired tear distribution was observed across the ocular surface due to abnormalities such as conjunctivochalasis, lid and lash malposition, or elevated ocular surface lesions. 32 Short TBUT-type dry eye was defined when TBUT was 5 s or less and the case did not fall into any of the three other subtypes.28,33
Subjective and objective examinations
All subjects completed the two-part Symptom Assessment in Dry Eye (SANDE) questionnaire,34,35 which assesses the frequency and severity of dry eye symptoms, and the 15-item Dry Eye-related Quality-of-life Score (DEQS) questionnaire. 36 After staining with fluorescein sodium-impregnated paper strips (Haag-Sterit, Bern, Switzerland), TBUT was measured three times, and the mean value was recorded to two decimal places. 37 Corneal and conjunctival staining with fluorescein were graded according to the NEI grading scale, which divides the cornea into five sections and divides the conjunctiva into six sections, and grades each section from 0 (absent) to 3 (severe) for a total score of 0–15 for the corneal staining and 0–18 for conjunctival staining. 38 Whole corneal and conjunctival staining was graded using the Oxford grading scheme according to standard photos (0–5). 39 To measure the tear volume, a strip meniscometry tube was applied to the lower tear meniscus for 5 s, and the stained length was measured. 30
Patient-reported outcomes were investigated at week 12 (Visit 3) to identify the most uncomfortable aspects of dry eye and evaluate the current dry eye condition, compared with before treatment. Patients' compliance of each eye drop instillation was evaluated by daily self-recording at each visit. Topical CsA 0.1% compliance was measured as a percentage of CsA instilled during the study period and DQS tetrasodium 3% compliance was measured as a percentage of the number of days, in which DQS was instilled four or more times a day during the study period.
Statistical analyses
This study hypothesized that there would be differences in treatment response among the CsA, DQS, and CsA/DQS groups and a priori power analysis was conducted to estimate the sample size needed for the testing hypotheses. Multivariable logistic regression analyses with treatment response as a variable required 240 dry eye subjects, assuming an expected treatment response rate of 70%, an odds ratio of 1.5, a significance level of 5%, a 20% attrition rate, and an R2 (proportion of variance explained by covariates) of 0.2. Thus, the number of subjects required for this study was set to 300 assuming a dropout rate of 20%.
Quantitative variables were summarized using the mean, standard deviation (SD), number (n), and percentage (%). Chi-square or Fisher's exact testing was used to compare categorical variables among groups. Intra- and intergroup efficacy changes between visits were analyzed using the Wilcoxon signed-rank test. Analysis of variance, calculated using a general linear model, was used to determine statistical significance among groups, and Scheffe's method was used for multiple comparisons between groups. The Student's t-test was used to compare the topical CsA 0.1% compliance and DQS 3% compliance between groups. Analysis of covariance (ANCOVA) with adjustment of baseline characteristics was conducted for intergroup comparison analysis of NEI conjunctival staining scores. A P < 0.05 signified statistical significance. All statistical analyses were conducted using SAS v9.4 (SAS Institute Inc., Cary, NC, USA).
Results
A total of 279 eyes from 279 dry eye patients (of 304 enrolled) were analyzed in this study [93, 99, and 87 subjects in Groups 1 (CsA), 2 (DQS), and 3 (CsA/DQS), respectively]; 25 subjects were not included in efficacy analysis due to nonadministration of the investigational drugs. Table 1 shows the baseline characteristics of the study population and their eyes. Most of the subjects were female (85.0%), and they had a mean (SD) age of 50.1 (14.8) years. Most subjects had Level I (mild; 47.0%) or II (moderate; 52.7%) disease, and a significantly higher proportion of Level II disease was found in the CsA (63.4%) and CsA/DQS groups (65.5%) than in the DQS group (31.3%). The most common dry eye subtype was the short TBUT-type (47.3%), followed by ADDE (34.4%) and EDE (17.2%). A higher proportion of ADDE was found in the CsA group (50.5%), and a higher proportion of short TBUT-type dry eye was found in the DQS (54.6%) and CsA/DQS groups (55.2%).
Baseline Characteristics of the Study Population (n = 279)
Data are mean (SD) except for sex, dry eye severity (level), dry eye subtype, and Oxford grading scheme, which are n (%).
Analysis of variance calculated with a general linear model was used to compare continuous variables among groups.
Chi-square or Fisher's exact testing was used to compare categorical variables among groups.
Significant difference between Groups 1 and 2 and between Groups 2 and 3.
Significant difference between Groups 1 and 3 and between Groups 2 and 3.
CsA, Cyclosporin A; DEQS, Dry Eye-related Quality-of-Life Score; DQS, diquafosol; NEI, National Eye Institute; SANDE, Symptom Assessment in Dry Eye questionnaire; SD, standard deviation; TBUT, tear break-up time.
The distribution of subtypes differed significantly between treatment groups (P = 0.0009). The mean SANDE scores, DEQS impact on daily life, DEQS bothersome ocular symptoms, DEQS summary scores, NEI corneal and conjunctival staining, and Oxford grading scheme at baseline were all significantly higher in the CsA/DQS group than in the CsA and DQS groups (P = 0.0004, P = 0.0004, P = 0.0022, P = 0.0004, P = 0.0160, P < 0.0001, and P = 0.0002, respectively).
The baseline SANDE symptom frequency, severity, and combined evaluation scores were significantly higher in the CsA/DQS group than in the CsA and DQS groups. Despite those differences, all three scores (symptom frequency, severity, and combined evaluation) improved significantly from baseline to week 4 and 12 in all three groups (P < 0.0001 for all; Fig. 1). Similarly, the baseline DEQS domain scores (impact on daily life, bothersome ocular symptoms, and questionnaire summary) were all significantly higher in the CsA/DQS group than in the CsA and DQS groups, and all three parameters improved significantly from baseline to week 4 and 12 in all treatment groups (P < 0.0001 for all; Fig. 2).
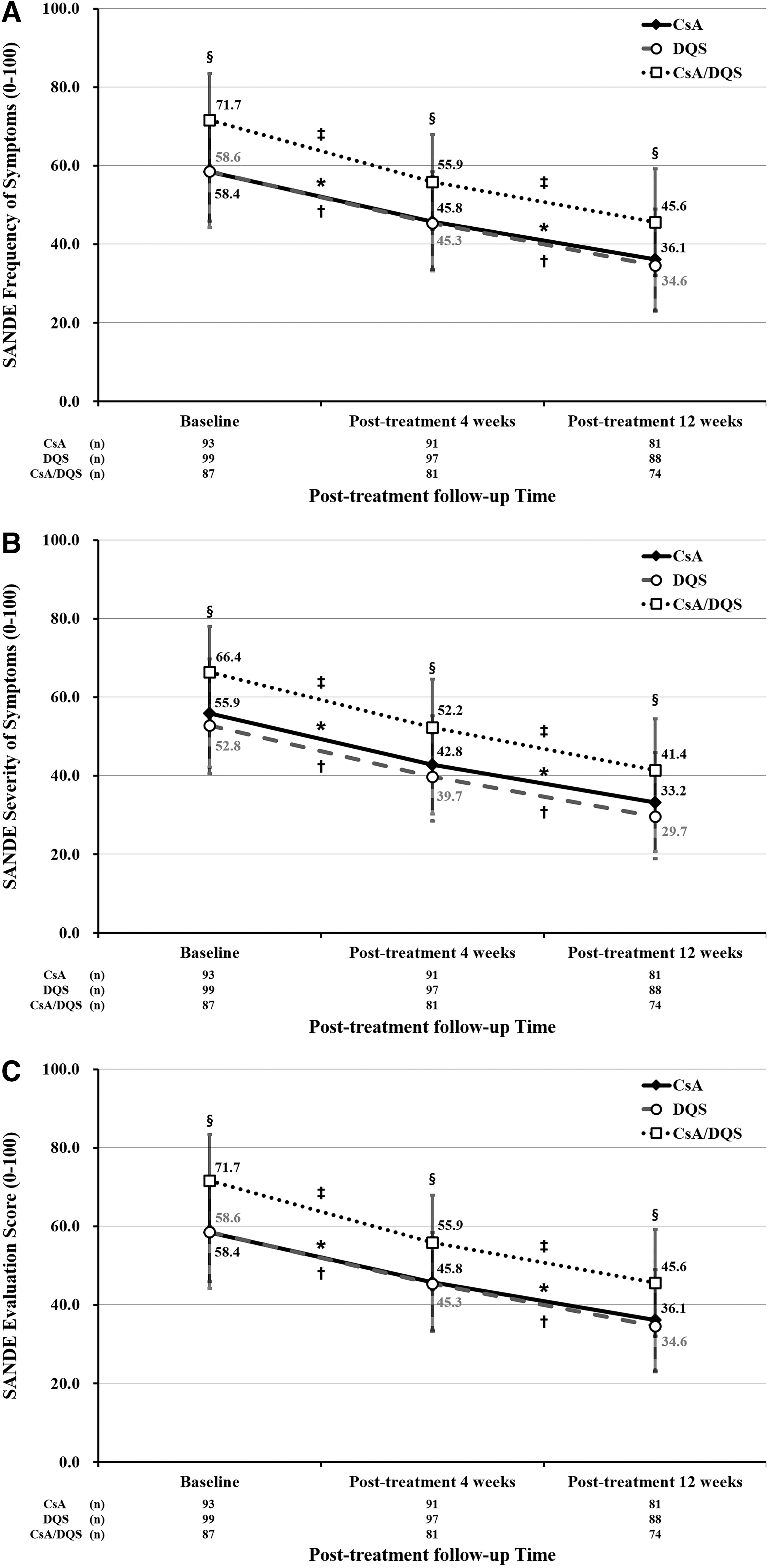
Comparison of SANDE symptom frequency

Comparison of DEQS domains for the impact on daily life
In each treatment group, TBUT improved significantly from baseline (Visit 1) to week 4 (Visit 2) and week 12 (Visit 3; P < 0.0001 for all). The mean change in TBUT between baseline and week 12 was significantly higher in the CsA/DQS group (2.13 ± 2.41 s) than in the CsA group (1.07 ± 1.71 s) (P = 0.0011; Table 2).
Comparison of Tear Break-Up Time at Visit 1 (Baseline), Visit 2 (Week 4), and Visit 3 (Week 12)
Data are mean (SD) in seconds.
Wilcoxon signed-rank test was used to compare efficacy changes between visits within each group.
Analysis of variance calculated with a general linear model was used to determine statistical significance among groups, and Scheffe's method was used for multiple comparison between groups.
Significant P values <0.05 are shown for pairwise comparisons, as indicated.
P value <0.0001.
In each treatment group, the NEI cornea and conjunctival staining scores improved significantly from baseline to week 4 and 12 (P < 0.0001 for all). The change in NEI conjunctival staining (but not corneal staining) from baseline to week 12 was higher in the CsA/DQS group (2.22 ± 3.37) than in the CsA (0.88 ± 2.00) and DQS (0.98 ± 1.55) groups (Table 3). However, there was no significant difference in the NEI conjunctival staining score change from baseline to week 12 among groups on ANCOVA with adjustment of baseline characteristics.
National Eye Institute Corneal and Conjunctival Staining Scores at Visit 1 (Baseline), Visit 2 (Week 4), and Visit 3 (Week 12)
Data are the mean (SD).
Wilcoxon signed-rank test was used to compare efficacy changes between visits within each group.
Analysis of variance calculated with a general linear model was used to determine statistical significance among groups.
P < 0.0001.
NEI staining scores are summarized by dry eye severity (Level I or II) in Table 4. In patients with Level I (mild) disease, the change in the NEI corneal staining score from baseline to 12 weeks was higher in the CsA/DQS group (1.66 ± 1.78) than in the CsA (0.71 ± 0.87) and DQS groups (0.99 ± 0.98). In patients with Level II (moderate) disease, the CsA/DQS group (2.91 ± 3.93) had a numerically higher mean change in the NEI conjunctival staining score from baseline to 12 weeks than the CsA group.
National Eye Institute Corneal and Conjunctival Staining Scores in Level I and II Dry Eye Disease at Visit 1 (Baseline), Visit 2 (Week 4), and Visit 3 (Week 12)
Data are the mean (SD).
Wilcoxon signed-rank test was used to compare efficacy changes between visits within each group.
Analysis of variance calculated with a general linear model was used to determine statistical significance among groups.
Subgroup analysis was used to assess changes in TBUT and combined NEI corneoconjunctival staining scores from baseline in subjects with short TBUT-type dry eye and ADDE. In patients with short TBUT-type dry eye, TBUT improved significantly from baseline to weeks 4 and 12 in all three groups (P < 0.0001). In addition, combined NEI corneoconjunctival staining scores improved significantly from baseline to weeks 4 and 12 in the DQS and CsA/DQS groups (P < 0.0001) and at week 12 in the CsA group (P < 0.05). Although there was no difference in TBUT among three groups at baseline, TBUT in the CsA/DQS group (6.11 ± 2.50 s) became significantly longer than that in the CsA group (4.88 ± 1.58 s) at week 12 (P = 0.0294; Table 5).
Comparison of Tear Break-Up Time and Combined National Eye Institute Corneal and Conjunctival Staining Scores at Visit 1 (Baseline), Visit 2 (Week 4), and Visit 3 (Week 12) in the Short Tear Break-Up Time-Type Dry Eye Disease Subgroup
Bold values indicate statistical significance at the level of P < 0.05 in follow-up visits, although there was no difference at baseline.
Data are the mean (SD).
Wilcoxon signed-rank test was used to compare efficacy changes between visits within each group.
Analysis of variance calculated with a general linear model was used to determine statistical significance among groups.
P < 0.0001.
P = 0.0564.
P < 0.05.
Among ADDE patients, TBUT improved significantly from baseline to weeks 4 and 12 in all three groups (P < 0.05). Combined NEI corneoconjunctival staining scores improved significantly from baseline to at weeks 4 and 12 in the CsA and CsA/DQS groups (P < 0.05) and at week 12 in the DQS group (P < 0.05). TBUT change from baseline to at week 12 in the CsA/DQS group (2.38 ± 2.54 sec) was greater than in the CsA (0.87 ± 1.74) and DQS (1.67 ± 1.29) monotherapy groups (Table 6; P = 0.0062).
Comparison of Tear Break-Up Time and Combined National Eye Institute Corneal and Conjunctival Staining Scores at Visit 1 (Baseline), Visit 2 (Week 4), and Visit 3 (Week 12) in the Aqueous-Deficient Dry Eye Disease Subgroup
Bold value indicates statistical significance at the level of P < 0.05 in follow-up visits, although there was no difference at baseline.
Data are the mean (SD).
Wilcoxon signed-rank test was used to compare efficacy changes between visits within each group.
Analysis of variance calculated with a general linear model was used to determine statistical significance among groups.
P < 0.05.
P < 0.0001.
P = 0.0607.
Changes among groups in the Oxford grading corneal and conjunctival staining score from baseline to weeks 4 and 12 are shown in Figure 3. At baseline, the Oxford grading scheme differed significantly among groups (P = 0.0002). No significant differences in the Oxford grading scheme were found among groups at week 4 but, at week 12, the ratio of grade 1 was higher in the DQS group than in the CsA group.
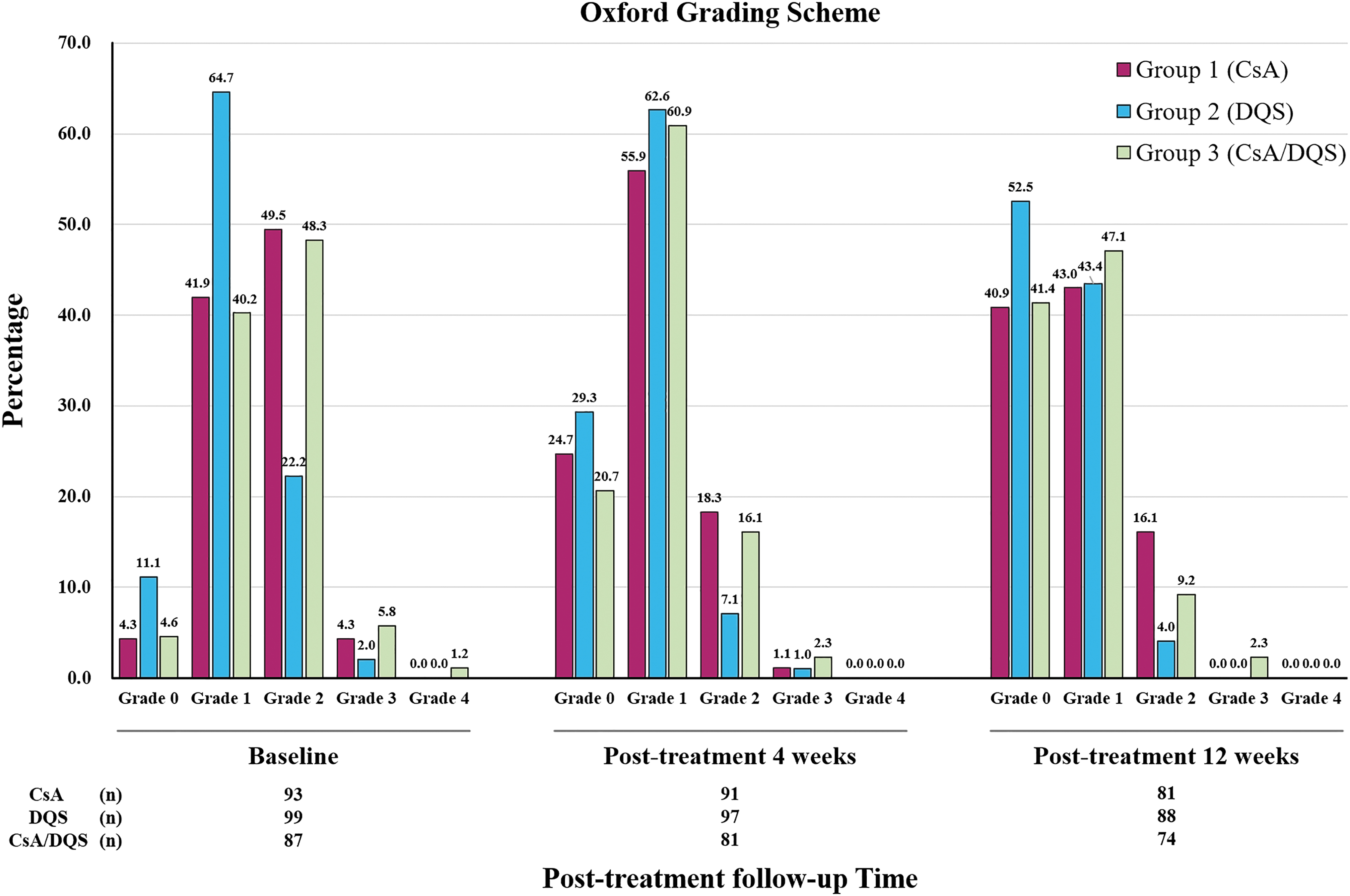
Oxford grading scheme for corneal and conjunctival staining at Visit 1 (baseline), Visit 2 (week 4), and Visit 3 (week 12) in the three treatment groups.
The tear volume measured with a strip meniscometry tube did not increase significantly in any of the groups from baseline to week 12 (Supplementary Table S1).
A similar proportion of patients in each treatment group reported that their dry eye condition was improved/very much improved. Patient-reported treatment success in the CsA, DQS, and CsA/DQS groups at week 12 was 84.0%, 81.8%, and 83.8%, respectively (P = 0.9849). Patient reports of uncomfortable sensations at 12 weeks were also comparable between groups (P = 0.4394). The most common complaint was sore or painful eyes (37.0%, 30.7%, and 37.8%, respectively; Supplementary Table S2).
The topical CsA 0.1% compliance values, measured as a percentage of CsA instilled during the study period, were 91.7% and 91.4% in the CsA and CsA/DQS groups, respectively. DQS 3% compliance values, measured as a percentage of the number of days in which DQS was instilled four or more times a day during the study period, were 88.0% and 90.2% in the DQS and CsA/DQS groups, respectively. There were no significant differences in either topical CsA 0.1% compliance or DQS tetrasodium 3% compliance between groups (P = 0.894 and P = 0.347, respectively).
Discussion
This prospective observational study compared CsA and DQS monotherapies with CsA plus DQS combination therapy in patients with mainly mild or moderate (Level I/II) DED in a real-world practice setting. All three therapies produced significant improvements from baseline to week 12 in TBUT and ocular surface fluorescein staining scores. In common with those results, a phase IV randomized clinical trial that compared the DED treatment effects of a topical CsA nanoemulsion 0.05%, topical CsA emulsion 0.05%, and DQS 3% found that all three groups improved in their combined corneal and conjunctival staining scores from baseline to week 12. 40 In addition, the trial found no significant differences in the amount of improvement in several parameters among the treatment groups, 40 in agreement with the results presented in this study that CsA and DQS monotherapy were comparable in patients with mild-to-moderate DED.
In the current study, combination therapy produced significantly larger changes in TBUT and NEI conjunctival staining in all patients compared with both monotherapies. However, the difference in level of change from baseline observed for conjunctival staining scores may have been due to heterogeneity in severity at baseline. In addition, even though there was no difference in TBUT among the three groups at baseline, TBUT in patients with short TBUT-type dry eye became longer in the CsA/DQS group than in the CsA group at week 12. It is also worth noting that, among ADDE patients, combination therapy led to significant improvement in TBUT compared with both CsA and DQS monotherapies. The observation that combination treatment produced better improvements in the signs of DED, especially in TBUT, than monotherapy, raises the possibility of potential additive effects of CsA and DQS; however, a definite conclusion cannot be drawn about the additive effects due to the significant heterogeneity in baseline characteristics, dry eye signs, and symptoms among the three arms.
In 2017, the Tear Film Ocular Society Dry Eye Workshop II advocated for a stepwise therapeutic approach depending on the etiology and disease severity, and the initiation of CsA or DQS is recommended in Step 2. 7 However, previous reports have shown that patients with mild dry eye can also derive benefit from early CsA treatment, which can delay the progression of DED severity and reduce the tissue damage caused by inflammation. 41 This study provides clinical data to suggest that early-stage DED patients can derive significant clinical benefit from the combination of a mucin secretagogue (DQS) and anti-inflammatory treatment (CsA 0.1%).
CsA is an anti-inflammatory agent that has been studied widely in DED, including ADDE and MGD. ADDE can be associated with SS and other systemic inflammatory conditions. Given the critical role of inflammation in SS, anti-inflammatory agents such as CsA are often necessary in individuals with SS-associated DED. 42 A previous study showed that topical CsA in combination with artificial tears improved tear production, conjunctival staining, and TBUT significantly better than artificial tears alone in patients with mild-to-moderate ADDE. 8 In addition, normal tears contain anti-inflammatory factors such as transforming growth factor-beta (TGF-β), which are secreted by the lacrimal gland and conjunctival goblet cells, and CsA is also known to increase goblet cell density and TGF-β levels. 43 A previous study showed that CsA treatment combined with warm compresses did more to ameliorate the clinical signs of obstructive MGD than hyaluronic acid eye drops and warm compresses. 44
Also, a prior real-world observational study showed that 8 weeks of DQS 3% treatment improved objective signs such as TBUT, ocular surface staining score, and meibum quality and expressibility. 24 Another study, evaluating the effectiveness of DQS in ADDE, showed that it produced a significant improvement in DED signs and partial improvement in symptoms. 45 Six months of DQS 3% treatment six times daily among 15 ADDE subjects with and without SS produced significant improvements in symptoms, reduced mean corneal and conjunctival staining, and increased both TBUT and tear meniscus height at all time points, compared with baseline. 45 The use of DQS 3% for more than 4 months also improved signs and symptoms in patients with obstructive MGD. 46 Whereas previous studies have revealed the effect of each monotherapy in DED, including ADDE and EDE with MGD, the current study has further compared the effects of those two monotherapies with those of combination treatment with CsA and DQS.
Interestingly, proteomic changes in human tears following topical CsA or DQS treatment of DED indicate that both treatments enhance innate and adaptive immune responses and cellular detoxification, with a protein-network analysis showing that an anti-inflammatory response was mainly responsible for the therapeutic effects of both agents. 47 However, analysis that also showed significant variances in terms of activated tear-specific biomarkers between topical CsA and DQS treatments, suggests that the two treatments use different pathways and might thus produce additive clinical effects as a combination regimen for DED. 47
In this study, each treatment was effective in improving dry eye symptom frequency and severity and patient QoL, as assessed with the SANDE and DEQS questionnaires during treatment, but the amount of improvement did not differ significantly among treatment groups. A study by Yang et al reported QoL improvements in moderate-to-severe DED treated with either DQS or topical CsA monotherapy. 48 In an observational study, DQS improved DEQS scores in patients while reading and using visual display terminals, relieving the sensation of a foreign body in the eye. 49 Based on results from the Ocular Surface Disease Index (OSDI) questionnaire, 8-weeks of DQS add-on or monotherapy significantly improved patient QoL from baseline in a recent Korean observational study. 24 In randomized trials of severe DED, a 0.1% CsA cationic emulsion administered for up to 1 year significantly improved OSDI scores, as well as signs and symptoms.11,12,50
In our study, all baseline subjective symptom scores were significantly higher in the CsA/DQS group than in the CsA and DQS monotherapy groups. Thus, even after 12 weeks of treatment, symptom scores in the CsA/DQS group were still higher than those in the monotherapy groups, although they had decreased significantly. In patients with severe dry eye symptoms who were treated for more than 12 weeks, it seems that symptom scores can be further improved by additional treatment with the combination of CsA and DQS.
In the current study, the tear volume, measured with a strip meniscometry tube, increased slightly after 4 weeks of treatment in the CsA, DQS, and CsA/DQS groups (3.18 ± 2.34, 4.24 ± 2.20, and 3.66 ± 3.08 mm, respectively) and further increased at 12 weeks (3.68 ± 2.97, 4.30 ± 2.24, and 4.11 ± 3.05 mm, respectively) compared with baseline (3.02 ± 1.95, 3.58 ± 1.58, and 3.19 ± 3.24 mm, respectively), but none of those changes in tear volume was statistically significant. To measure tear volume in this way, a strip meniscometry tube is applied to the tear meniscus for 5 s without touching the ocular surface, which does not induce reflex tearing. 51 Studies have shown that strip meniscometry is a sensitive and reliable diagnostic test for dry eye when used in conjunction with other tear function tests.51,52 However, the mean tear volume measured by a strip meniscometry tube was only 3.0 ± 1.9 mm in dry eye patients and 5.4 ± 2.2 mm in normal controls. 51 Therefore, it might be difficult to show a significant increase in tear volume using strip meniscometry, which has a relatively small measurement range.
To the best of our knowledge, this is the first study to compare the treatment effects of CsA 0.1% and DQS 3% ophthalmic solutions, and their combination, in patients with mild-to-moderate DED. However, it has some limitations, which are generally inherent in observational studies, including a lack of randomization and confounding, selection, and information biases. 53 Study assignment was not randomized, and the significant heterogeneity in the baseline values of the efficacy parameter might have introduced the risk of bias to the results Also, since the type and severity of dry eye are heterogeneous in different treatment arms, intergroup comparison is not reliable. Therefore, future studies with prospective, randomized, controlled designs are warranted to confirm the potential additive effect of the combination therapy and to elucidate its exact mechanism of action. Nevertheless, this study provides insight into the effectiveness of CsA, DQS, and their combination in patients with mild-to-moderate dry eye in a real-world setting in Korea.
Conclusions
This study found that both CsA 0.1% and DQS 3% monotherapies and CsA 0.1% plus DQS 3% combination therapy significantly improved dry eye symptoms, TBUT, and NEI corneoconjunctival staining scores from baseline to week 12 in patients with mild-to-moderate DED. In addition, the CsA/DQS combination therapy outperformed the CsA 0.1% and DQS 3% monotherapies in improving the TBUT and ocular surface staining scores. Therefore, an additional therapeutic effect in improving tear film stability and ocular surface inflammation in dry eye patients could be obtained by combining CsA 0.1% and DQS 3%.
Footnotes
Acknowledgments
The authors thank the following professors for data collection: Hung Won Tchah, University of Ulsan College of Medicine, Republic of Korea; Joon Young Hyon, Seoul National University College of Medicine, Republic of Korea; Kyoung Yul Seo, Yonsei University College of Medicine, Republic of Korea; Mee Kum Kim, Seoul National University College of Medicine, Republic of Korea; Shi Hwan Choi, Chungnam National University School of Medicine, Republic of Korea; Hong Kyun Kim, School of Medicine, Kyungpook National University, Republic of Korea; Jong Soo Lee, Pusan National University College of Medicine, Republic of Korea; Woo Chan Park, Dong-A University College of Medicine, Republic of Korea; Hyung Joon Kim, College of Medicine, Catholic University of Daegu, Republic of Korea; Sang-Bumm Lee, Yeungnam University College of Medicine, Republic of Korea; So Hyang Chung, College of Medicine, Catholic University of Korea, Republic of Korea; Jin Kwon Chung, Soonchunhyang University College of Medicine, Republic of Korea; and Eun Chul Kim, College of Medicine, Catholic University of Korea, Republic of Korea.
Under the guidance of the authors, medical writing support was provided by Robert A. Furlong, PhD, and David P. Figgitt, PhD, ISMPP CMPP™, Content Ed Net, with funding from Santen Pharmaceutical Co., Ltd., Korea.
Authors' Contributions
Y.E.: writing (lead), review and editing (equal); conceptualization (supporting); methodology (equal); and formal analysis (equal). J.S.S.: review and editing (supporting); conceptualization (supporting); methodology (equal); and formal analysis (supporting). H.M.K.: review and editing (equal); conceptualization (lead); methodology (equal); and formal analysis (equal).
Institutional Review Board Statement
This study was a part of the Health Insurance Portability and Accountability Act compliance, adhered to the tenets of the Declaration of Helsinki, and was approved by the Institutional Review Board (IRB) of each institution: Korea University Anam Hospital (IRB approval code: 2019AN0108); Asan Medical Center (2019-0446); Seoul National University Bundang Hospital (B-1905/543-405); Korea University Guro Hospital (201GR0149); Severance Hospital (4-2019-0462); Seoul National University Hospital (H1902-139-1016); Chungnam National University Hospital (2019-03-044); Kyungpook National University Hospital (2019-02-031); Pusan National University Hospital (1904-006-088); Dong-A University Hospital (DAUHIRB-19-060), Catholic University of Daegu Hospital (CR-19-039-L); Yeungnam University Hospital (YUMC 2019-04-029-001); Catholic University of Korea Seoul St. Mary's Hospital (XC1OEDI0018K); Soonchunhyang University Seoul Hospital (SCHUH 2019-03-004); Korea University Ansan Hospital (2019AS0082); and Catholic University of Korea Bucheon St. Mary's Hospital (XC19OEDI0018H).
Author Disclosure Statement
No competing financial interests exist. All authors attest that they meet the current ICMJE criteria for authorship.
Funding Information
This study was funded by Santen Pharmaceutical Co., Ltd., Korea (IKE-01).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.