
Abstract
Purpose:
To compare the effectiveness of intravitreal injections of brolucizumab and aflibercept in patients with polypoidal choroidal vasculopathy (PCV).
Methods:
In total, 62 treatment-naive PCV eyes (62 patients) treated with intravitreal brolucizumab or aflibercept were analyzed retrospectively. All patients received a monthly loading injection of antivascular endothelial growth factor for 3 months, followed by further injections as required. Visual and anatomical outcomes were compared between drugs after 12 months of treatment.
Results:
The improvement in best-corrected visual acuity after 12 months of treatment was not significantly different between the brolucizumab-treated (22 eyes) and aflibercept-treated groups (40 eyes). However, in the brolucizumab-treated group, there was a significantly greater decrease in central retinal thickness (172 vs. 147 μm; P = 0.031) and subfoveal choroidal thickness after treatment (51 vs. 29 μm; P = 0.025). In addition, the regression rate of polypoidal lesions was significantly higher in the brolucizumab-treated group (77.3%, 17/22 eyes) than that in the aflibercept-treated group (45.0%, 18/40 eyes; P = 0.014). Sterile intraocular inflammation showing mild vitritis was observed in 1 of the 22 eyes (4.5%) of brolucizumab-treated patients.
Conclusion:
Intravitreal brolucizumab injections for PCV showed visual improvement comparable to that of aflibercept during the 12-month treatment period. However, brolucizumab was more effective than aflibercept for the regression of polypoidal lesions and caused a greater decrease in central retinal thickness and subfoveal choroidal thickness.
Introduction
Age-related macular degeneration (AMD) is a leading cause of irreversible vision loss in developed countries. 1 Polypoidal choroidal vasculopathy (PCV) is considered a subtype of neovascular AMD characterized by the presence of polypoidal lesion with a branching neovascular network (BNN). 2 Most multimodal imaging studies suggest that the BNN in PCV lesions is located in a plane between the retinal pigment epithelium (RPE) and Bruch's membrane, which supports the conclusion that BNN is a type 1 macular neovascularization (MNV).3,4 Hence, PCV is also referred to as aneurysmal type 1 MNV. 4 The prevalence of PCV has been reported to be within the range of 23%–55% among newly diagnosed neovascular AMD in Asians, which is relatively higher than that in Caucasians.2,5 Currently, intravitreal antivascular endothelial growth factor (VEGF) injections, photodynamic therapy (PDT), or a combination thereof has been the standard treatment for patients with PCV.6–8
Recently, brolucizumab has been introduced and approved as a new anti-VEGF agent for the treatment of neovascular AMD. 9 The drug is a humanized, 26 kDa single-chain antibody fragment (scFv) that inhibits VEGF-A. 10 Since scFv is the smallest functional unit of antibody, brolucizumab can deliver a greater molar dose compared with other larger molecules and may effectively penetrate tissues.10,11 Recent worldwide phase 3 clinical trials, HAWK and HARRIER studies, showed that intravitreal brolucizumab was effective in improving and maintaining visual acuity for 96 weeks, which was not inferior to those of every 8 weeks dosing interval for intravitreal aflibercept. 9 Moreover, it has been reported that brolucizumab showed better effective macular fluid control, including subretinal fluid (SRF), intraretinal fluid (IRF), and sub-RPE fluid, than aflibercept. 9
Several studies have reported the therapeutic effects of brolucizumab in patients with PCV, which has shown promising results.12,13 However, there have not been sufficient reports on the differences between brolucizumab and other anti-VEGF agents for PCV-only cohorts with more than 12 months' follow-up period. This study aimed to identify the differences in the therapeutic efficacy of brolucizumab and aflibercept in the treatment of PCV.
Methods
We retrospectively screened for patients with PCV between May 2019 and December 2021 through a computerized search of the neovascular AMD database of Kim's Eye Hospital. This study conformed to the guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board of Kim's Eye Hospital, Konyang University College of Medicine. Due to the retrospective nature of this study, the need for informed consent was waived by the Institutional Review Board.
Subjects
The inclusion criteria were: (1) confirmation of active PCV with multimodal imaging, including Indocyanine Green angiography (ICGA) at the first visit; (2) no previous history of anti-VEGF treatment before the diagnosis; (3) treatment with intravitreal injections of brolucizumab (6.0 mg/0.05 mL) or aflibercept (2.0 mg/0.05 mL); and (4) a complete follow-up period of more than 12 months. This study only included patients whose ICGA revealed the presence of characteristic polypoidal structures at the border of the BNN. The presence of only polypoidal structure without BNN was also considered a PCV. Only the earlier diagnosed eye was included in the analysis if both eyes were diagnosed with PCV.
End-stage conditions at the initial diagnosis, including disciform scar or fibrosis involving fovea, were excluded from the analysis. The presence of other concomitant ocular diseases that could affect visual acuities, such as diabetic retinopathy or retinal vein occlusion, were also excluded from the analysis.
As a routine for all patients diagnosed with neovascular AMD at Kim's Eye Hospital, patients received 3-monthly anti-VEGF injections as an initial treatment. After the loading injections, the patients were followed up and retreated on a pro-re-nata (PRN; as-needed) basis. The retreatment criteria were as follows: (1) persistent macular fluid on optical coherence tomography (OCT) 1 or 2 months after the previous injection and (2) OCT evidence showing recurrence of IRF, SRF, or retinal hemorrhage. If the treating physician determined that additional treatment was required to preserve vision, the treatment was changed from a PRN regimen to a proactive regimen. Standardized examinations, including best-corrected visual acuity (BCVA), fundus examination, and spectral domain OCT [SD-OCT; consisting of 31 horizontal lines (6 × 6 mm area)], were performed at every visit for all patients. To evaluate changes in polypoidal lesions, ICGA images were taken after the initial 3 loading injections and at 12 months (or at the closest visit to 12 months if the patient was not followed up at the exact 12-month time point).
In addition to the routine follow-ups, brolucizumab-treated patients were advised to visit the clinic immediately if they experienced any symptoms associated with intraocular inflammation, such as floaters, blurred vision, scotoma, or visual field defect.
Outcome measures
The visual outcome was the mean change in BCVA [converted from Snellen BCVA to a logarithm of the minimum angle of resolution (logMAR)] from baseline to 3, 6, and 12 months. The proportion of patients gaining or losing more than 3 lines of vision from the baseline and better than 20/50 or worse than 20/200 at 12 months were also evaluated. The anatomical outcome was a mean change in central retinal and subfoveal choroidal thickness from baseline at 3, 6, and 12 months. Central retinal thickness was defined as the average thickness of the central macular 1-mm area and was automatically calculated by the OCT software. Central subfoveal choroidal thickness was defined as the distance from the outer portion of the hyperreflective line corresponding to the RPE to the hyporeflective line corresponding to the sclerochoroidal interface at the foveal center. The regression of polypoidal lesions after treatment was also evaluated by comparing ICGA images between baseline and 12 months. Polyp regression was defined as the complete disappearance of hyperfluorescence associated with polypoid lesions on ICGA images.
In addition, various baseline characteristics were analyzed, including PCV location, pattern of polypoidal lesions, baseline fluid feature, and presence of choroidal vascular hyperpermeability. The individual polyps, excluding the hypofluorescent halo measured manually, were summed to derive the total polyp area. The lesion size was measured manually, including the polypoidal lesion and BNN of the ICGA image. The pigment epithelial detachment (PED) associated with the polypoidal lesion, without underlying vascular components, was not included in the lesion size measurement.
All measurements were estimated using the in-built software of an HRA-2 machine (Heidelberg Eye Explorer, software v. 6.0.9.0; Heidelberg Engineering). The mean values from the measurements by 2 independent retinal specialists (J.W.K. and W.Y.) were used for the analysis. Whenever there was a disagreement regarding the determination of polyp regression on ICGA image between the graders, a senior specialist (H.J.C.) would determine it after an open discussion.
Statistical analyses
Data were analyzed with frequency and descriptive statistics for each variable, using SPSS software version 18.0 (SPSS, Inc., Chicago, IL). Frequencies between the groups were compared using the chi-squared or Fisher's exact test. After the normality test by Shapiro–Wilk test, comparative statistical analyses were performed with a 95% confidence interval using either Student's t-test or Mann–Whitney U test. A P-value of <0.05 was considered statistically significant.
Results
Baseline characteristics
In total, 127 eyes with PCV treated with aflibercept or brolucizumab were initially screened from the AMD database during the study period. Among them, 65 eyes were excluded for the following reasons: incomplete 12-month follow-up (19 eyes), unavailability of ICGA images at 12 months (39 eyes), retinal vein occlusion or diabetic retinopathy (2 eyes), and the presence of end-stage atrophy or scarring at baseline (5 eyes). Finally, 62 eyes (62 patients) met the eligibility criteria.
All included patients were South Korean, and the mean age of the entire study group was 67.7 ± 9.4 years. Table 1 summarizes the baseline characteristics of the patients included in the study.
Baseline Characteristics of the Patients with Polypoidal Choroidal Vasculopathy Treated Using Either Aflibercept or Brolucizumab
Statistical analysis was performed using either Student's t-test (a) or Mann–Whitney U test (b), according to the result of Shapiro–Wilk test.
Chi-square test.
Fisher's exact test.
Refers to any hemorrhage, including subretinal and sub-RPE hemorrhage, not necessarily limited to the lesion.
BCVA, best-corrected visual acuity; IRF, intraretinal fluid; logMAR, logarithm of the minimum angle of resolution; PCV, polypoidal choroidal vasculopathy; RPE, retinal pigment epithelium; SD, standard deviation; SHRM, subretinal hyperreflective material; SRF, subretinal fluid.
Among the baseline characteristics, no significant difference was found between aflibercept-treated (40 eyes) and brolucizumab-treated eyes (22 eyes) in age, gender distribution, baseline BCVA, baseline central retinal thickness, baseline subfoveal choroidal thickness, PCV location, lesion size, total polypoidal lesion area, baseline fluid feature, and incidence of choroidal vascular hyperpermeability (Table 1).
Visual outcomes
Mean BCVA showed significant improvement at 3, 6, and 12 months from baseline for both groups (Fig. 1). The mean BCVA [logMAR (Snellen equivalent)] of the aflibercept-treated group significantly improved from 0.44 ± 0.38 (20/55) to 0.34 ± 0.27 (20/43) at 12 months (P = 0.009), and that of the brolucizumab-treated group also significantly improved from 0.46 ± 0.40 (20/57) to 0.35 ± 0.28 (20/44) at 12 months after treatment (P = 0.011). However, no significant difference between the groups was found regarding the BCVA at 12 months (Table 2). In addition, there was no significant difference between the groups with respect to not only the proportion of improved or worsened BCVA more than 3 lines but also the proportion of eyes that achieved a BCVA of 20/40 or better (Table 2). The mean injection number during the 12 months of treatment was not significantly different between the groups [5.2 ± 1.8 (median, 5.0) for the aflibercept-treated group and 4.9 ± 1.7 (median, 4.5) for the brolucizumab-treated group, P = 0.443, Table 2].
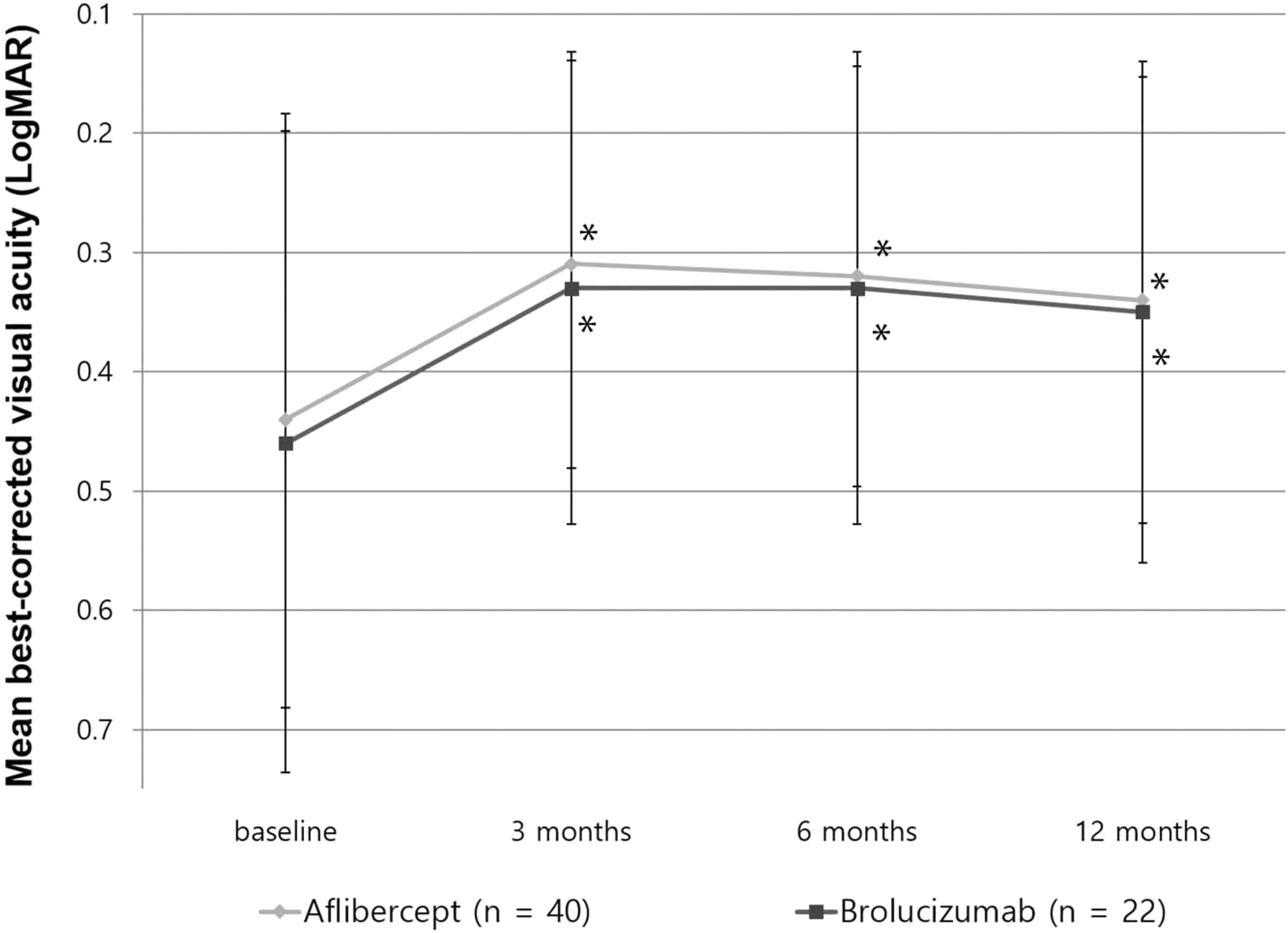
The changes in mean BCVA (expressed as the logarithm of the minimal angle of resolution) in PCV during the 12 months of treatment. The BCVA significantly improved at 3, 6, and 12 months compared with the baseline in both brolucizumab- and aflibercept-treated eyes (*P < 0.05). However, no significant difference was observed in the achieved improvement in BCVA between the 2 drugs. BCVA, best-corrected visual acuity; PCV, polypoidal choroidal vasculopathy.
Outcomes of Antivascular Endothelial Growth Factor Treatment During 12 Months for Polypoidal Choroidal Vasculopathy
Statistical analysis was performed using either Student's t-test (a) or Mann–Whitney U test (b), according to the result of Shapiro–Wilk test.
Chi-square test.
Fisher's exact test.
Anatomical outcomes
The mean central retinal thickness decreased significantly in both groups during the 12-month treatment period (Fig. 2). Although there was no significant difference regarding the central retinal thickness at 12 months between groups, the decrease in central retinal thickness from the baseline for the brolucizumab-treated group was significantly greater than that for the aflibercept-treated group (172 ± 108 μm vs. 147 ± 102 μm; P = 0.031; Table 2).
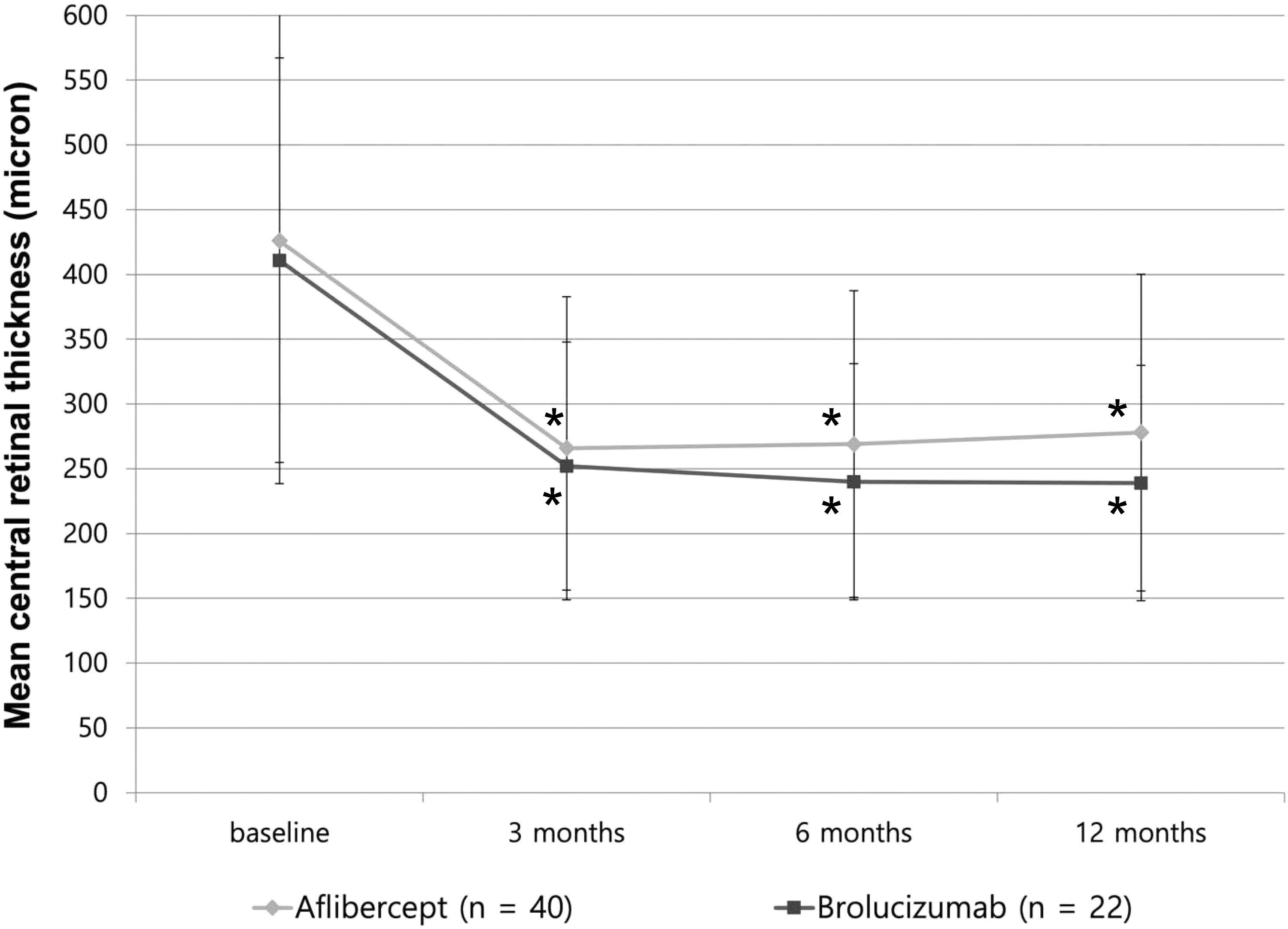
Changes in mean central retinal thickness in PCV treated with brolucizumab or aflibercept. The mean central retinal thickness significantly decreased through the 12 months of treatment with both aflibercept and brolucizumab (*P < 0.05). At 12 months, no significant difference was found in the mean central retinal thickness between the groups (P = 0.092). However, the decrease in central retinal thickness from the baseline was greater for the brolucizumab-treated group (P = 0.031).
The changes in mean subfoveal choroidal thickness in both groups were similar to the changes in central retinal thickness. The mean subfoveal choroidal thickness was significantly reduced through 12 months of treatment in both groups (Fig. 3). However, the decrease in the mean subfoveal choroidal thickness was significantly greater for the brolucizumab-treated group than that for the aflibercept-treated group (51 ± 28 μm vs. 29 ± 35 μm; P = 0.025, Table 2).
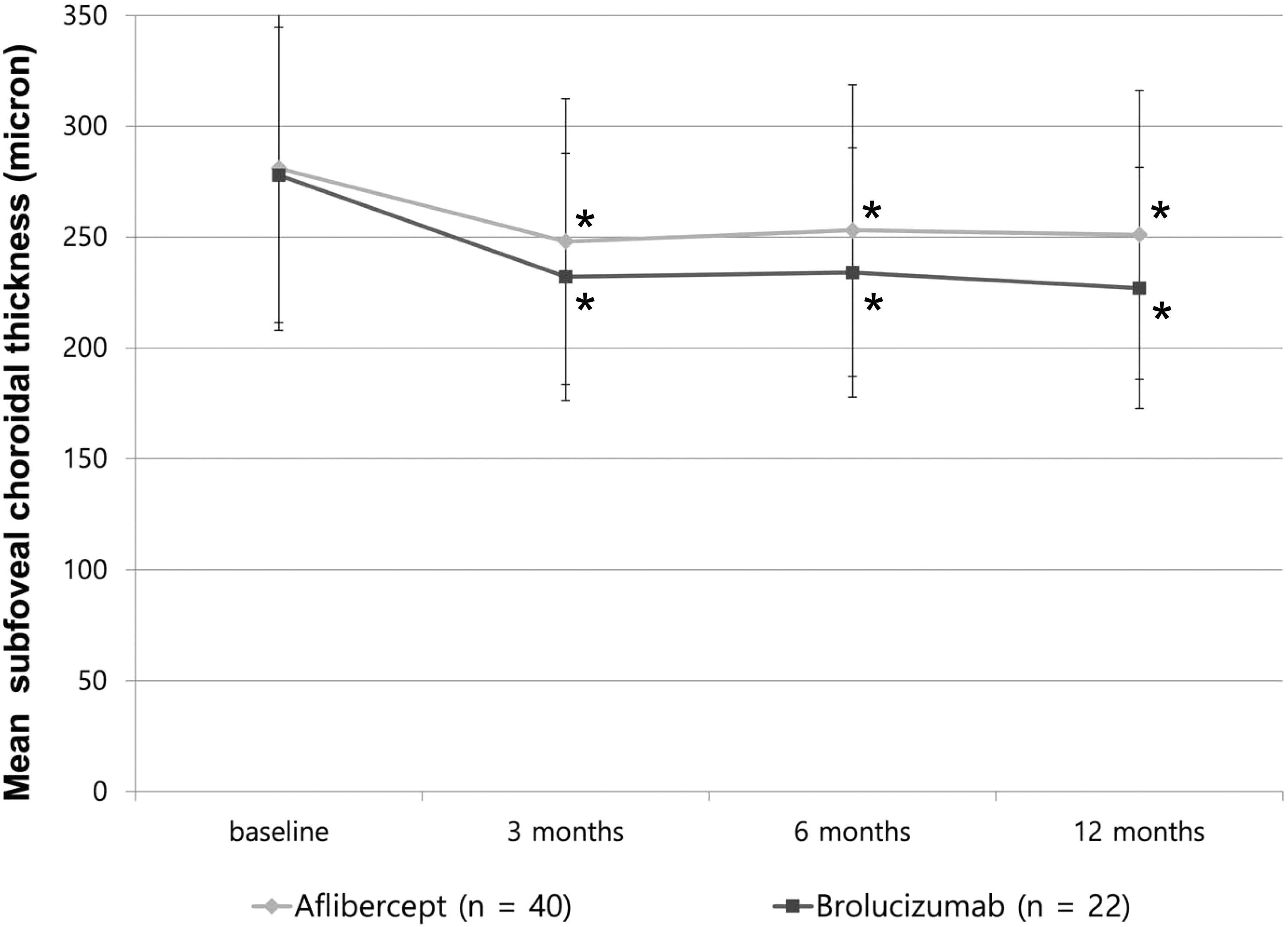
Changes in mean subfoveal choroidal thickness in PCV treated with brolucizumab or aflibercept. The mean subfoveal choroidal thickness significantly decreased through the 12 months of treatment for both aflibercept and brolucizumab (*P < 0.05). Although the mean subfoveal choroidal thickness at 12 months only showed a marginal difference between the groups (P = 0.057), the decrease in subfoveal choroidal thickness from the baseline was significantly greater for the brolucizumab-treated group (P = 0.025).
The proportion of dry macula at 12 months was not significantly different between the groups. The presence of SRF at 12 months for the brolucizumab-treated group (13.6%) tended to be less than that for the aflibercept-treated group (32.5%); however, no statistical significance was found (P = 0.104, Table 2).
The regression rate of polypoidal lesions after the treatment showed a significant difference between the groups. After the 3-monthly loading injections, the brolucizumab-treated group (81.8%; 18/22 eyes) showed more frequent regression of polypoidal lesions than the aflibercept-treated group (47.5%; 19/40 eyes) (P = 0.008). After 12 months of treatment, the regression of polypoidal lesions was still significantly higher for the eyes in the brolucizumab-treated group (77.3%; 17/22 eyes) than for those in the aflibercept-treated group (45.0%; 18/40 eyes) (P = 0.019, Table 2).
Intraocular inflammation
Noninfectious intraocular inflammation with mild vitritis was noted in 1 eye (4.5%; 1/22 eyes) in the brolucizumab-treated group. This 71-year-old woman made an unscheduled revisit to our clinic due to the floaters that developed 5 days after the third intravitreal brolucizumab injection. Mild anterior chamber inflammation was noted, and fundus examination revealed mild vitritis without retinal vasculitis. The patient was treated with a subtenon triamcinolone acetonide injection (20 mg/0.5 mL), and the inflammation resolved without any residual visual loss. After the resolution of intraocular inflammation, she had no recurrence of inflammation. She was administered 2 additional brolucizumab injections when needed during the study period without any additional adverse events. No other intraocular inflammation associated with brolucizumab, including vasculitis or retinal artery occlusion, was found in our study group. In addition, no other adverse events related to the brolucizumab or aflibercept injections, including infectious endophthalmitis, retinal detachment, or systemic adverse events, were observed in any of the subjects.
Discussion
In the current study with the PCV-only cohort, brolucizumab and aflibercept showed a similar effect in stabilizing visual acuity and decreasing central retinal thickness during a 12-month treatment period. However, there were significant differences between the drugs regarding the regression rate of polypoidal lesions and the decrease in subfoveal choroidal thickness.
The mean BCVA after the loading injection was improved by 0.11 logMAR unit in the brolucizumab-treated group (from 0.46 to 0.35; about 5.1 letters) and 0.10 logMAR unit in the aflibercept-treated group (from 0.44 to 0.34; about 5.0 letters). These visual outcomes are similar to those of a HAWK study with neovascular AMD, where 6.6 letters were gained for the brolucizumab 6.0 mg-treated group, and 6.8 letters were gained for the aflibercept 2.0 mg-treated group after 48 weeks of treatment. 14 In terms of central retinal thickness, in the HAWK study, the central subfield thickness of the brolucizumab-treated group was significantly reduced compared with the aflibercept-treated group after 48 weeks. 14 Our study with a PCV-only cohort also showed that the decrease in central retinal thickness of the brolucizumab-treated group was also greater than that of the aflibercept-treated group.
In the current study, the regression of polypoidal lesions was significantly more frequent in the brolucizumab group than in the aflibercept group. As polypoidal lesions in PCV have been thought to be the main source of the exudative change, PED development, and hemorrhagic complications, 15 many previous clinical trials regarding PCV have included the regression rate of a polypoidal lesion as a biomarker for treatment. 3 Recent studies have reported that the regression rate of polypoidal lesions after an initial 3-monthly loading injection was ∼79% for the eyes treated with brolucizumab.12,16 Our results confirmed that the higher polyp regression rate for the eyes treated with brolucizumab was sustained during the 12 months of treatment. To date, aflibercept has continuously shown its superiority in the regression of polypoidal lesions over other anti-VEGF agents, including ranibizumab and bevacizumab. 8 However, given our results regarding the regression of polypoidal lesions, brolucizumab may be more effective than aflibercept for treating patients with PCV.
PDT with verteporfin is another treatment option for PCV besides anti-VEGF. 7 Several clinical trials have shown that the combination of PDT and anti-VEGF (ranibizumab) has an advantage in the management of PCV in terms of higher regression rates of polypoidal lesions than anti-VEGF monotherapy (69.3% vs. 34.7%).6,17,18 However, it is well known that PDT has unwanted complications, such as subretinal hemorrhage or diffuse macular atrophy.19,20 Therefore, considering our result of ∼77% of polypoidal lesion regression after brolucizumab monotherapy, brolucizumab could be an effective therapeutic option with the expectation of not only stabilization of neovascularization but also higher regression of polypoidal lesions even without PDT. Future studies comparing brolucizumab and PDT for PCV management are needed.
Previous investigations have reported that aflibercept can result in a greater reduction in choroidal thickness when compared with other anti-VEGF agents, including bevacizumab or ranibizumab.21,22 However, in the current study, the choroidal thickness was greatly reduced after brolucizumab treatment than aflibercept treatment. Given that the difference in choroidal thickness reduction between anti-VEGF agents is more evident in patients with PCV compared with other types of MNV, 22 decrements in foveal thickness after brolucizumab therapy should also be confirmed for other types of neovascular AMD besides PCV in the future. The change in choroidal thickness could be an important issue because patients with thinner choroids have an increased risk of macular atrophy.23,24 Additionally, the reduction in choroidal thickness has been previously suggested to be related to suppressed disease activity in PCV eyes. 25 Further studies regarding the clinical significance of changes in choroidal thickness associated with brolucizumab treatment are needed with long-term follow-ups of more than 24 months.
It is uncertain why the anatomical outcomes such as polyp regression are different between the brolucizumab-treated and aflibercept-treated groups. This could be associated with brolucizumab's high molar concentration of the anti-VEGF agent: the molar concentration in brolucizumab is ∼11 and 22 times greater than that in aflibercept and ranibizumab, respectively. 11 Another speculation is that this result could be associated with the higher penetration of brolucizumab into the sub-RPE. Preclinical studies have shown that brolucizumab readily penetrates the retina to reach the RPE/choroid and has a better target-tissue penetration than full-sized immunoglobulin G.10,26 The precise difference and the therapeutic effect mechanisms for PCV between brolucizumab and other anti-VEGF agents should be investigated in future studies.
Noninfectious intraocular inflammation has been reported as one of the major adverse events after brolucizumab treatment for neovascular AMD. 27 The incidence has been reported to vary from 4.6% to 19%.12,27 The incidence in our study was 4.3%, which is similar to that of the post hoc analysis of a clinical trial (HAWK and HARRIER study). 27 Although the definite mechanisms have not been elucidated, some researchers have proposed that the inflammation following brolucizumab injection would be related to delayed-type hypersensitivity (type 4). 28 Another group of researchers suggested that retinal vasculitis following brolucizumab injection could be associated with type 3 hypersensitivity. 29 Furthermore, it has not been fully elucidated whether racial or ethnic differences might influence the incidence of inflammation.
To date, it has been reported that most cases of intraocular inflammation after brolucizumab injection have been successfully controlled with anti-inflammatory treatment, including topical steroids, oral steroids, or subtenon triamcinolone acetonide injections. 27 However, severe inflammations, such as branched retinal artery occlusion, if once developed, could not be recovered. 28
More than 85% of cases of intraocular inflammations reported after brolucizumab injection developed within the first 6 months of treatment initiation. 27 Therefore, a detailed explanation should be provided to all patients so as to understand the importance of seeking immediate ophthalmic examination whenever floaters or blurred vision is recognized after the injection, particularly in the early phase of the treatment. In addition, it should also be noted that there is a view that if intraocular inflammation is detected, brolucizumab treatment should be discontinued and neovascular AMD treatment resumed with another anti-VEGF agent. 30
Our study had several limitations, including its retrospective design. First, the treatment regimen was chosen at the discretion of the physician. If the study was conducted with a fixed anti-VEGF injection, as in clinical trials, our results could have been different. Second, the choice of anti-VEGF therapy for PCV was not randomized. However, at our institution, the majority of treatment-naive PCV cases from May, 2021 (when brolucizumab was introduced in South Korea) to the present were treated with brolucizumab, whereas the majority of cases before May, 2021 were treated with aflibercept. Therefore, the baseline characteristics of the 2 groups were similar and well balanced, allowing for a meaningful comparison.
In conclusion, intravitreal brolucizumab and aflibercept injections for PCV showed similar efficacy regarding improvement in visual acuity after 12 months of treatment. However, the regression rate of polypoidal lesions was significantly higher, and the decrements in subfoveal choroidal thickness and central retinal thickness were significantly greater in the brolucizumab-treated group. Further investigations are required to determine whether the differences in the effects of the 2 anti-VEGF drugs persist in the long term and whether these differences influence long-term visual outcomes.
Footnotes
Authors' Contributions
Design and conduction of the study (H.J.C.); data collection (H.J.C., K.H.K., W.Y., J.L., C.G.K., and J.W.K.); analysis and interpretation of data (H.J.C.); writing of the article (H.J.C.); critical revision and final approval of article (C.G.K. and J.W.K.).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Kim's Eye Hospital Research Center.