
Abstract
Purpose:
To evaluate the longitudinal changes of axial length (AL) and factors associated with AL growth in myopic children receiving 0.05% atropine.
Methods:
This single-center retrospective study included children aged 4–13 years with myopia of at least −0.5 diopters (D) treated with 0.05% atropine eye drops from November 2016 to May 2021. Predictive factors for AL change were evaluated using linear mixed models.
Results:
Among 109 patients (218 eyes), 58 (53.2%) were male and the mean age at treatment was 8.5 ± 2.0 years. At baseline measurement, the mean spherical equivalent was −4.05 ± 2.34 diopters (D), and AL was 25.00 ± 0.97 mm. The mean follow-up duration was 25.4 (12–58) months, and the mean AL elongation was 0.23 ± 0.17 mm/year during the follow-up periods. AL shortening of ≥0.05 mm at subsequent visit occurred in 18 patients (26 eyes). The mean AL change in the group without initial AL shortening was statistically larger than that in the group with initial AL shortening (0.26 ± 0.16 mm/year vs. 0.02 ± 0.17 mm/year, P < 0.001). In linear mixed model, the age at atropine treatment and initial AL shortening were significantly associated with respect to AL growth (beta coefficient: −0.032 and −0.122, respectively, P < 0.001 for both).
Conclusions:
Our study found that older age and initial AL shortening are predictors of favorable response after 0.05% atropine treatment. Children with AL shortening at initial subsequent visit may be associated with good long-term response, and younger children may require higher concentration of atropine for optimal response.
Introduction
Myopia is one of the most common eye diseases in pediatric ophthalmology. 1 In children, the incidence of myopia is increasing across the globe, especially in East Asia.2,3 Since myopia is associated with excessive axial length (AL) elongation, it became a risk factor for sight-threatening complications such as retinal detachment, choroidal neovascularization, open-angle glaucoma, and cataracts. 4 Lifestyle changes are thought to be the reasons for the increasing incidence of myopia in modern society.5,6 The number of children with myopia increased as the relative percentage of time spent in outdoor activities decreased. 7 Recently, home confinement and online lectures during the coronavirus disease 2019 pandemic have been associated with the progression of myopia in children. 8 Accordingly, treatment modalities for myopia progression in children have gained more attention. 9
Atropine eye drops were first started as a treatment for myopia in 1868. 10 Evidences support the use of low-dose atropine as effective treatment in preventing myopia progression.11–14 Currently, various concentrations of atropine eye drops are prescribed to treat myopia in many countries. However, some children persistently progress to high myopia even after atropine treatment. In the Atropine for the Treatment of Myopia (ATOM) 1 study, 14% of children treated with 1% atropine had disease progression (>1 diopter [D]) in 2 years). 11 In the ATOM2 study, about 18% of children with myopia were classified as severe progressors (≥1 D in 2 years) regardless of atropine concentration. 15
Loh et al reported that younger age, parental myopia, and high degree of baseline myopia are risk factors for failure to respond to atropine, 16 whereas in the low-concentration atropine for myopia progression (LAMP) study, younger age was the only risk factor for poor response. 17 A recent study of 133 children receiving 0.01% atropine suggested that lower baseline myopia and maternal myopia were the risk factors associated with poor response. 18 It is unknown why some children do not respond to treatments to control myopia.
In this study, we investigated the longitudinal changes of AL in children with myopia who received 0.05% atropine treatment and the factors associated with AL elongation in those children.
Methods
This single-center retrospective study included children with myopia who received 0.05% atropine treatment from November 2016 to May 2021 at Gangnam Severance Hospital. This study was approved by the Institutional Review Board (IRB) and Ethics Committee of Gangnam Severance Hospital (IRB No. 3-2021-0128). The study adhered to the tenets of the Declaration of Helsinki. The 0.5mL 1% atropine eye drop (Isopto atropine, Alcon) was mixed with 9.5 mL povidone (Optagent, Samil) to prepare a 0.05% atropine solution. The low-dose atropine eye drops were instilled once every night. A total of 180 children aged between 4 and 13 years with myopic refractive error of at least −0.5 D in either eye received 0.05% low-dose atropine during the study period.
Patients with the following were excluded from the analysis: previous use of atropine, use of orthokeratology lens, or other optical methods for myopia control, those with underlying ocular diseases (e.g., cataract, inherited retinal diseases, or Stickler syndrome), previous intraocular surgery, or allergy to atropine. At the initial follow-up, 50 children were excluded due to missing follow-up (n = 36), noncompliance (n = 10), blurred near vision (n = 2), and severe photophobia (n = 2). One hundred thirty children continued using 0.05% low-dose atropine. From those, 21 children were excluded from the final analysis due to the concurrent use of orthokeratology lens (n = 10), <1 year follow-up (n = 7), less than two measurements of AL (n = 3), and previous history of retinopathy of prematurity (n = 1). Therefore, 109 children were eligible for the final analysis (Fig. 1).
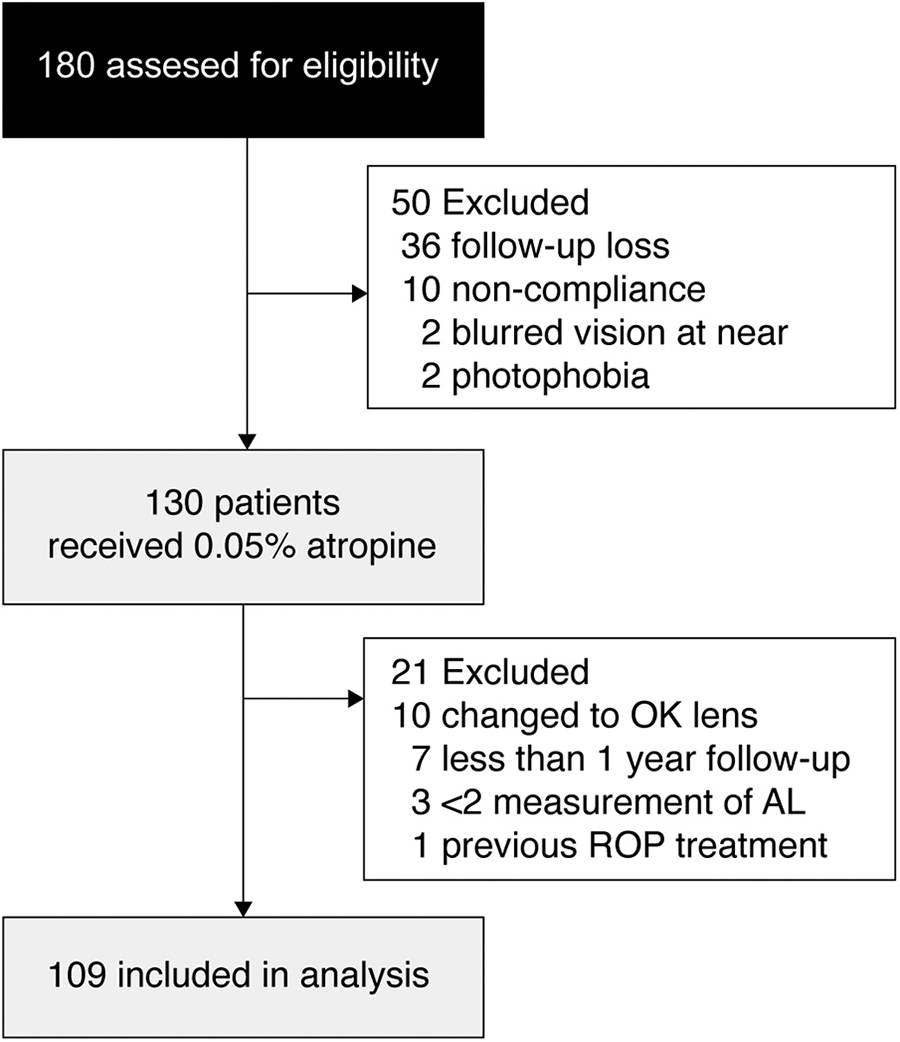
Flowchart showing participants enrolled in the 0.05% atropine treatment group. A total of 180 patients were eligible for the study; however, 50 were excluded because of follow-up misses, noncompliance, near-vision problem, and photophobia; 0.05% atropine treatment was continued in 130 patients, 21 of whom were excluded. From 180 patients eligible for the study, data of 109 children were analyzed.
Cycloplegic refraction was performed at first visit. All patients were instructed to follow-up every 4 months. However, the follow-up interval varied at each visit in most patients. The refractive errors were measured using an autorefractor (Nidek ARK-510A, Japan) without cycloplegia at subsequent visits. The AL was measured using a Zeiss IOL Master 500 (Carl Zeiss Meditec, Dublin, CA, USA) based on noncontact partial coherence interferometry. Five readings with a maximum–minimum deviation of ≤0.05 mm were taken and averaged. All measurements were done in the afternoon clinic (1:30–4:30 PM). The photopic pupil size after atropine treatment was measured using the RETeval (LKC technologies, MD, USA). Status of myopia in parents was collected based on a questionnaire. If the AL shortened (≥0.05 mm) at the subsequent follow-up after low-dose atropine treatment, then that patient was included in the initial AL shortening group.
Statistical analyses
The baseline characteristics are described as mean ± standard deviation (SD) or as proportions (%). A chi-squared test was used to evaluate the group differences of categorical data. The following factors were evaluated: (1) age at treatment, (2) initial AL shortening, (3) gender, (4) eye (5) baseline spherical equivalent (SE), (6) baseline AL, and (7) status of parental myopia. As the AL was measured repeatedly in same patients with correlated paired eye, we used the mixed effect model because it was more efficient in the presence of nonrandom missing data compared to the generalized estimating equation. 19 Statistical analyses were performed using STATA 16.1 (StataCorp LLC, College Station, TX, USA). A P < 0.05 was considered statistically significant.
Results
Among 109 children, 58 were male (53.2%), and the mean age at atropine treatment was 8.5 ± 2.0 years. The mean follow-up duration was 25.4 ± 10.9 months (range, 12–58 months). The mean baseline SE was −4.05 ± 2.34 D, and the mean baseline AL was 25.00 ± 0.97 mm. The status of parental myopia was investigated in 108 patients. Both parents of 2 children had no myopia, either parent of 47 children had myopia, and both parents of 59 children had myopia. The mean photopic pupil size after atropine treatment was 5.2 ± 0.9 mm (Table 1).
Clinical Characteristics in Children with Myopia Who Received 0.05% Atropine Treatment
AL, axial length; D, diopters; F, female; M, male; SE, spherical equivalent.
Among 109 children (i.e., 218 eyes), the mean AL elongation was 0.23 ± 0.17 mm/year. The AL shortening of ≥0.05 mm at subsequent visit after low-dose atropine treatment occurred in 18 patients (i.e., 26 eyes). The AL reduced in both eyes in 8 patients, and 10 patients had AL shortening in the unilateral eye. Among 26 eyes with initial AL shortening, the AL change was 0.02 ± 0.17 mm/year (range, 0.35 ± 0.53 mm/year), and 25 eyes were considered as responders. Only one eye in the initial AL shortening group was classified as a nonresponder (P = 0.001; Fig. 2). The mean AL change in the group without initial AL shortening was statistically larger than that in the group with initial AL shortening (0.26 ± 0.16 mm/year vs. 0.02 ± 0.17 mm/year; P < 0.001).
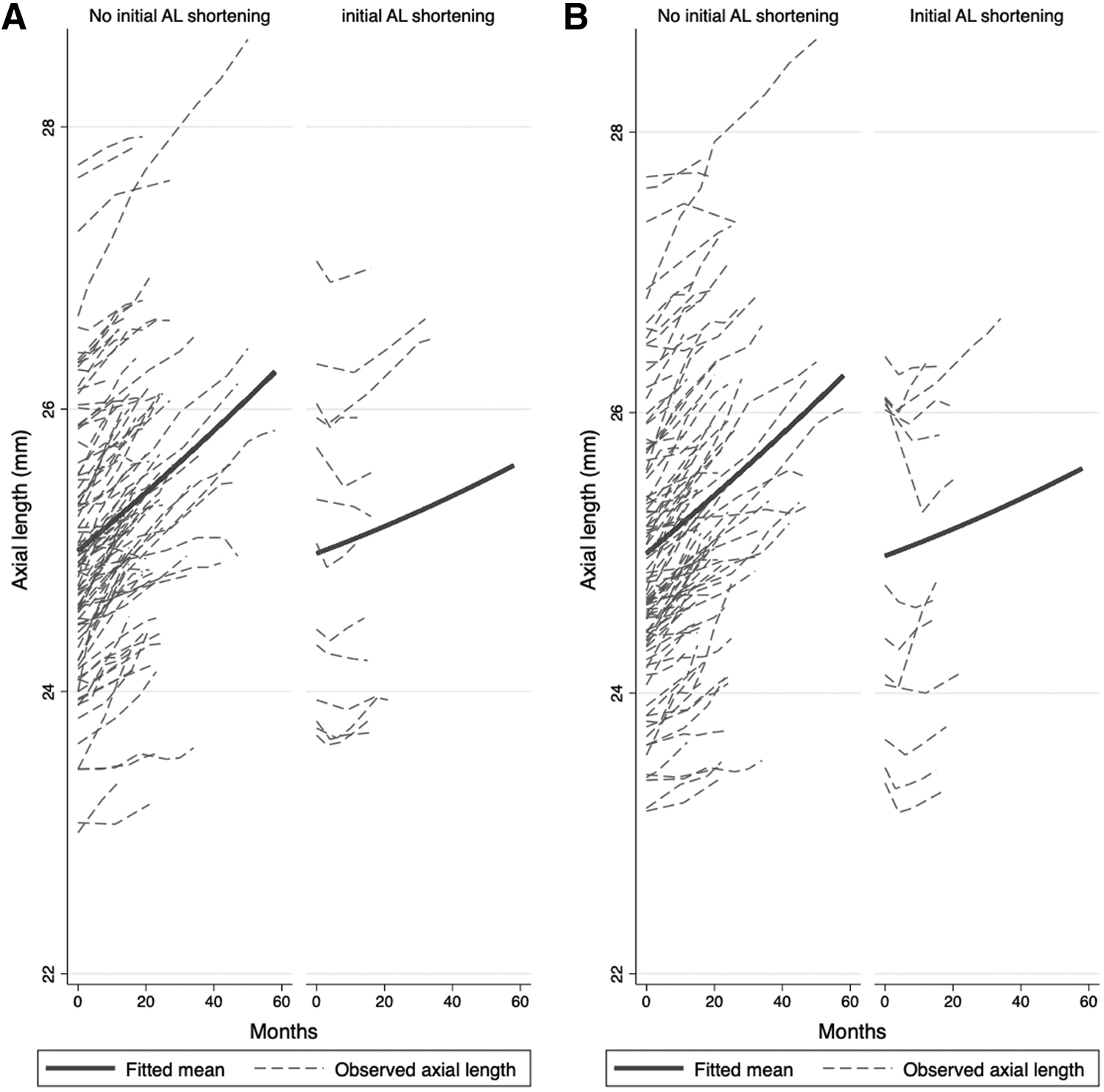
Longitudinal changes in ALs according to the initial AL shortening group.
Among 109 children, AL lengthening of ≥0.05 mm at initial follow-up visit occurred in 137 eyes. The mean AL change in the group with initial AL lengthening was statistically larger than that in children without initial AL lengthening (0.31 ± 0.15 mm vs. 0.10 ± 0.14 mm; P < 0.001).
Factors associated with AL growth
In the mixed model with random intercept and random slope, which included 108 patients (i.e., 216 eyes), the mean measurement of AL per eye was 4.3 (range, 2–8). Both, the age at atropine treatment and the initial AL shortening correlated with AL growth (beta coefficient: −0.032 and −0.122, respectively; Table 2), indicating that younger age and no initial shortening of AL after atropine treatment were associated with high probability of AL growth (all P < 0.001). Sex, eye side, baseline SE, baseline AL, and status of parental myopia did not correlate with AL growth (all P > 0.05).
Factors Associated with Axial Length Growth Among 108 Children (N = 108 Subjects, 216 Eyes, 937 Eye Visits)
Bold font indicates statistical significance.
The mixed effect with random intercept and random slope model was used.
The number of AL measurement per group (average: 4.3, minimum: 2, maximum: 8). Log likelihood = 973.45, Wald chi 2 statistics = 52066.71 (P < 0.001).
Discussion
In our study, the mean AL elongation was 0.23 ± 0.17 mm/year with 0.05% atropine treatment. Meanwhile, in the LAMP study, the mean SE change was −0.27 ± 0.61 D/year and the AL elongation was 0.20 ± 0.25 mm/year. 12 The AL changes were similar in both studies. The analysis of SE change was not included in this study because we did not perform cycloplegic refraction at every visit. Although some studies also measured SE without cycloplegia,20–22 most of previous studies evaluated SE after cycloplegia. Many sight-threatening complications related with myopia were associated with AL elongation. Retinal detachment, myopic choroidal neovascularization, or lacquer cracks occur in patients with long AL. Therefore, slowing the growth of the AL was the primary goal of myopia treatment.
In this study, older age and initial AL shortening were associated with a good response to atropine treatment. In the LAMP study, the factors associated with the changes in SE and AL over 2 years were investigated. 23 The authors also concluded that younger age was the only factor associated with SE progression and AL elongation as they found no association between AL elongation and sex, baseline SE, outdoor activity, near work, status of parental myopia, and treatment compliance.
Our results, consistent with the LAMP study, can be interpreted in several ways. It is apparent that AL elongation gradually slows down with age. Therefore, age should be considered when evaluating the effect of atropine treatment. Although the AL change per year was greater in younger children, the mean percentage of AL reduction might be the same in both younger and older children. For example, the mean AL growth was 0.9 mm/year in 6-year old control and 0.45 mm/year in 6-year old children with 0.05% atropine group. The mean AL growth was 0.6 mm/year in 9-year old control and 0.3 mm/year in 9-year old children with 0.05% atropine.
As you noted in the example, the percentage of reduction in AL growth was the same in both age group. Therefore, it may be equally effective in terms of relative efficacy of AL reduction. Otherwise, younger children may require higher concentration of atropine to get optimal responses during their exponential AL growth.
AL usually increases with age even if atropine eye drops are used. However, AL shortened after low-dose atropine treatment in some children.12,15 In our study, 18 patients (i.e., 26 eyes) had AL shortening of ≥0.05 mm at subsequent visits. Among 26 eyes with the AL shortening, 25 eyes (96.2%) showed good long-term response. The mean AL change per year was 0.02 ± 0.17 mm/year in the initial AL shortening group. This result revealed that AL growth was stable in this group and AL shortening indicated a good long-term prognosis. The mechanism regarding AL shortening after atropine treatment may be related to choroidal expansion. A previous study suggested that atropine increased choroidal thickness in children aged 6–7 years. 24 Ye et al also reported that initial choroid expansion at the 1-week visit after instillation of 1% atropine eye drops was negatively associated with long-term eye elongation. 25
They also reported that 0.01% atropine led to a decrease in the choroidal thickness and pronounced eye elongation after 6 months. Yam et al reported that low concentration atropine induced a choroidal thickening effect in a concentration-dependent manner and that choroidal thickening was associated with a slower SE progression and AL elongation. 26 An increase in choroidal thickness was also reported among children with orthokeratology lens, and the short-term increase in choroidal thickness was associated with good response in myopic progression. 27 As the choroid thickens, it moves the retinal pigment epithelium forward, causing the measured AL to shorten. Therefore, an increase in choroidal thickness could indicate a robust response after low-dose atropine treatment, explaining the association between initial AL shortening and subsequent axial elongation.
Several mechanisms have been proposed to explain how atropine causes choroidal expansion and anti-myopic progression. First, atropine eye drops causes ciliary muscle relaxation, which may allow the sclera to stretch in the equatorial meridian of the eyeball, or relaxation of nonvascular smooth muscle may allow an increase in choroidal blood flow. 28 Second, atropine could stimulate cyclic adenosine monophosphate synthesis in nitric oxide (NO)-ergic neuron because NO is necessary for choroidal thickening.29,30 Moreover, atropine may cause dopamine release in the retina, which can lead to increase in choroidal thickness. 31 Although the exact mechanism has not yet been confirmed, the muscarinic receptor that is in the sclera plays a fundamental role in remodeling. In animal studies, it was found that atropine inhibits scleral growth by acting as a nonselective antagonist of intraocular muscarinic acetylcholine receptors.32–34
The main concerns regarding low-dose atropine were its side effects. Photophobia, glare symptoms, difficulty with near work, and allergic conjunctivitis were reported. In the LAMP study, 31.2% of patients suffered photophobia at 2 weeks, which was statistically significant when compared to the rate seen in those who received the placebo. However, photophobia at 1 year was not different between the 0.05% atropine and placebo groups. 12 In our study, most patients tolerated the 0.05% atropine drops well. The discontinuation rates due to side effects were low, that is, photophobia (1.1%) and discomfort of near vision (1.1%). However, 20% of patients (36/180) did not have subsequent visits after atropine treatment, and these patients might have experienced side effects. Because long-term side effects of atropine are largely unknown, prospective studies should be conducted to investigate the effect of a dilated pupil on the development of cataract and age-related macular degeneration.
This study had some limitations. First, it was conducted retrospectively with the absence of a control group. Although the absolute AL growth was greater in younger children despite of atropine treatment, it is impossible to assess the percentage of reduction in AL growth since our study had no control group. Second, due to the limitations of its retrospective design, the status of parental myopia and photopic pupil size were not investigated in all children. Third, myopia is caused by both genetic and environmental factors. 35 It is not clear how the genetic and environmental causes respond to atropine, respectively. Although our study identified young age as a strong predictor for AL growth, we could not determine whether early onset myopia progresses more than late-onset myopia because age at treatment varied. Fourth, we could not assess several factors associated with interfering drug effect. The blinking and tearing during instillation of atropine eye drops, and simple noncompliance could be possible factors, which is more common in younger children than older children. Despite these limitations, our study showed that general trends of AL growth and factors associated with nonresponder during 0.05% atropine treatment in real-world clinical practice.
In conclusion, our study showed that older age and initial AL shortening were associated with good treatment response. Therefore, children who are young or have initial AL elongation despite 0.05% atropine may require higher concentration of atropine (>0.05%). We found that children with shortened AL at subsequent visits had favorable outcomes with atropine treatment. Pediatric ophthalmologists should bear in mind that the beneficial effect of low-dose atropine varies among children, and this should be discussed with their parents carefully. A prospective study on the natural elongation of AL in untreated children is required to determine the ideal cutoff value of AL growth for favorable outcomes with respect to their age.
Footnotes
Authors' Contributions
Data collection: H.C. and J.H. Data interpretation: H.C., Y.S., S-H.H., and J.H. Article drafting: H.C. and J.H. Critical revision of the article: H.C. and J.H. Final approval of the article: all authors.
Availability of Data and Materials
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board and the Research of Gangnam Severance Hospital (No. 3-2021-0128) and followed the stipulations of the Declaration of Helsinki. The need for informed consent was waived because of deidentified data handling and the retrospective nature of the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2020R1C1C1007965).