
Abstract
In rare cases, bisphosphonates are well established to cause ocular inflammation, presenting as uveitis, episcleritis, scleritis, orbital inflammation, and/or conjunctivitis. Some reports of bisphosphonate-associated neuro-ophthalmic complications also exist. We identified 101 reports in the literature relating to bisphosphonate-associated ocular complications. In a great majority of cases, symptoms resolve after discontinuation of the drug and anti-inflammatory treatment. Many cases recur if rechallenged with the same bisphosphonate. First-generation nonamino bisphosphonates, including clodronate and etidronate, are not associated with ocular inflammation. Only 2nd- and 3rd-generation amino bisphosphonates, including pamidronate, alendronate, risedronate, ibandronate, and zoledronate are associated with these complications. The mechanism of bisphosphonate-induced ocular inflammation may be related to activation of γ/δ T cells or M1 macrophages. Intravenous forms, such as pamidronate and zoledronate, tend to have higher rates and faster onset of ocular inflammation, generally presenting within days of infusion. In oral bisphosphonates, such as alendronate and risedronate, these complications present with more sporadic timing. Rates of complications are also higher when bisphosphonates are used for malignancy, as doses tend to be higher compared with doses for osteoporosis.
Introduction
Bisphosphonates are a class of drugs derived from inorganic phosphate that are prescribed to decrease bone resorption by osteoclasts. Patients may present taking bisphosphonates for a variety of conditions, including osteoporosis, Paget's disease, hypercalcemia, malignancy of the bone, and osteogenesis imperfecta. 1 The prevalence of osteoporosis in the U.S. adults >50 years old is estimated at 10.3%, 2 suggesting that >10 million Americans have osteoporosis. A 2012 study estimated bisphosphonate use in the United States at 26.7 per 100,000. 3
The most widely discussed adverse effect associated with bisphosphonate use is osteonecrosis of the jaw (ONJ), with an estimated incidence of 1%–15% among those being treated for malignancy, and an incidence of 0.001% to 0.01% among those being treated for osteoporosis, whose doses tend to be lower and less frequent. 4 Dental infections and dental procedures are the strongest risk factors for bisphosphonate-associated ONJ. 5
Irritation of the upper gastrointestinal tract has also been reported, including cases of esophagitis and esophageal erosion. 6 However, several reviews and trials have found no evidence of increased risk of upper gastrointestinal events when bisphosphonates are administered as instructed. 7 Other concerns related to bisphosphonate use include atrial fibrillation, severe musculoskeletal pain, hypocalcemia, renal damage, and excess suppression of bone turnover. 1
The most reported adverse effect of intravenous (IV) bisphosphonate use is an acute phase reaction. In the 2007 HORIZON clinical trial on zoledronate, 32% of patients reported a related symptom after the 1st dose, including fever, myalgia, headache, arthralgia, or influenza-like symptoms. 8 Notably, this response decreased to 7% after the 2nd dose and 3% after the 3rd. Rarely, patients may experience ocular inflammation in response to bisphosphonate use, especially anterior uveitis or periorbital inflammation with an estimated incidence between 0.046% and 1%.9–12
The acute phase reaction is commonly seen in conjunction with adverse ocular effects of bisphosphonates, and may play a role in their pathogenesis.13,14 However, the bisphosphonate-associated ocular inflammatory response typically occurs within days of administration and often results in discontinuation of the drug, hence other long-term side effects, such as ONJ, are not usually seen in conjunction with ocular inflammation.7,15 Due to the widespread use of bisphosphonates, ophthalmologists should be acutely aware of their associated ocular side effects. This article examines the ocular side effects associated with bisphosphonate therapy and explores the current understanding of their mechanism.
Method of Literature Search and Data Analysis
We conducted a literature search using PubMed, EMBASE, SCOPUS, Cochrane, and OVID/Medline in June 2022. Keywords used in our search included the following: (bisphosphonate) AND (uveitis OR iritis OR ocular inflammation OR orbital inflammation OR ocular side effects OR ocular adverse effects OR diplopia OR optic neuritis OR scleritis OR episcleritis). We also performed the same search replacing bisphosphonate with Zoledronate, Alendronate, Etidronate, Clodronate, Pamidronate, Risedronate, Ibandronate, Minodronate, Neridronate, and Tiludronate. Inclusion criteria consisted of peer-reviewed case reports, retrospective/prospective case studies, clinical trials, and reviews concerning ocular adverse effects of bisphosphonates written in English, Spanish, French, Portuguese, and German. Our initial search contained 887 articles of which 3 independent observers identified 101 that met our inclusion criteria.
When measuring the time from starting bisphosphonate therapy to an adverse reaction, many case studies gave imprecise measurements such as several hours or 3 months. In these cases, several hours were estimated at 0.25 days, and time frames given in months or years were estimated in days using 30.437 days/month and 365 days/year, respectively.
Bisphosphonate Chemistry and Pharmacology
Bisphosphonates are derived from inorganic pyrophosphate, a molecule important in many biological processes. Table 1 lists the names and route of administration of bisphosphonates prescribed worldwide, and Fig. 1 shows their structures. Neridronate is only currently approved for use in Italy, and meridronate is only approved in Japan; all other bisphosphonates are approved for use in the United States. Structurally, bisphosphonates consist of a central carbon bound to 2 phosphate groups and 2 “R groups” that are the primary determinants of drug potency. 16 For example, in etidronate (Fig. 1) the central carbon is bonded to 2 phosphonate groups, a hydroxyl group (R1), and a methyl group (R2).
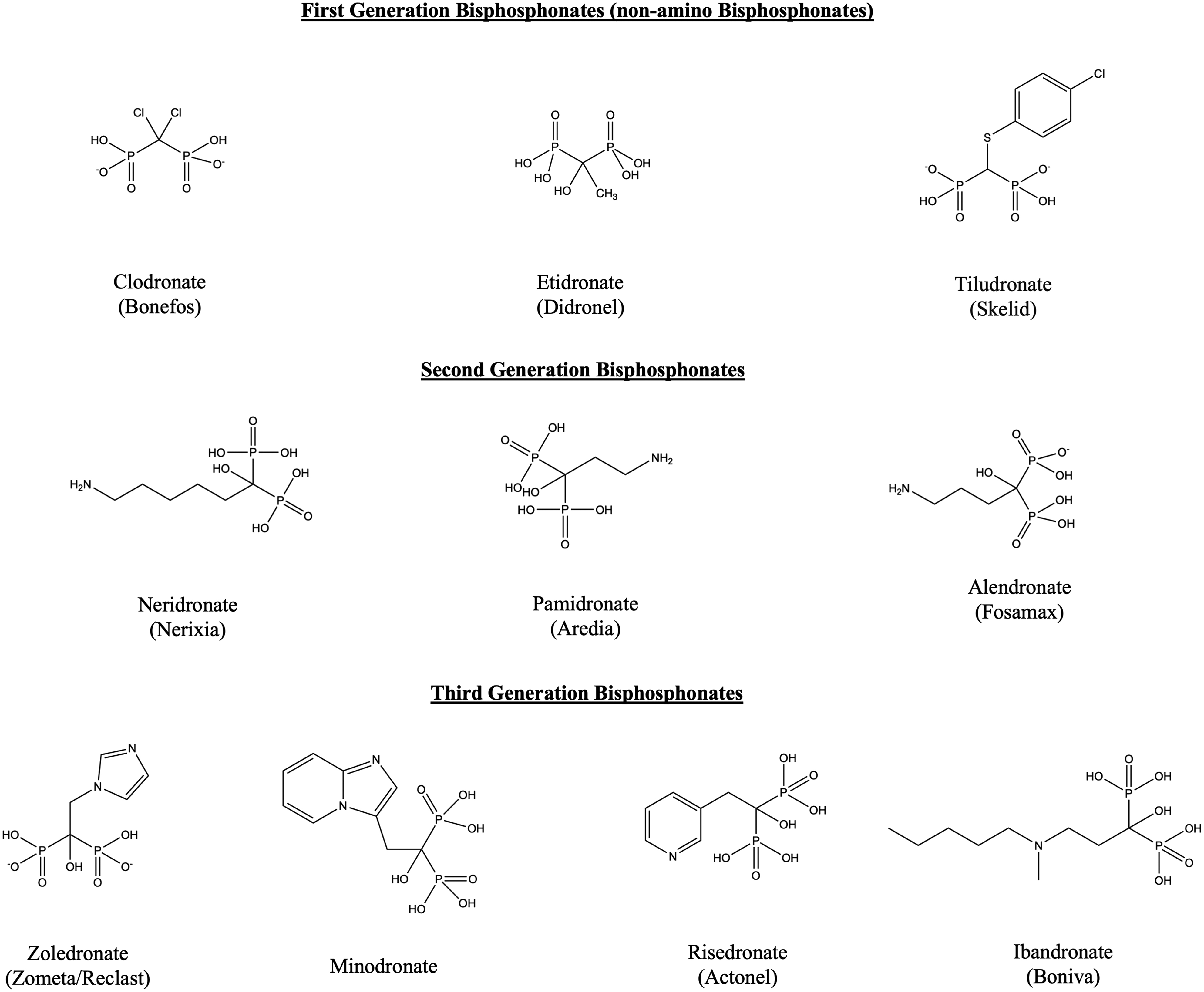
Structure of 10 bisphosphonates in clinical use around the world.
Chemical Name, Brand Name, and Route of Administration of Bisphosphonates
Notably, all 2nd- and 3rd-generation bisphosphonates (“amino bisphosphonates”) contain nitrogen in the R2 group, which greatly increases drug potency compared with 1st-generation bisphosphonates (“non-amino bisphosphonates”). 16 In addition, amino bisphosphonates inhibit farnesyl diphosphate synthase at the rate-limiting step of the mevalonate pathway, which increases the inhibition of osteoclast-mediated bone resorption compared with nonamino bisphosphonates. 17
Today, non-amino bisphosphonates are rarely prescribed because of their decreased potency and potential to inhibit bone deposition leading to osteomalacia. 17 Amino bisphosphonates are associated with an acute inflammatory response or ocular inflammation, 1 although a single case report of a non-amino bisphosphonate causing an ocular inflammatory response has been published. 18
When bisphosphonates are administered orally, such as risedronate and alendronate, ∼1% of the oral dose is absorbed and reaches systemic circulation. 1 Pamidronate and zoledronate are both administered exclusively as IV infusions. Ibandronate can be administered both orally and IV. 17 About half of the bioavailable dose binds to active bone, while the other half is renally excreted. 19 It is unclear how bisphosphonates permeate the eye, although some suggest that they may be secreted by the lacrimal gland into the tears, causing irritation of the mucous membranes. 20 It should be noted that the portion that binds bone may remain in the body for up to 10 years after administration. 1
Bisphosphonates and the Ocular Inflammatory Response
The ocular inflammatory response due to bisphosphonate therapy is well established in the literature, 21 although no causal mechanisms have yet been identified. However, numerous studies investigate the systemic inflammatory response to bisphosphonates and may guide future research to understand these mechanisms. M1 macrophage polarization, γ/δ T cell proliferation, and immune-complex deposition have been proposed as mechanisms for the immune responses seen during bisphosphonate therapy.22–24
Macrophage cells are plastic and heterogeneous but can be simplified into 2 general types, including M1 macrophages (proinflammatory) and M2 macrophages (anti-inflammatory). Disequilibrium of the ratio of M1/M2 macrophage phenotypes toward M1 macrophages is implicated in various autoimmune diseases such as systemic lupus erythematosus (SLE), 25 Behçet's syndrome, 26 rheumatoid arthritis, 24 and inflammatory bowel diseases. M1 macrophage polarization is stimulated by microbial products and proinflammatory cytokines such as TNF, IFN-γ, and Toll-like receptor (TLR) ligands. 27 It remains unknown if macrophage polarization is the primary disease process or rather the consequence of underlying pathogenic processes.
Zoledronate has been shown to induce systemic M1 macrophage polarization both in vivo 24 and in vitro. 28 The mechanism of M1 macrophage polarization in bisphosphonate therapy is poorly understood; however, results from Zhu et al suggest that zoledronate may bind to the TLR-4 receptor and contribute to M1 polarization (Fig. 2). 29 The resulting proinflammatory state is thought to contribute to the antimetastatic effects that have been observed in breast cancer patients taking bisphosphonates. 24 Many autoimmune diseases associated with M1 macrophage polarization, such as SLE and Behçet's syndrome, are also associated with an increased risk of acute anterior uveitis (AAU).30,31

Mechanisms of bisphosphonate-induced γ/δ T cell inflammation and M1 macrophage polarization.
γ/δ T cells are a subset of T cells with a distinct surface T cell receptor.23,32 Unlike the antigen-mediated response of mature B and T cells, γ/δ T cells respond to a variety of antigens, including phosphoantigens. 33 Kunzmann et al34,35 demonstrated a dose-dependent activation and proliferation of human γ/δ T cells from healthy donors and multiple myeloma patients upon exposure to amino bisphosphonates (alendronate, ibandronate, and pamidronate), and no activity upon exposure to non-amino bisphosphonates (clodronate and etidronate). Amino bisphosphonate-mediated γ/δ T cell proliferation occurs through inhibition of the rate-limiting step of cholesterol biosynthesis, which triggers an accumulation of isopentyl pyrophosphate leading to γ/δ T cell activation.23,36
The activation of γ/δ T cells releases cytokines and inflammatory mediators such as IFN-γ and IL-17A, which mediate the acute phase reaction that is commonly seen after infusion of amino bisphosphonates. 32 γ/δ T cells are also present in the ciliary body and enthesis of mice, which may contribute to the strong association between amino bisphosphonates and anterior uveitis. 37 γ/δ T cell activation and the subsequent release of cytokines 38 have also been proposed as a mechanism for orbital and ocular inflammation after bisphosphonate treatment (Fig. 2).23,32,39–41
Given the high molecular weight of bisphosphonates, immune-complex deposition has also been proposed as a component in the inflammatory response to bisphosphonates. 22 While the exact pathogenesis of bisphosphonate-induced adverse ocular effects is still unknown, it is clear that they induce a proinflammatory state by activating γ/δ T cells and by polarizing M1 macrophages. This may leave patients predisposed to inflammatory conditions more susceptible to adverse ocular effects.
Ocular Side Effects of Bisphosphonates
Bisphosphonates have been reported to cause different inflammatory ocular side effects since the early 1990s. The 1st reported case involved a 63-year-old woman with Paget's disease who presented with early symptoms of iritis 3 days after receiving risedronate in a clinical trial. The patient previously took etidronate, a non-amino bisphosphonate, with no ocular symptoms. 42
Almost all reported adverse ocular effects associated with bisphosphonates are associated with amino bisphosphonates, suggesting that the presence of nitrogen plays a role in the pathogenesis of the adverse effects. The only adverse ocular effect secondary to non-amino bisphosphonate therapy reported in the literature is one case of uveitis during clodronate therapy. 18 In this case, the reaction repeated upon each rechallenge administration of clodronate and symptoms resolved upon discontinuation of the drug. Despite the paucity of adverse ocular events associated with non-amino bisphosphonates, they are rarely prescribed due to the higher potency of the 2nd- and 3rd-generation amino bisphosphonates. 17
In the 8th edition of Drug-Induced Ocular Side Effects: Clinical Ocular Toxicology, 43 Fraunfelder et al used the WHO Causality Assessment of Suspected Adverse Reaction guide to classify bisphosphonate adverse effects into 4 categories: certain, probable, possible, and conditional/unclassified. Certain adverse ocular effects included decreased vision, transitory conjunctival side effects (lacrimation, hyperemia, pain, burning/gritty sensation, irritation, edema), photophobia, uveitis, blepharitis, scleritis, episcleritis, and visual hallucinations. Probable adverse ocular effects included orbital inflammation and edema, as well as color vision defect. Possible adverse ocular effects included optic neuritis, and conditional/unclassified adverse effects included conjunctival squamous metaplasia. 43 However, the most common side effects of bisphosphonates are predominantly inflammatory.44,45
A retrospective cohort study involving residents of British Columbia estimated the prevalence of uveitis and scleritis in bisphosphonate users at 29/10,000 and 63/10,000 person-years, respectively. 10 Prevalence among nonusers was 20/10,000 person-years for uveitis and 36/10,000 for scleritis, suggesting an increased risk of uveitis and scleritis in bisphosphonate users. However, these results are contrasted by 2 other large cohort studies.
One of these is a retrospective study of a large cohort of U.S. veterans, which estimated the risk of uveitis/scleritis within 6 months of being dispensed a bisphosphonate to be 7.9/10,000 individuals. 12 The risk of developing the conditions was not significantly greater than the general veteran population. A retrospective analysis using the Danish National Prescription database also found no significant difference in ocular inflammation between bisphosphonate users and the general population. 11
Notably, all 3 large cohort studies analyzed time frames before the introduction of zoledronate, and all found that a significant number of patients presenting with adverse ocular reactions during bisphosphonate therapy also had underlying inflammatory diseases such as rheumatoid arthritis and Sjögren's syndrome.
Table 2 summarizes the case reports of adverse ocular effects associated with bisphosphonates, including notable outcomes and decreases in visual acuity. Outcomes not included either resulted in a complete resolution of symptoms or were not included in the case report. The most common ocular adverse effects associated with bisphosphonates in our review were anterior uveitis, scleritis, and orbital inflammation. Conjunctivitis is the most common ocular side effect of bisphosphonate use overall, but it is likely under-reported in the literature because it is usually self-resolving within a few days.7,22
Summary of Bisphosphonate-Associated Ocular Side Effects
BCVA, best corrected visual acuity.
Female patients comprised 59.2% of the cases reviewed. Two large cohort studies found the percentage of men taking bisphosphonates ranges from 10.4% to 22.9%, confirming that women are prescribed bisphosphonates more often than men.10,11 However, no studies have compared the prevalence of bisphosphonate-related ocular adverse effects between male and female patients, so it remains unclear if there is any disparity based on gender.
The route of administration of bisphosphonates may affect the time it takes to develop adverse ocular effects. Among cases reviewed, adverse ocular effects typically appeared within 1–7 days of an IV infusion of zoledronate or pamidronate. Alternatively, reactions to oral doses of alendronate, risedronate, and ibandronate could manifest acutely after days of the 1st dose or after months to years of taking the drugs. This is consistent with previous findings of oral bisphosphonates showing adverse effects 15–21 days after administration, and IV bisphosphonates showing adverse effects after ∼3 days. 46
Zoledronate
Although rare, IV zoledronate has been closely associated with AAU.14,21,47–70 Two prospective, double-blind, placebo-controlled trials in postmenopausal women estimated the incidence of AAU after zoledronate therapy to be 0.8% and 1.1%.47,71 The higher prevalence of published reports of zoledronate adverse effects can be attributed to zoledronate being the most potent bisphosphonate, hence used in more severe cases of osteoporosis and in cases of malignancies. 1
Pamidronate
The side effect profile of pamidronate was similar to that of zoledronate, most likely because they are both highly potent IV infusions. Serious adverse effects associated with vision loss, such as optic neuritis72,73 and pseudotumor cerebri, 74 were also more common with these drugs. Hrabovsky et al 74 reported a case of pamidronate-induced pseudotumor cerebri confirmed by spinal tap and rechallenge that resulted in severely limited visual fields and a decrease in acuity from 6/6 OU at presentation to 6/60 OD and 6/9 OS. While these serious complications are rare, clinicians should include bisphosphonate-induced reactions in their differential diagnosis when patients taking bisphosphonates present with unusual ocular symptoms. Other ocular adverse effects associated with pamidronate are summarized in Table 2.
Alendronate and Risedronate
The oral bisphosphonates alendronate and risedronate showed similar side effects to zoledronate and pamidronate, but the time from starting the drug to adverse reaction was generally longer. One study examined inflammatory ocular events of patients taking oral bisphosphonates in Denmark, and found that 10% of patients taking bisphosphonates who received hospital treatment for uveitis had underlying rheumatoid arthritis. 11 These findings suggest that underlying inflammatory disease may be a risk factor for adverse ocular effects in patients taking oral bisphosphonates such as alendronate and risedronate. Of note, one case of alendronate-induced anterior uveitis led to corneal graft rejection and a decrease in best corrected visual acuity (BCVA) to 6/12. Table 2 summarizes other ocular effects associated with these drugs.
Ibandronate
Ibandronate was FDA approved in 2003, making it the most recent bisphosphonate to gain approval, but there are only 3 associated cases of adverse ocular effects reported in the literature. One medical letter in the Journal of Obstetrics & Gynecology noted a case of uveitis and a case of scleritis associated with ibandronate. 75 Martín Guillén et al 76 also reported a case of AAU secondary to ibandronate.
Clodronate
Clodronate is an oral and intramuscular (IM) non-amino bisphosphonate that is used extensively in patients with breast cancer. 77 As mentioned previously, only one known case was reported, which resulted in uveitis after IM administration.
Effects of Bisphosphonates on Wet Age-Related Macular Degeneration
Several studies have demonstrated dose-dependent antiangiogenic effects due to bisphosphonates,96–98 which has led some to propose the use of oral99,100 or intravitreal 101 bisphosphonates as a potential therapy or supplement for wet age-related macular degeneration (AMD).
Interestingly, hydroxyapatite spherules in the subretinal pigment epithelium are found in AMD, which may allow bisphosphonates to localize to the site of AMD.102,103 Two nonrandomized studies compared long-term oral alendronate with intravitreal anti-vascular endothelial growth factor (VEGF) injections and photodynamic therapy (PDT) in patients with myopic choroidal neovascular membranes.99,100
Miki et al found that taking oral bisphosphonates over 24 months maintained BCVA comparably with PDT, while the group that received no treatment had a significantly worse BCVA at the end of the 2-year trial. 99 The cohort that received anti-VEGF treatment had an improvement in BCVA, although this was not statistically significant compared with PDT or oral bisphosphonates. While both showed potential antiangiogenic effects in patients taking oral bisphosphonates, both studies were subject to several limitations including small sample size and lack of randomization. As neither PDT nor anti-VEGF injections are suitable for prevention of AMD, these results warrant further study as oral bisphosphonates may be useful to prevent or stop progression of early AMD.
Two studies investigated the long-term effects of bisphosphonate use on the macula due to their antiangiogenic effects. One analyzed the long-term risk of oral bisphosphonate using data from the Food and Drug Administration Adverse Event Reporting system and the British Columbia Ministry of Health Databases, and found a statistically significant, though small, increased risk of AMD in subjects regularly taking oral bisphosphonates. 104 However, the magnitude of this effect was minimal, and the study was subject to limitations. The study population only included patients visiting an ophthalmologist and used different time periods for cases versus controls.
A similar population study using data from the United Kingdom found no increased risk of AMD in a cohort of hip fracture patients, although a significantly increased risk of AMD was found in patients with a high medication possession ratio. 105 While neither study supports the use of bisphosphonates for prevention of AMD, further studies are needed to fully understand the effects of bisphosphonates in the pathophysiology of AMD.
Treatment of Ocular Side Effects
It is important to note that not all patients will present with the same side effect profile, and serious cases need to be treated adequately to prevent vision loss or long-term sequelae from inflammation. Mild reactions, such as persistent conjunctivitis, typically resolve upon drug discontinuation, but topical NSAIDs and steroids can help improve symptoms more rapidly. For more serious reactions, such as scleritis and orbital inflammation, systemic and sometimes subcutaneous or IV corticosteroids are given to reduce inflammation as quickly as possible and prevent further complications.
Cycloplegics are indicated for anterior uveitis to prevent synechiae formation, synechiolysis, and relieving pain. In some cases, patients may also consider discontinuing the offending drug if the inflammation persists. When evaluating a patient with inflammatory ocular symptoms, ophthalmologists should take a thorough medication history to better assist in clinical decision making.
Nearly all adverse ocular effects identified in our literature search were fully resolved after appropriate treatment; however, in some cases, complications persisted after treatment. One case of zoledronate-induced fibrinous iritis resulted in a uveitis-induced cataract, which was treated by phacoemulsification and intraocular lens implantation. 51 Zoledronate-induced orbital inflammation led to anterior ischemic optic neuropathy that resulted in permanent visual acuity and field deficits. 78
Another case of anterior ischemic optic neuropathy was reported secondary to giant cell arteritis associated with zoledronate, which also led to permanent loss of visual acuity and fields. 79 Surgical intervention was required for one case of zoledronate-induced uveitis that induced a persistently raised intraocular pressure 80 and a case of retinal pigment epithelial detachment associated with pamidronate therapy. 81 One case of alendronate-induced uveitis led to corneal graft rejection. 82 While most bisphosphonate-associated ocular effects are reversible, it is important that clinicians be aware of the possible side effects, so that they can be treated promptly to prevent further complications.
There is no consensus on readministering bisphosphonate therapy after an adverse ocular effect. While various case reports demonstrate a recurrence of symptoms on rechallenge,9,18,45,83–93 others demonstrated no symptoms upon rechallenge.9,50,66,94 In addition, there are reports of no adverse response after switching therapy to a different bisphosphonate68,95 or prophylactically administering corticosteroids before rechallenging with the same bisphosphonate. 64 Clinicians treating patients who have exhibited an adverse ocular effect due to bisphosphonate therapy should consider switching to a different bisphosphonate and monitoring closely for a recurrence of symptoms, or consider alternative treatments to decrease bone resorption such as denosumab.
Conclusion
Bisphosphonates are widely prescribed to decrease osteoclast-mediated bone resorption for osteoporosis and a variety of other indications. While adverse ocular events are rare with bisphosphonates, they can lead to serious ocular complications. In patients taking bisphosphonates who present with ocular inflammatory conditions, ophthalmologists should consider the inflammatory effects of bisphosphonates in their differential diagnosis.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship of this article, take responsibility for the integrity of the work, and have given final approval to the version to be published.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any author.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during this study.
Publication Originality Statement
We confirm that this publication is original.
Authors' Contribution
N.A.C. contributed to methodology, investigation, writing—original draft, data curation, visualization; C.L. and M.T.P. assisted with methodology, investigation, writing—original draft; J.J.H. performed data curation and visualization; Y.C.R. contributed to writing—editing and review, project administration; P.C.H. provided supervision; M.M. contributed to conceptualization, writing—editing and review, project administration.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by an unrestricted grant from Research to Prevent Blindness (RPB), 360 Lexington Avenue, 22nd Floor New York, NY 10017, the United States. No support was received for the publication of this article.