
Abstract
Many pharmaceutical and medical device start-up companies share similar goals. Each experience is different and offers important lessons for companies seeking Food and Drug Administration approval. This article offers important advice for budding entrepreneurs as it discusses some career-altering decisions, lessons learned in the start-up world, the technology leading up to innovation, the relevant science, medicine, chemistry, and engineering, the need to develop novel biomaterials, the regulatory path, and the business process culminating in the development of a Poly(styrene-block-isobutylene-block-Styrene)-based microshunt to treat glaucoma that led to the founding of InnFocus, Inc. (Miami, FL) in 2004, and then the acquisition of InnFocus by Santen Pharmaceuticals (Osaka, Japan) in 2016.
Introduction
Early masters
1
Third, it became apparent that the synthetic bladder (Fig. 1), comprised of synthetic ureters, a bladder reservoir, and a urethra with a valve to control incontinence, fared well in animals in the short term (days) 3 ; however, the interface of the artificial ureters (polyurethane tubes) that conducted urine to the synthetic bladder was by far the main problem with this device. The host's natural ureters, when attached to the synthetic tubes, consistently scarred over, and tissue grew into and occluded the lumens of the tubes; the result was total failure of the device. Fourth, one can design just about any replacement organ; however, interfacing it with live tissue is often the most critical part and the main source of failure.

Artificial urinary bladder.
Upon graduation with his Ph.D. the author accepted a position at Cordis Corporation (Miami Lakes, FL), a medium-sized medical device firm (≈3,000 employees) where he learned from seasoned mentors cardiovascular medical devices ranging from simple angiographic catheters to very advanced cardiac pacemakers. Also, the experience offered an education about some differences between working for a larger company versus a smaller one. The large company often takes business risks and has the resources to accomplish objectives without internal time constraints. In contrast, although there is more risk in the small company, there is usually the opportunity for more diverse work experience (as fewer people are doing all the work), a larger equity stake, and more financial upside.
Regardless of the size of the company, employment offers a financial reward in the form of salary, bonus, and possibly equity, as well as a personal reward as one builds a reputation. The reputation, which includes visibility, is perhaps the most important for the budding entrepreneur, and will become a recurring theme in this article. From personal experience, one builds an honorable reputation by accepting all proper assignments, always volunteering to assist, consistently delivering on promises, networking, publishing work and results, when possible (or allowed), and remaining always respectful of all coworkers and others.
Entrepreneurship
In 1987, Cordis' CEO, Dr. Norman Weldon, approached the author with an interesting offer to leave Cordis with him to form a start-up company called Corvita Corporation (Miami, FL). The author is often asked when does one form a start-up company? The answer is somewhat personal but; in considering the offer, he and his wife had to weigh several important factors, including (1) the downside risk if Corvita failed (this was minimal as Cordis would likely rehire him); (2) financial security for their growing family (they had two incomes and at that time two young boys with another child on the horizon); and (3) family stability and timing (children were young and the time was right to take the risk). Dr. Weldon would advise that the next opportunity to take the leap would be after the children graduate from college, as was Dr. Weldon's situation. In 1987, the author accepted the offer and left Cordis with Dr. Weldon and two other engineers (who had no children) to cofound Corvita Corporation.
In assuming the position of Vice President of Research and Development, the author was exposed to the start-up world from the ground level providing a very valuable education for his future professional path. Besides advancing the biomedical field, he gained first-hand experience in running a small company with all the attendant triumphs and challenges. For example, as a seasoned businessman (critical for a start-up), Dr. Weldon believed in a small and efficient Board of Directors comprised of only people who could raise money or who had a reputation of securing and calming investors.
The author was 33 years old then with no connections to raise money, and satisfied none of these criteria, and thus was not appointed to the Board. In his gracious effort to educate, Dr. Weldon appointed him as Corporate Secretary so he could attend Board meetings; it was there in the Board room where he learned the intricacies of raising money, executing a business plan, and dealing with venture capitalists and a Board of Directors. Far from an easy journey, the Corvita experience was a roller coaster ride of financial hardship to the point when on one occasion, the Board voted to close the company (fortunately this situation was soon reversed).
The Corvita start-up provided a valuable learning experience. It is most important when forming a company to engage people who have earned a good reputation in the business and technical fields, and who have a proven ability to raise money. The inexperienced entrepreneur simply “does not know what he/she does not know.” Isolation from others who can advise and support is the most common cause of failure for the small business. 4
Corvita secured its financing predominantly through Dr. Weldon's reputation and professional accomplishments. His prior positions as CEO of CTS Corporation (Elkart, IN), a NYSE-listed company, and then Cordis Corporation, facilitated his ability to attract venture capitalists. On the technical side, he appointed to the Board, Richard L. Kronenthal, Ph.D., a seasoned technology leader who was one of the inventors of Ethicon's Vicryl® suture. Dr. Kronenthal provided credibility to the technology, an important aspect of the financing process. The Board was then filled with venture capitalists who demanded Board seats as a prerequisite for investing in the company. And, yes, the venture capitalists were at times difficult; in one instance, they tried to force out the CEO, at which point, the author threatened to resign. Fortunately, this did not come to pass.
The mission for Corvita Corporation was to develop a small caliber (≤6 mm diameter) compliant (as in stretchy) artificial artery (vascular graft) to bypass diseased blood vessels in the body. Corvita engineers had developed a process of spinning polyurethane fibers onto a rotating mandrill; at the end of the process, a fibrous tube with controlled porosity was pulled off the mandril.
Figure 2 (left) shows a fibrous tube with a suture needle inserted; Fig. 2 (center) shows a scanning electron micrograph (SEM) of the fibrous structure of the graft in comparison with a human hair; and Fig. 2 (right) shows an SEM of the fibrous graft fibers after 1 month implantation demonstrating severe unintended biodegradation. To the Company's shock and dismay, just 1 month after formation of the company, their only product was doomed as explants confirmed that the Corvita grafts had a 100% failure rate with severe biodegradation of the material. This discovery was devastating, resulting in an initial Board vote to close the Company.

Spun polyurethane vascular graft (left). SEM of fibrous vascular graft in comparison with a human hair (center) and unintended degradation of the polyurethane fibers comprising the vascular graft at 1-month postoperative (right). SEM, scanning electron micrograph.
The Invention of the Angioplasty Balloon Catheter
By this time, the author was fascinated and captivated by the start-up world, and was not interested in returning to corporate bureaucracy—he was also highly motivated to fix the degradation problem. He was aware that angioplasty was moving to the forefront of cardiology, and that the companies practicing in the cardiovascular field, including Cordis, were using the wrong materials for these balloon catheters. They were typically using a material normally used for soda bottles called biaxially oriented polyester terephthalate (PET).
This material was certainly sufficiently strong to hold the pressure required for dilating arteries; in fact, this is why many companies were developing balloon catheters from it; however, PET is crystalline, preventing the balloon legs (top and bottom of a soda bottle) from folding down sufficiently small to be inserted through tight lesions in the blood vessel or to be delivered through small guiding catheters or small arteries. In addition, high pressure balloons made from biaxially oriented PET would often burst if scratched by a calcified lesion.
Similarly, balloons made from heat-shrink materials, as used by other inventors, had similar thick legs that could not trans-pass tight lesions. The author recognized that a totally new material was needed, and with his chemistry background knew that Nylon 12 was the perfect choice. He soon developed prototypes of his new balloon catheter and, with other engineers on his and Cordis' teams, applied for patents (which subsequently issued), describing Nylon 12 double stretch blow-molding angioplasty balloon catheters. These materials were amorphous and could be deflated to small profiles to be delivered through small catheters as well as from the radial artery in the arm; they were also scratch resistant and sufficiently compliant to dilate tapered arteries.
Corvita proposed selling the Nylon 12 technology to Cordis for upfront money and a 2% royalty. Unfortunately, Cordis took the position that the “shop rights” doctrine gave Cordis at least a no royalty license to the technology as Corvita had been renting space from Cordis and the companies often shared equipment, including the Cordis extruder that was used to make the balloon catheters. Through subsequent negotiations, Cordis agreed to pay Corvita US$300,000 over 6 months to design and fabricate the machinery used to stretch-blow-mold Nylon 12 angioplasty catheters; Cordis refused to pay any royalty to Corvita. This upfront money provided a lifeline for Corvita to fix the degradation of the polyurethanes and secure necessary financing. Several years later when Johnson and Johnson acquired Cordis, the Nylon 12 patents were valued at ∼US$800 million.
Although there were likely other factors, such as freedom to operate (Were the Nylon 12 patents infringing other patents?), influencing the Corvita CEO's decision to forego royalties on this technology, a very seasoned CEO can or may have to succumb to regrettable deals; selling the Nylon 12 patents without a royalty was truly one of those. On the contrary, this “bad deal” spurred the author to eventually start his own company. To quote him; “I can make bad deals all day long.” Note that this perspective is important as many budding entrepreneurs need to overcome their lack of self-confidence when starting their company.
The issue of “shop rights” is very important for professors and students who use university equipment to invent new products. The university can claim “shop rights” with the intention of owning the invention; it is therefore best to invent outside the institution. In the case of the professor, there is no question as employment by the university is controlled by the terms of the Employment Agreement, which will generally dictate that any inventions created during tenure are owned by the university. Students should take heed as they are not often governed by Agreements of this nature!
Nylon 12 has dominated the angioplasty market since the late 1980s and, according to Cordis engineers who police the field for infringement, is still the only material used for this application, as well as other applications, including a drug-coated balloon, as a cutting balloon, and for deploying stents. It is noteworthy that 20 U.S. patents were issued on this invention, with the first in 1990 5 and the 20th in 2002 6 ; the technology is extremely valuable, and the family was “kept alive” with continuations in part, divisional patents, and other extensions, which helped increase the value of the technology and the company.
In 2019, the author and four very influential well-known interventional cardiologists were awarded the National Academy of Engineering's Fritz and Delores Russ Prize, the world's highest prize in engineering (there is no Nobel Prize in engineering), “for innovations in medical devices that enable minimally invasive angioplasty treatment of advanced coronary artery disease.” 7 To quote the author, “We all know that Neil Armstrong was the first person on the moon, but who were the people who got him there and back safely?” The Russ Prize included at least one “engineer” who “brought them back safely.” Needless to say, the invention of this lucrative technology opened doors for the author and gave him access to a new source of investment.
The Development of a More Biostable Polyurethane
In the early 1990s, the author recognized the need for new implantable biomaterials for long-term implant. He observed that Pellethane® 2363 80A (Dow Chemicals, TX), the polyurethane used for the failed Corvita vascular graft, was the same polyurethane formulation used for insulators on pacemaker leads. It is best described as an aromatic polyether urethane (PEU). Reports of the surface cracking of these polyurethanes appeared in the literature in the late 1970s, and a comprehensive review of these polyurethanes, their degradation and suspected carcinogenicity (never proven), was published by Pinchuk in 1994. 8 He first attempted to fix the PEUs, requiring replacement of the ether group, which was known to oxidize, with a carbonate group, which was resonance stabilized and less prone to oxidation and hydrolysis.
The resultant polyurethane was an aromatic polycarbonate urethane (PCU).9–11 This PCU was substantially more biostable 12 than PEU; thereby enabling Corvita to recover from imminent failure by pursing PCU vascular grafts and then stent-grafts as their signature product lines. 13 Corvita engineers bonded this novel PCU to a self-expanding stent comprised of braided cobalt-chromium-nickel (Elgiloy®) spring wire to form a self-expanding endoluminal graft or stent-graft to bypass diseased blood vessels in the body from within the lumen of the vessel (Fig. 3).
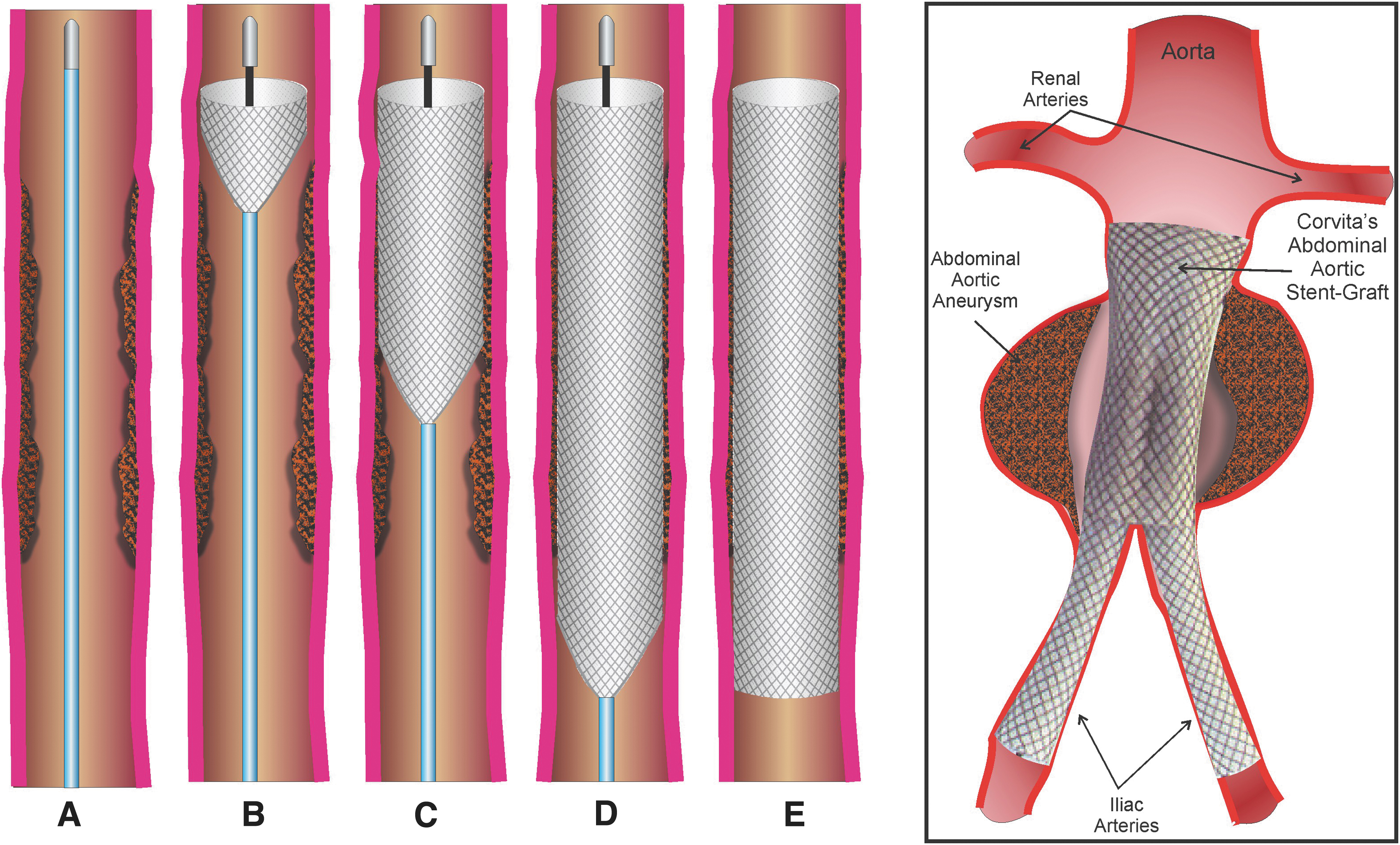
Corvita's major product soon became a bifurcated abdominal aortic stent-graft shown on the right of Fig. 3. This novel prosthesis required first placing, through a catheter, a self-expanding trunk stent-graft below the renal arteries with its distal end resting on the aortic bifurcation. This trunk stent-graft had two sockets in it for accepting two additional stent-grafts. Once the trunk was in place, two more stent-grafts were catheter deployed; one in each socket to shunt blood from the trunk to the iliac arteries feeding the legs. This abdominal aortic stent-graft served as a reinforcement for the abdominal aorta and iliac arteries.14,15 Rupture of abdominal aortic aneurysms was the 13th leading cause of death in the United States at that time, and Corvita's PCU-lined braided Elgiloy self-expanding wire stent-graft became a viable fix for these diseased arteries. Corvita also became a supplier of PCUs to the implant industry.
Corvita's Initial Public Offering
With this promising technology, the Corvita Board of Directors voted to take Corvita public in an Initial Public Offering (IPO) in 1994. At that time, Corvita was privately held; the majority of stock was held by venture capitalists whose goal was to execute a liquidity event in which they could recognize a substantial return on investment. The Board chose Pacific Growth Equity (“PGE”) to serve as investment banker to take them public. PGE purchased 25% of the Corvita stock for US$25 million, and then sold this stock on the NASDAQ stock market. Through this IPO process, Corvita received US$25 million from PGE to cover operating expenses, and in exchange PGE received all monies raised through trading Corvita stock on the open market as well as the 25% equity stake in the Company. One of the common restrictions of “going public” is that the internal shareholders cannot sell their stock for ∼6 months after the IPO.
After this successful IPO, Pfizer, Inc.,'s Schneider division in Zurich, Switzerland, acquired Corvita Corporation in 1996. However, before consummating this deal, Pfizer demanded that Corvita divest the PCU business as Pfizer had no interest in supplying biomaterials. As a result, the PCU business was sold to the Polymer Technology Group (PTG) in Berkeley, California. PTG was later acquired by DSM, a Dutch consortium located in the Netherlands, which was then acquired by Covestro AG, a former subsidiary of Bayer AG (both from Leverkusen, Germany).
Bionate®, the renamed Corvita PCU, is now a very successful biomaterial used for many implant applications, including neurostimulation, vascular applications, pacer lead insulators, artificial heart, cardiac assist, and diagnostic devices. Because of its exceptional load-bearing capability, it is also used extensively in orthopedic applications such as hip and knee joints and spinal motion preservation devices.
Unfortunately, over time, the small PCU microfibers comprising Corvita's stent-graft began to show signs of biodegradation 16 ; the author lost sleep over this and knew it was time to design a new biomaterial that would not degrade in the body. (Disclaimer: It should be noted that (1) the PCU tested was synthesized at Corvita and may not represent the formulations used by PTG, DSM, and Covestro; (2) macrophages can surround the microfiber on the stent-graft and concentrate their oxidants, thereby causing early degradation of the microfiber. This degradation may not readily occur on large surfaces, such as pacer lead insulators, as the cells cannot engulf them).
The Invention of Poly(styrene-block-isobutylene-block-Styrene) in Medicine
The realization that the PCU synthesized by Corvita, comprising the device microfibers, was not totally biostable, 16 occurred in about the mid 1990s. Fortunately, there were no failures of Corvita's devices due to biodegradation as the vascular grafts were reinforced with Dacron meshes, the stent-grafts were reinforced by a metal mesh-stent as well as the wall of the vessel in which they were placed. Nonetheless, the author was adamant that a new polymer was needed; he hypothesized that if the polymer could not degrade, had no labile pendant groups, was made extremely pure, matched the compliance of tissue, and contained chemical groups familiar to the body, it would not provoke a foreign body reaction.
This hypothesis directed his research in material development. Beginning with chemical moieties familiar to the body, he knew that the theorized polymer could not be silicone or a fluoropolymer. Although both are extremely biostable, there is no silicon or fluorine in the body, and therefore the body could recognize these materials as foreign, which could in turn elicit a chronic foreign body reaction. He also knew that there could be no unprotected hydrolyzable, oxidizable, or enzymatic cleavable groups on the polymer backbone or on its pendant groups; that is, no ester, amide, ether, carbamate, urea, or any other groups that are labile, as cleavage would both weaken the polymer as well as attract inflammatory cells.
The polymer had to be all carbon and hydrogen with predominant methyl groups interfacing tissue. Polyisobutylene (PIB) (Fig. 4) fit this model, especially because it has a dimethyl group on every second carbon. The alternating quaternary carbon and secondary carbon structure is important because double bonds cannot form on this type of backbone as carbon cannot support five bonds. Double bonds would embrittle the polymer, and cause it to crack and break in the body; this cracking has occurred with polyethylene used in knee and acetabular joints, 17 polypropylene used in intraocular lens (IOL) haptics,18,19 and the PEUs shown in Fig. 2.
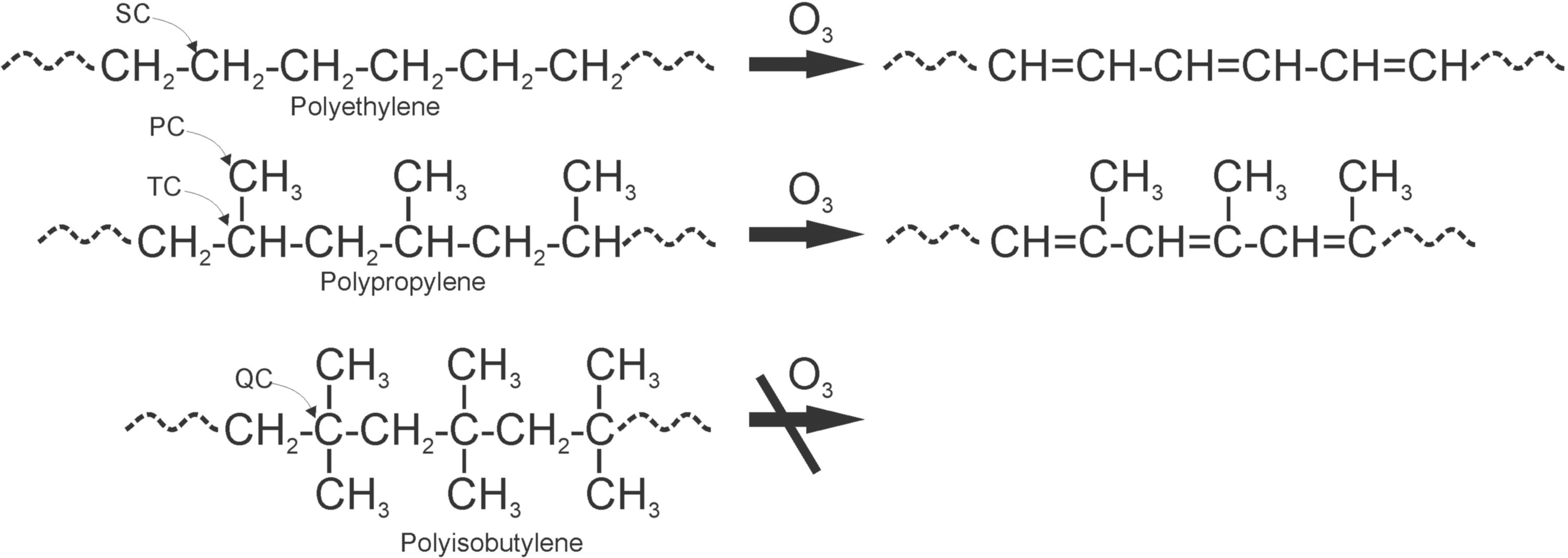
Polyethylene, polypropylene, and PIB showing PC, SC, TC, and QC and oxidation by O3 from macrophages to double bond formation. PIB cannot form double bonds as carbon cannot have five bonds, and therefore cannot oxidize. PC, primary carbons; PIB, polyisobutylene; QC, quaternary carbons; SC, secondary carbons; TC, tertiary carbons.
PIB by itself is a gum, and to convert it into a stretchable polymer, that is, an elastomer, it must be crosslinked or in the alternative, the PIB strands extended to include glassy segments, which could bind them altogether into meltable thermoplastic elastomers. The search for elastomers that contain PIB rubbery segments covalently linked to readily thermally- and/or solution-processable glassy segments pointed to Dr. Joseph P. Kennedy's laboratory at The University of Akron where such polymers were already synthesized. 20 Dr. Kennedy's patents protecting the triblock copolymer Poly(styrene-block-isobutylene-block-Styrene) (SIBS) were quickly licensed by Corvita Corporation and strengthened by additional patents covering applications in the medical implant arena.21–23
A simplified molecular structure of the triblock Poly(styrene-block-isobutylene-block-Styrene) or “SIBS” is shown in Fig. 5 in which soft PIB rubbery chains are held together by hard glassy polystyrene domains. SIBS is a self-assembled physically crosslinked PIB, and thus thermoformable and solutionformable. That is, SIBS can be extruded, injection or compression molded, and is soluble in various nonpolar solvents; it can thus be spray coated, solvent cast to deliver soft strong coherent films, or solvent bonded.
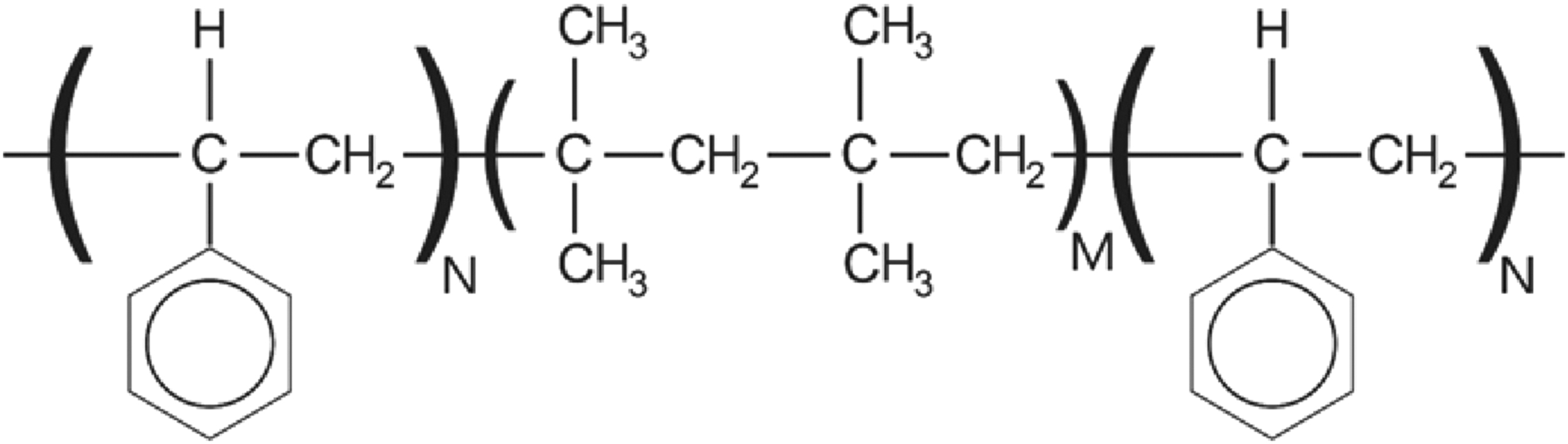
Simplistic chemical structure of “SIBS” where M is >> N. SIBS, Poly(styrene-block-isobutylene-block-Styrene).
SIBS in Cardiovascular Applications
SIBS was first tested in animal studies as a replacement for the PCU coating on Corvita's stent-graft (Fig. 3); results are published. 16 It was observed throughout the implant studies that there were usually very few, if any, polymorphonuclear leucocytes (PMN) around SIBS, which contrasts with the significant accumulation of PMNs observed around implanted polyurethanes. The results from this testing confirmed the hypothesis that a material that could not degrade, was ultrapure, matched the compliance of the tissue where implanted, and was predominantly composed of methyl groups, would provoke no clinically significant foreign body reaction.
The next step was to replace the PCU in Corvita/Schneider's vascular graft and stent-graft with SIBS. Unfortunately, Schneider management chose not to replace the PCU with SIBS, to withdraw all publications on SIBS, to the extent that no one outside of Schneider knew there was a better and more biostable polymer available. Discontinuing SIBS created a difficult situation for the author as he was very proud of the invention of SIBS in medicine, and the ability to stop biodegradation and mitigate the foreign body reaction.
In 1998, Pfizer sold its Schneider division, including Corvita, to Boston Scientific Corporation (BSCI). Consequently, the patents on SIBS in medicine,21–23 which resided in the Corvita portfolio, became the property of BSCI. Interestingly, BSCI was not aware of the SIBS asset, and in addition had no plans to develop or sell the Corvita Stent-Graft as they already had several stent-graft products about to enter the market; however, they did need the intellectual property on Corvita's abdominal aortic stent-graft at it was the first stent-graft that was assembled in the aorta. In retrospect, discontinuing the Corvita stent-graft was a blessing in disguise as the stent-graft still used the PCU material with its degradation risk.
Still preferring the small business environment, the author left BSCI/Corvita in ∼1999 to become a partner at Syntheon LLC, another Miami biomedical start-up company. Soon thereafter, he was called to attend a meeting at BSCI concerning their attempts to make a coronary stent that would release the drug “paclitaxel” into the wall of the coronary artery to stop the proliferation of smooth muscle cells that were clogging the artery. BSCI was testing, among other polymers, the author's PCU as the carrier for paclitaxel, and they were encountering an ∼100% failure rate.
After reviewing the histology, the author informed the BSCI team that the PCU was generating an inflammatory reaction due to its slow biodegradation, which was attracting PMNs and shutting down the artery. He then introduced SIBS to BSCI, and they subsequently tested the SIBS polymer in the same porcine coronary model as a stent coating; SIBS demonstrated wide patency with both an absence of neointima and PMNs at 90 and 180 days. 16 This product became BSCI's TAXUS® drug-eluting coronary stent. A comprehensive review of SIBS in TAXUS, and how the stent was designed, tested, and fine-tuned for this coronary application, is set forth in detail by Pinchuk et al. 24 The release of TAXUS was considered by Boston Scientific management to be one of the largest launches in the history of medical devices, with sales of approximately US$3 billion achieved in the first year of commercialization alone.16,24
The Formation of Innovia LLC, InnFocus LLC, and Innolene LLC and Foray into Ophthalmology
As first named inventor on the TAXUS patents25–28 and after building a SIBS pilot plant for BSCI, with the help of Corvita engineer, John B. Martin, Jr., and teaching their chemists how to synthesize SIBS, the author achieved celebrity status at BSCI. These contributions, along with the multibillion-dollar revenue stream earned by the TAXUS, placed him in an interesting position where BSCI management offered to finance his future endeavor(s), provided that (1) the venture did not compete with BSCI in cardiovascular medical devices, and (2) all association with the Syntheon partners would terminate.
It is worth reflecting on these relationships to highlight how reputation and integrity can play a paramount role in one's success. When BSCI recognized the value of SIBS, they began negotiating with the author for the rights to the material. He amusingly revealed to them that BSCI already owned the rights to SIBS as it was buried deep in the Schneider patent portfolio which they acquired when they purchased the Schneider company from Pfizer. It turned out that the SIBS patent portfolio was likely more valuable to BSCI than the rest of the Schneider technology that they acquired. In stark contrast, the Syntheon partners, who were principals in an earlier company called Symbiosis (Miami, FL), had burned bridges years earlier with BSCI management, and BSCI management refused to work with them again (a story beyond the scope of this article).
The author decided to pursue the BSCI investment offer and in 2001, formed Innovia LLC, his first personal medical device start-up company. He invited BSCI to invest US$600,000, and they countered with an investment of US$3 million. They were sufficiently savvy to understand that US$600,000 would not be adequate to develop and launch any product in the medical device arena.
Innovia later spun off as InnFocus LLC, a start-up company that developed a glaucoma device, and later as Innolene LLC, another start-up, with partners in China, to develop the next-generation IOL material made from crosslinked PIB, and an IOL made therefrom. BSCI invested >US$16 million in aggregate in the author's companies and in return asked for <20% ownership in any one of them (likely due to corporate reporting issues). They also refused a Board seat, probably for liability reasons, requesting only board observation privileges.
The process of structuring Innovia and its affiliate companies was also a learning experience aided by some very helpful advice from BSCI. The author learned that there are no inexpensive professionals; that is, one either pays up front for competent lawyers and accountants, or downstream to repair damage done by incompetent ones. In addition, whatever is done at the outset will determine success or failure at the exit, and thus it is critical to have the right people in place from inception.
All of the author's start-up companies were initially organized as individual limited liability companies (“LLC”). The rationale for forming three separate companies rather than just one company with three products, and why the LLC model was used rather than a C or S Corporation are explained as follows: Corporate structure is decided on a case-by-case basis and must be addressed as a threshold issue. (A discussion about corporate structure and organization is beyond the scope of this article, and the author is providing no legal or accounting advice herein. He is highlighting certain factors that were involved in the decision for these companies.) The LLC allows for maximum flexibility in managing and running the business, and there is no requirement for a Board of Directors (called a Board of Managers in an LLC). An unlimited number of owners or “members” are allowed, and there is no personal liability for the business. There is also flexibility to help minimize tax exposure.
The C Corporation (“C Corp”) was also a viable option, and in fact is preferred by venture capitalists and other investors. This is the best structure if there are plans to go public as the company can issue shares to founders, employees, and investors with an unlimited number of shareholders. The C Corp model is recognized internationally, and there is no personal liability for the shareholders. A downside is that this form of entity faces double taxation as the business pays at the corporate level, and the shareholders pay on personal income received. To illustrate if a C Corp sells off one product line, the company must pay tax on the value of the sale. If the proceeds are then distributed to shareholders, the shareholders must pay tax on a personal level; this is the double taxation problem.
Alternatively, if an LLC has only one product line and the entire LLC is sold, preferably >1 year after stock issuance, there is tax only at the shareholder level at a capital gains rate (lower than a corporate or regular income tax rate). In addition, the author was simultaneously developing several different and unrelated medical devices, and was not willing or able to sell them all at the same time. Logically, a company that has, for example, a sales force that calls on ophthalmologists would have no means of selling products to cardiologists. For these reasons, separate and more flexible company structures in the form of LLC's worked best in this situation.
In mid-2010, BSCI sold its ownership stake in the author's companies to a venture capital (VC) firm to raise money to acquire Guidant Corporation. Soon thereafter, the VC, as majority preferred unitholder of InnFocus LLC, demanded conversion of the LLC to a C Corporation, InnFocus, Inc., as a prerequisite for a possible sale of the company and to facilitate the handling of foreign investors who were shareholders in the VC firm. This conversion ultimately proved very beneficial for some stockholders as it enabled treatment of sale proceeds under a particular IRS/US Code Section (1202) under which capital gains on select small business stock may be excluded from federal tax requirements.
In general, if stock is held in a C Corporation for >5 years, a large portion of the proceeds from a liquidity event may be nontaxable to the noninstitutional shareholders. This is a great example of how hiring the right accountant can prove very beneficial in running a business. (Note that this IRS Rule may now possibly extend to an LLC if the LLC has elected to be taxed as a C corporation for federal tax purposes.)
Financing the start-up can be just as difficult as developing the technology. InnFocus was financed at first by BSCI, and then by the VC and numerous angel investors, and eventually by some institutional investors. It was a long road where the founder routinely presented InnFocus' product, at first called the InnFocus MicroShunt, and now called the PRESERFLO® MicroShunt (at the time of this writing, not Food and Drug Administration (FDA) approved in the United States), at ophthalmology/financial symposia, which included Morgen Stanley's Life Sciences talks in San Francisco, CA, preophthalmology congress meetings such as Glaucoma 360, New Horizons, and the Innovation Summit. Eventually, the technology became familiar to the investment community, and the first corporate investor, HOYA Corporation (Tokyo, Japan), invested significantly in the Company, followed a year later by investment and then in 2016 ultimate acquisition by Santen Pharmaceuticals (Osaka, Japan).
Santen Pharmaceuticals acquired all shares of InnFocus in 2016 and currently owns InnFocus, Inc. Approximately US$50 million was raised before acquisition, and the return on investment, although staged, can be in excess of five times the monies raised in the last round. In summary, the development of the PRESERFLO MicroShunt was an educated, iterative process that occurred over the course of 12 years.
Another lesson learned in the financial realm is that one should be very careful when working with venture capitalists (VC). The author learned the hard way that scientists who work to save lives and VCs who focus mainly on the return on their investment do not necessarily share the same perspectives. The VC's perspective can be constructive when VCs work collectively to increase the value of the company to benefit the shareholders; however, one should remember that VCs are not necessarily “your friend.” Usually by the third financing when there is a scent of a liquidity event, VCs begin to significantly influence the management, and the founding CEO is often replaced. Then with the founder removed, the Board could be reconstituted, removing the founder's Board member to be replaced by a VC Board member.
The VC and its loyalist Board member could also take control of the compensation committee and the audit committee, bringing in their own corporate lawyers. In a bad case, at the time of selling the company as an example, founding members could be surprised to discover that the loyalist Board member had given himself a huge salary, a large amount of stock options and a significant percentage of the proceeds from the sale of the Company, resulting in a major dilutive effect on the proceeds that would be distributed to company's loyal shareholders and employees who had supported the company from inception.
SIBS in Glaucoma Applications
At the time of this writing, the University of Miami's Miller School of Medicine, Bascom Palmer Eye Institute has been ranked by the U.S. News Best Hospitals 29 as the number one ophthalmology institute in the United States for the last 21 years. While a student at the University of Miami (≈1980), the author met Dr. Jean-Marie Parel, an ophthalmic physicist at the Bascom Palmer Eye Institute. The author advised Dr. Parel on the use of silicones in the eye, which Dr. Parel and his team later used as a replacement for vitreous humor after vitrectomy. Twenty years later, he worked with Dr. Parel and Dr. David Tse, an oculoplastic surgeon, on developing an orbital tissue expander to expand the orbit of babies born missing an eye (anophthalmia).
If the empty eye socket is not expanded, the face hemi-distorts as the child grows. The results of this collaboration led to a treatment for anophthalmia, and the results are published. 30 Soon thereafter, upon request of the author, Dr. Parel tested SIBS in the rabbit eye, and found that SIBS was extremely well tolerated both in the stroma of the cornea and under the conjunctiva and Tenon's capsule. The results of this testing are published by Acosta et al., 31 Fantes et al., 32 and reviewed by Pinchuk et al.16,24
These results encouraged the BPEI doctors to find a use for SIBS in ophthalmology. With the help of the late Dr. Francisco Fantes, they focused on glaucoma. Uncontrolled glaucoma is the leading cause of irreversible blindness worldwide, affecting 76 million people in 2020; this number is estimated to increase to 112 million by 2040.33,34 Glaucoma is a term describing a group of ocular disorders with multifactorial etiology, united by a clinically characteristic intraocular pressure-associated degeneration of the optic nerve, leading to blindness. 35 Data from AGIS (Advanced Glaucoma Intervention Study) suggested that intraocular pressure (“IOP”) must be reduced to the mid to low teens (≤14 mmHg) to stop the progression of vision loss. 36
The most common method to reduce IOP in the early 2000s, other than medication and laser treatments, was to shunt aqueous humor from the anterior chamber to beyond the area where the outflow is restricted. Trabeculectomy utilizes this concept. In brief, looking at Fig. 6 (left), a trapdoor is cut through a partial thickness of the sclera, the roof of the trapdoor is elevated, and a fistula is punched or trephined connecting the anterior chamber to under the trapdoor. Frequently, a section of the iris is removed to prevent it from blocking the fistula. On the right, the lid on the trapdoor is sutured closed.
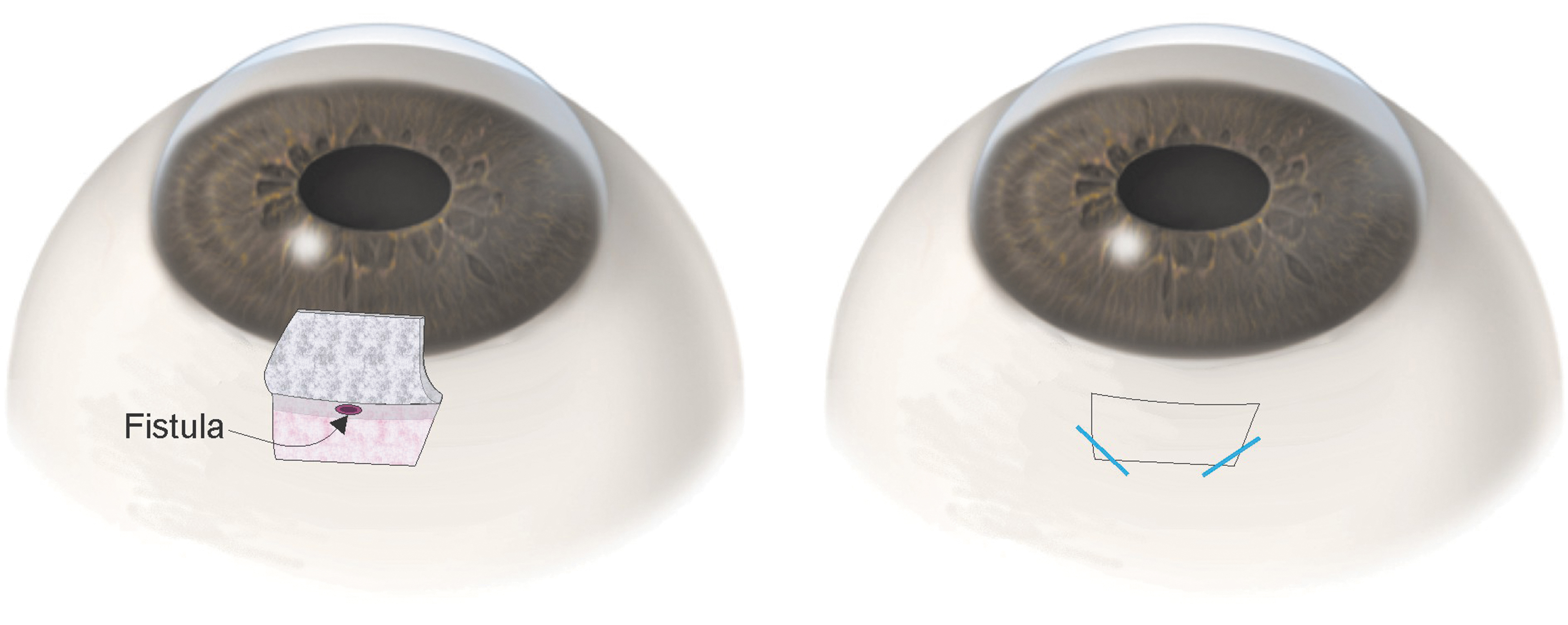
Trabeculectomy: left, trapdoor cut in the sclera and a fistula is trephined connecting the anterior chamber to under the trapdoor. Right, the lid on the trapdoor is sutured closed.
Aqueous humor drains through the fistula into the area under the trapdoor and seeps through the incisions defining the trapdoor to the extent enabled by the tension on the sutures maintaining the trapdoor closed. This procedure is subjective and difficult to teach. If too much tension is placed on the sutures, the IOP becomes too high, which will require laser suture lysis later; conversely, if too little tension, hypotony can occur. Once aqueous humor leaves the trabeculectomy, it pools into the natural space under the conjunctiva and Tenon's capsule to form a small blister-like reservoir called a bleb. 37
It was hypothesized that if a small SIBS microtube did not provoke severe inflammation and tissue encapsulation, implantation of such a tube could serve as a flow restrictor to control outflow from the eye. The length of the tube was set to 8.5 mm to drain from the anterior chamber, under the limbus and under Tenon's capsule to the mid-posterior part of the eye. A fin was added to the tube halfway down its length (Fig. 7, top), to prevent migration through the needle tract into the anterior chamber, and to serve as a “cork” to prevent fluid leakage around the tube.

The PRESERFLO MicroShunt and placement in the eye.
The lumen diameter was set to ∼70 μm; smaller lumen diameters of 50–60 μm, which were suggested by the Hagen–Poiseuille equation to prevent hypotony, were found to severely restrict flow as the surface tension of SIBS is too high to allow water to flow through the lumen at physiological pressures. SIBS is very hydrophobic with a water droplet angle of 101°. A review of the Hagen–Poiseuille equation and its implication on the PRESERFLO MicroShunt are presented by Ibarz et al. 38 The outer diameter of the tube was set at 350 μm to provide sufficient columnar strength to push the device with a forceps through the needle tract under the limbus. A series of rabbit eye implants by Arrieta et al 39 and Fantes et al 32 confirmed, before human trials, that the design and lumen diameter of 70 μm was indeed safe with no apparent hypotony issues.
Figure 7 (top) shows a schematic of the PRESERFLO MicroShunt and its placement in the eye (bottom). It required ∼5 years (2006–2011) of clinical work to optimize the design and placement of the tube, the surgical procedure, and the drug regimens used before, during, and after implantation. The first successful results of the PRESERFLO MicroShunt in the clinic were achieved by Batlle et al. with implant data now exceeding 10 years.40,41 The clinical procedure is reviewed in detail by Pinchuk et al 42 and by Sng and Barton. 37 Other peer-reviewed articles include Schlenker et al., 43 Durr et al., 44 Aptel et al., 45 Beckers et al., 46 Tanner et al., 47 Sharif et al., 48 Sadruddin et al., 49 and, in pediatric glaucoma patients, Brandt. 50
The regulatory path for a Class III implantable device like the PRESERFLO MicroShunt to be sold in the United States typically requires FDA approval through an IDE/PMA (Investigational Device Exemption/Pre-Market Approval) process. The FDA strategy should be thoroughly discussed before setting the course. The cost of an IDE/PMA is many times higher, and it can take many years longer than the 510k route; however, approval and indication of use are not guaranteed with either plan.
The 510k path seeks FDA clearance if the device is substantially equivalent to a predicate device through information gleaned from the literature or clinical trials. Having experienced both options, in the author's opinion, if the 510k route is feasible, it is advisable to follow this path to enable expeditious delivery of the product to the patient even though the downside of the 510k path is that the indication for use may be restricted to a very narrow patient population. Once available on the market, the physician–scientist consumer will often perform the necessary science, usually in retrospective clinical studies, to provide consumer confidence to expand the use of the product for other indications beyond that written on the label; however, these off-label uses cannot be endorsed by the company and may at times not be reimbursable by medical insurances.
Drainage to the mid-posterior part of the eye is relatively novel in glaucoma surgery. The bleb formed more posteriorly with the MicroShunt (and XEN gel stent 51 ) is thicker walled and potentially less prone to adverse events, as compared with the thin-walled blebs formed in the anterior Tenon's capsule adjacent to the limbus where trabeculectomy is often performed. 52 However, because Tenon's capsule is thicker in the posterior part of the eye 53 with more fibroblasts and smooth muscle cells, this placement seemingly requires a higher dose of an antiproliferation medication, such as mitomycin C (MMC, 0.4 mg/mL), to optimize outcomes. 54
On the contrary, trabeculectomy, with less fibroblasts in the anterior Tenon's, can be neutralized with only 0.2 mg/mL MMC of mitomycin C 55 ; whereas a higher dose of 0.4 mg/mL does not seem to make a difference, as suggested by the trabeculectomy arm in the Primary Tuber versus Trabeculectomy Study by Gedde et al. 56 Unfortunately, the 0.4 mg/mL MMC dose is not approved by the FDA in the United States; only the 0.2 mg/mL dose is approved.
On a similar note, when conducting a prospective randomized study against the standard of care for a procedure, as is trabeculectomy, which is considered the “gold standard” treatment for advanced glaucoma, one should consider that the investigators would be well versed in performing trabeculectomy and be in “early learning curve” when implanting the test arm. The restriction to use only 0.2 mg/mL MMC in the study arm combined with the excellent results in the trabeculectomy control group by the excellent surgeons 55 (see Gedde et al. for typical results of primary trabeculectomy) 56 may have contributed to the larger separation of end-point outcomes of trabeculectomy versus the PRESERFLO MicroShunt, than expected in the IDE/PMA prospective randomized study conducted by InnFocus. This larger separation of endpoints prevented a claim of noninferiority of the MicroShunt to trabeculectomy, which led the FDA to deny the PMA.
In several studies, the MicroShunt has lowered IOP by 30%–55% from preoperative baseline to 10–14 mmHg and significantly reduced the need for glaucoma medications, with no long-term sight-threatening adverse events.40–50 At the time of this writing, the PRESERFLO MicroShunt is approved in 33 countries worldwide, and a smaller 510k study is being conducted in the United States by Glaukos Corporation (Aliso Viejo, CA) comparing the MicroShunt with a predicate device to glean FDA clearance of the MicroShunt in the United States.
About the Author and Closing Remarks
The author grew up in an entrepreneurial home in Montreal Quebec, Canada and received a B.Sc. in Chemistry from McGill University in 1976. He then completed his master's degree in biomedical engineering in 1981, and his Ph.D. degree Interdisciplinary in Engineering and Chemistry in 1984 at the University of Miami (Miami, FL). Several times during his college years, he entertained the thought of going to medical school but did not pursue this path for two reasons: first, he wanted to treat diseases as opposed to individual patients; and second, having grown up in an entrepreneurial environment, he was more intrigued with self-governance and the financial upside of a successful business as opposed to earning income in proportion to working hours in a predetermined structure.
The entrepreneur path was a roller coaster ride. In the end, all turned out very well, and he and his teams of engineers made significant life-saving contributions to the fields of biomaterials, interventional cardiology, interventional ophthalmology, and other disciplines that use his biomaterials. In addition, it is estimated by Evercore ISI (New York, NY, 2019) that >100 million patients benefitted from his technologies, and over a hundred billion dollars of revenue were generated with many thousands of job opportunities provided throughout the worldwide industry. The roller coaster ride was filled with challenges and triumphs, and proved well worth the effort for the advancement of health care and satisfaction of an investment community.
Footnotes
Disclaimer
Any views or opinions represented in this article are personal and belong solely to the author and do not represent those of people, institutions, or organizations that the author may or may not be associated with in a professional or personal capacity.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.